CNE: 1.5 contact Hours
Learning Objectives:
- Describe causes and risk factors of knee osteoarthritis (KOA), related health assessments, diagnostic tests that may be recommended by providers, and patient education needs.
- Discuss signs and symptoms of KOA and nonpharmacologic options for improved mobility and pain reduction.
- Understand pharmacologic options that providers may recommend to address KOA pain and inflammation.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 8/1/25
Takeaways:
- Knee osteoarthritis is a growing health and socio-economic concern.
- The disease progress can be successfully controlled with efficient management.
- Nurses are instrumental in controlling disease progress via patient teaching, interprofessional integration, and support.
Osteoarthritis (OA), a degenerative and inflammatory condition, can affect any joint, involves the main structures of the affected joint, and is a leading contributor of chronic pain, loss of work, and disability in the United States. The knee’s weight-bearing function creates a high risk for OA. Obesity, a growing health concern among the general population, increases the knee’s weight-bearing load and therefore the risk for OA. (See About KOA.)
About KOA
The word arthritis denotes inflammation of the joint and the surrounding tissues. Initially considered a noninflammatory condition, knee osteoarthritis (KOA) results in joint structure alteration that points to the influence of inflammation and immunological consequences. In the United States, about one in every five adults is diagnosed with KOA. According to Lespasio and colleagues, most U.S. adults age 65 or older have KOA (12.4 million), which consumes a substantial amount of healthcare resources. The estimated economic burden is more than $188 billion a year. The increasing lifelong treatment costs of KOA and potential associated disabilities and job losses impose huge financial burdens on patients and families.
According to Ackerman and colleagues, KOA incidence is on the rise, including among younger adults, with the prevalence increasing rapidly during midlife. KOA prevalence is higher among women than men, and women are more likely to experience symptoms. Blacks are affected by the condition more than Whites. Strenuous kneeling, knee-bending, squatting, prolonged standing, knee surgeries, and other traumas and injuries have been linked to a higher prevalence of symptomatic KOA.
Although chronic and degenerative, efficient management can control the rate of knee OA (KOA) progress. Understanding the condition, its causes and risk factors, appropriate health assessments and physical examinations, and diagnostic tests can help nurses advocate for the best treatment, which can include pharmacologic and nonpharmacologic modalities, interventional options such as intra-articular and extended-release steroids, and surgical options.
Causes
The main predisposing factors for KOA include age, biomechanical forces, and obesity. Other factors include gender, race and ethnicity, unhealthy diet, smoking, traumatic injury, and type 2 diabetes. These risk factors can be grouped into genetic, environmental, metabolic, and biochemical factors, which can further be described as modifiable and nonmodifiable. Nonmodifiable risk factors include hereditary (genetic mutations) and congenital (inherited abnormalities) causes.
Modifiable risk factors include obesity, trauma, biomechanical forces, biochemical reactions, and metabolic alterations. In the United States, the most common modifiable risk factors include obesity and physically demanding occupations such as farming, mining, and floor laying. Based on the evidence, obesity increases KOA risk threefold and accelerates its progression. Obesity and strenuous work cause harmful biomechanical effects on the knee. According to Lespasio and colleagues, every pound (0.45 kg) of weight gained adds 2 to 4 lbs (0.9–1.8 kg) of extra pressure on the knees.
Other modifiable risk factors include altered bone density and malalignment, occupation-related injuries, and other traumas. In addition, technological advancement has imposed work and lifestyle changes that reduce physical activity. For example, computer games that replace physical activities as well as virtual education and healthcare visits.
Systemic and local factors also play a role in KOA development. Systemic factors include oxidative damage, cartilage thinning, muscle weakening, and proprioception alteration. The basic cellular mechanisms that maintain tissue homeostasis decline with age, which can lead to an inadequate response to stress or joint injury and eventually result in joint tissue destruction. In addition, the body’s ability to repair itself decreases with age, exposing an individual to continued injury and inflammation.
Local factors related to KOA include trauma, calcium deposition, and other bone and joint disorders such as osteonecrosis; rheumatoid, gout, and septic arthritis; and Paget’s disease of the bone.
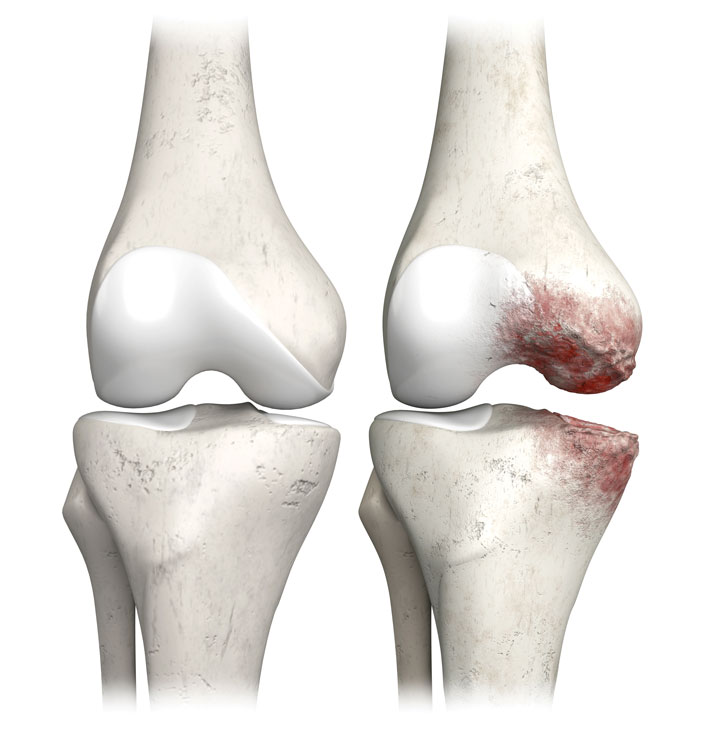
Signs and symptoms
The most common symptom of KOA is a dull or sharp pain in the joint that usually develops progressively and may be constant or intermittent. Early morning stiffness is another common symptom. Over time, painful symptoms may occur more frequently, including at night or while at rest. The main source of pain results from changes to the noncartilaginous components of the joint, such as the joint capsule, synovium, subchondral bone, ligaments, and periarticular muscles. As the condition advances, structural alterations—including bone remodeling, osteophyte formation, periarticular muscle weakening, ligament laxity, and synovial effusion—become evident on radiographs. (See Normal vs. osteoarthritic knee joint.)
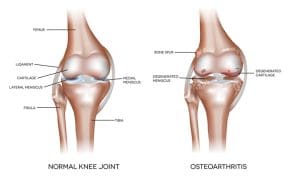
Normal vs. osteoarthritic knee joint
The knee, the largest complex hinge and synovial joint, connects three bones to compose two articulations. The distal femur and proximal tibia form the tibio-femoral joint and the distal femur and patella form the patello-femoral joint.
Other structures within the knee include meniscus and hyaline cartilages, the extra- and intracapsular ligaments, the flexor and extensor muscles that provide stability for the flexion and extension of the knee joint, and a synovial membrane that produces synovial fluid to provide lubrication and nutrients to the avascular cartilages.
Knee osteoarthritis, a heterogeneous condition, affects most of the knee structures, especially bone, cartilage, synovium, and menisci.
Other common symptoms include muscle weakness, swelling, decreased mobility, and grinding or popping sounds during movement. Pain, combined with one or more of these symptoms, results in limited knee function.
Debate exists about whether inflammation triggers osteoarthritic changes or if inflammation results from those changes. Regardless of which occurs first, most patients experience chronic low-grade inflammation, especially of the synovial membrane, in the disease’s early stages. In the advanced stages, inflammation becomes more prominent. Prolonged inflammation results in tissue destruction.
Diagnosis
Physical assessments, laboratory tests, and imaging reports aid KOA diagnosis. Begin with a detailed personal and family history followed by a thorough physical assessment. Evaluate the patient for other chronic health conditions, injuries, trauma, previous knee surgery, occupation, medications, and symptom onset (including pain character and severity).
Focus the physical examination on any deformity, tenderness, crepitus, effusion, or limitation in range of motion (passive and active). According to Vina and Kwoh, knee structure misalignment is a common risk factor for KOA. About 60% to 70% of a person’s weight-bearing load transmits medially, so any shift affects load distribution and increases knee articular stress. Also assess for misalignment and injury to the surrounding muscles, tendons, and ligaments.
Laboratory investigations include complete blood cell count with differential, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor titers, and synovial fluid evaluation. Although these test results may remain within normal limits in patients with OA, rheumatoid arthritis may result in an elevated erythrocyte sedimentation rate and elevated C-reactive protein concentration.
X-rays can help identify fractures, dislocations, and alterations in bones and joint spaces caused by cartilage loss. Other imaging studies include magnetic resonance and computed tomography to determine the condition of surrounding joint tissue.
The European Alliance of Associations for Rheumatology recommends looking for three signs (crepitus, restricted range of motion, and bony enlargement) and three symptoms (persistent pain, morning stiffness, and decreased joint function) that suggest KOA. When these six signs and symptoms are present, the radiographic report likely will indicate the presence of KOA.
Health assessment
Nurses play a vital role in helping patients manage their condition effectively. At each visit, perform a comprehensive health assessment and physical examination to help identify physical signs and symptoms and any other health problems that may interfere with the patient’s KOA diagnosis. Evidence-based patient education about self-management strategies should include discussion of exercise, weight control, and medications.
Also assess patients for the psychosocial effects of KOA, including fatigue, poor sleep, stress, anxiety, depression, social isolation, loss of work, financial difficulty, a general deterioration of quality of life, and suicidal ideation. Provide relevant education on relaxation techniques, and encourage patients to participate in social and religious activities to help manage social isolation. Advise individuals whose job inflicts biomechanical forces on the knee to consider a change of work. Provide support and resources to help them make this important decision. Depending on the extent of other psychosocial effects of KOA, provide information and encourage patients to seek appropriate mental healthcare.
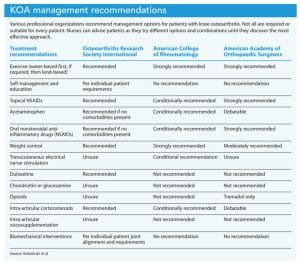
Management
The ultimate goal of KOA management is enhanced quality of life via pain control, disability minimization, and functional improvement. Interprofessional collaboration, including with physical therapy and mental health providers, can help achieve these outcomes. Several academic and professional societies (including the Osteoarthritis Research Society International, American College of Rheumatology, and American Academy of Orthopaedic Surgeons) have cooperated to establish standardized protocols that integrate multiple modalities. (See KOA management recommendations.)
Nonpharmacologic options
Nonpharmacologic management options include exercise, corrective devices, electrical stimulation, hot and cold applications, and diet.
Exercise. Because inactivity and disuse lead to rapid cartilage degeneration with deterioration of knee joint integrity and reduced joint flexibility, many professional organizations recommend exercise in the early stages of the disease. Flexibility, muscle-strengthening, and aerobic exercises, as well as weight loss, may offer relief of initial symptoms.
Recommend that patients start with light-to-moderate exercise as tolerated, and emphasize long-term adherence for the best results. All exercise should be adequately dosed and progressive. For example, water therapies may be best for patients with advanced symptoms such as increased pain, inflammation, and reduced mobility because water aids joint movement. As movement becomes easier and less painful, patients can move to land-based exercise. Help patients make these transitions based on assessment findings. (See Exercise recommendations.)
Exercise recommendations

Mounting evidence supports the efficacy of exercise to successfully control and manage knee osteoarthritis. Exercise presents minimal risk and few undesirable consequences. Many patients benefit from starting with water-based exercise, which allows easier movement of the joint.
Land-based exercise
Land-based exercises (walking, climbing stairs, cycling) help reduce joint tenderness and improve functional status and respiratory capacity. Brosseau and colleagues recommend aerobic exercises (brisk walking, running, spin cycling) as promising nonpharmacologic interventions for pain relief and to improve physical function.
Muscle-strengthening
Muscle-strengthening for the quadriceps, hip abductors, hamstrings, and calf muscles improve strength, physical function, and pain levels, with similar efficacy and outcomes to aerobic exercise.
Balance/proprioceptive exercises
This includes modalities such as Tai Chi, which combines slow, gentle movements to adopt different weight-bearing postures with breathing exercises.
Stretching
Stretching helps to improve range of motion and flexibility.
Sources: Mora et al and Brosseau et al
Corrective devices. Recommendations for patients with structural defects include appropriate footwear—braces, foot orthoses, shock-absorbent soles, arch supports, and laterally or medially wedged insoles (depending on the patient’s structural defect) to increase foot pronation and re-alignment. Although clinical efficacy of these devices is inconsistent, no evidence suggests a controversial effect. Biomechanical interventions are more effective in younger patients and those who aren’t obese.
Electrical stimulation. Transcutaneous electrical nerve stimulation (TENS) and neuromuscular electrical stimulation can provide effective pain management. TENS application occurs using gate control theory via a small, battery-powered machine in which electrodes placed over the skin on the affected area provide low-voltage electrical current. Gate control theory directs electrical impulses along nerve fibers, producing a sensation that blocks the pain signal in the brain. This mechanism relaxes and strengthens the muscles around the knee, easing pain sensations. To ease any patient anxiety, explain the procedure and its effects.
Hot and cold applications. Heat enhances circulation to ease stiff joints, and cold packs relieve inflammation and reduce pain. Depending on the application the provider chooses (based on the individual patient’s symptoms), offer education to ensure safe use.
Diet. Unhealthy diets can contribute to KOA and its symptoms. Consuming any food that contains high amounts of salt, fat, and sugar leads to increased production of inflammatory cytokines and promotes inflammation. Unhealthy diets can speed the progression of inflammatory diseases, including OA. Evidence suggests that diets featuring fruits, vegetables, whole grains, and certain spices (including turmeric and ginger) may help reduce inflammation.
Pharmacologic options
In addition to exercise and other nonpharmacologic interventions, analgesics and anti-inflammatory drugs may be required if pain and inflammation persist. The most commonly used medications include acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, viscosupplementation with hyaluronic acid injections, glucosamine, and platelet-rich plasma (PRP) therapies. However, to avoid adverse effects (including liver injury related to prolonged use of acetaminophen), providers should limit these medications to short-term (2-week) use. Common NSAID side effects include heartburn, nausea and vomiting, bleeding and ulcers, hypertension, and allergic reactions. However, NSAIDs’ anti-inflammatory properties make them highly effective.
If these pharmacologic options prove ineffective, opioids may be prescribed. Small doses of tramadol are reported to have less risk of respiratory depression compared to other opioids and may be considered for short-term use.
Many patients with KOA may be elderly and have multiple comorbidities. Assess for contraindications and drug interactions to any pharmacologic modalities.
Immediate-release cortisone therapy. The Food and Drug Administration approved immediate-release corticosteroid injections (such as methylprednisolone acetate, triamcinolone acetate, triamcinolone hexacetonide, betamethasone acetate, betamethasone sodium phosphate, or dexamethasone), which have anti-inflammatory effects, for advanced KOA. Administered as intra-articular injections directly into the joint, these medications provide direct effect with fewer systemic adverse reactions. Intra-articular injections are recommended over NSAIDs for advanced KOA. Corticosteroids prevent collagen production in the joint, suppress inflammation, relax nerves and other tissues, and indirectly reduce pain. However, corticosteroids relax the nerves and tissues for a prolonged period, which prevents the natural production of healing factors and eventually exacerbates the condition.
Novel therapies. To prevent the degeneration associated with KOA, several innovative therapeutic approaches have been developed, including injecting autologous blood products and mesenchymal stem cells into the affected joint. For example, PRP derived from a patient’s own blood sample can be injected directly into the affected joint to reduce pain and improve mobility. Similar to PRP, stromal vascular fraction, composed of a lesser amount of mesenchymal stem cells and autologous conditioned serum, can be collected from a patient’s whole blood. According to Fotouhi and colleagues, inoculation with these products improves joint mobility by repairing the affected cartilage. The platelet concentrate promotes mitogenesis of healing cells because they contain platelet-derived, vascular endothelial, epithelial, and transforming growth factors. These products also may enhance bone growth by promoting the formation of fibrin, fibronectin, and vitronectin to improve knee function. Researchers continue to explore the clinical efficacy of these products.
Extended release pain management. To prolong the pain relief effect and reduce the adverse effects of high-peak plasma concentration, researchers developed a triamcinolone acetonide (TA) molecule, which has been approved for use in the United States. TA, which is administered as a single 5 mL (32 mg) intra-articular injection, releases slowly into the synovium, enabling prolonged presence in the joint for long-lasting pain relief while also reducing inflammation with fewer adverse effects such as blood glucose elevations. Although the FDA has approved TA’s use, additional evidence will help clarify the magnitude of its benefits.
Surgical management
Surgery remains the definitive treatment for advanced KOA. It should be considered when the patient’s quality of life diminishes significantly. Surgical interventions include cartilage repair, arthroscopy, osteotomy, and partial or total knee replacement. Before choosing a surgical intervention, patients must understand that it won’t stop KOA; instead, it will control disease progression and may improve function for about 20 years. According to Lespasio and colleagues, total knee arthroplasty provides 90% to 95% pain relief with just a 1% to 2% complication rate.
Nursing implications. Many patients may experience preoperative fear and anxiety about mobility limitations, pain, and dependence on others for activities of daily living. Those patients with extreme fear and anxiety are at greater risk for postoperative anxiety and complications. Assess patients’ stress levels before the procedure, and provide appropriate education and emotional support.
Before discharge, emphasize the importance of behavioral changes such as staying physically active and participating in family and community activities. Share information about community recreational opportunities, including swimming, to help maintain physical activity. Community parks and religious organizations that provide indoor and outdoor spaces for recreation also function as occasions for social interaction. Participating in any of these community resources helps reduce social isolation.
Control symptoms, improve quality of life
Risk of KOA, a rising health problem in the United States, increases with age, is higher in women than men, and can be exacerbated by several modifiable risk factors, including obesity. Management should start with exercise to control symptoms before considering pharmacologic and interventional options. As vital members of the interprofessional team, nurses help develop individualized care plans that aim to enhance patients’ quality of life.
Mary Variath was a nursing educator at Case Western Reserve University in Cleveland, Ohio. She’s authored book chapters on osteoarthritis, osteoporosis, and osteomyelitis.
References:
Ackerman IN, Kemp JL, Crossley KM, et al. Hip and knee osteoarthritis affects younger people, too. J Orthop Sports Phys Ther. 2017;47(2):67-79. doi: 10.2519/jospt.2017.7286
Brosseau L, Taki J, Desjardins B, et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part two: Strengthening exercise programs. Clin Rehabil. 2017;31(5):596-611. doi:10.1177/0269215517691084
Bruyère O, Cooper C, Cutolo M, Reginster J-Y. International endorsement of the ESCEO algorithm for management of knee osteoarthritis in clinical practice. Semin Arthritis Rheum. 2017;47(2):e10. doi: 10.1016/j.semarthrit.2017.07.002
Chen L, Zheng JJY, Li G, et al. Pathogenesis and clinical management of obesity-related knee osteoarthritis: Impact of mechanical loading. J Orthop Translat. 2020;24:66-75. doi:10.1016/j.jot.2020.05.001
Damar HT, Özlem B. The patient’s experience in total knee arthroplasty: Past-now-future. MedSurg Nurs. 2017;26(2):132-6.
Fotouhi A, Maleki A, Dolati S, Aghebati-Maleki A, Aghebati-Maleki L. Platelet rich plasma, stromal vascular fraction and autologous conditioned serum in treatment of knee osteoarthritis. Biomed Pharmacother. 2018;104:652-60. doi:10.1016/j.biopha.2018.05.019
Ganji R, Pakniat A, Armat MR, Tabatabaeichehr M, Mortazavi H. The effect of self-management educational program on pain intensity in elderly patients with knee osteoarthritis: A randomized clinical trial. Open Access Maced J Med Sci. 2018;6(6):1062-6. doi:10.3889/oamjms.2018.225
Ghai B, Gupta V, Jain A, Goel N, Chouhan D, Batra YK. [Effectiveness of platelet rich plasma in pain management of osteoarthritis knee: Double blind, randomized comparative study]. Braz J Anesthesiol. 2019;69(5):439-47. doi:10.1016/j.bjane.2019.06.005
Hall M, Castelein B, Wittoek R, Calders P, Van Ginckel A. Diet-induced weight loss alone or combined with exercise in overweight or obese people with knee osteoarthritis: A systematic review and meta-analysis. Sem Arthritis Rheum. 2019;48(5):765-77. doi:10.1016/j.semarthrit.2018.06.005
Herrero-Beaumont G, Roman-Blas JA, Bruyère O, et al. Clinical settings in knee osteoarthritis: Pathophysiology guides treatment. Maturitas. 2017;96:54-7. doi:10.1016/j.maturitas.2016.11.013
Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220-33. doi:10.1002/art.41142
Lespasio MJ, Piuzzi NS, Husni ME, Muschler GF, Guarino AJ, Mont MA. Knee osteoarthritis: A primer. Perm J. 2017;21:16-183. doi:10.7812/TPP/16-183
Melzack R, Katz J. The gate control theory: Reaching for the brain. In: Hadjistavropoulos T, Craig KD, eds. Pain: Psychological Perspectectives. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 2004; 13-34.
Mora JC, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: Pathophysiology and current treatment modalities. J Pain Res. 2018;11:2189-96. doi:10.2147/JPR.S154002
Paik J, Duggan ST, Keam SJ. Triamcinolone acetonide extended-release: A review in osteoarthritis pain of the knee. Drugs. 2019;79(4):455-62. doi:10.1007/s40265-019-01083-3
Stefik D, Vranic V, Ivkovic N, et al. An insight into osteoarthritis susceptibility: Integration of immunological and genetic background. Bosn J Basic Med Sci. 2021;21(2):155-62. doi:10.17305/bjbms.2020.4735
Vina ER, Kwoh CK. Epidemiology of osteoarthritis: Literature update. Curr Opin Rheumatol. 2018;30(2):160-7. doi:10.1097/BOR.0000000000000479
Wang X, Perry TA, Arden N, et al. Occupational risk in knee osteoarthritis: A systematic review and meta‐analysis of observational studies. Arthritis Care Res. 2020;72(9):1213-23. doi:10.1002/acr.24333
Wellsandt E, Golightly Y. Exercise in the management of knee and hip osteoarthritis. Curr Opin Rheumatol. 2018;30(2):151-9. doi:10.1097/BOR.0000000000000478
Xu C, Liu T, Driban JB, McAlindon T, Eaton CB, Lu B. Dietary patterns and risk of developing knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthritis Cartilage. 2021;26(6):834-40. doi:10.1016/j.joca.2021.02.571


















1 Comment. Leave new
Thanks for the info.