
Takeaways
- Nursing assignments frequently are based on ratios and geography rather than work intensity associated with a specific patient assignment.
- Nurse satisfaction and perceptions of assignment fairness are highly correlated with workload.
- A quantifiable work intensity tool was developed and used to create fair, equitable, level-loaded assignments, and increasing nurse satisfaction.
Jennifer*, a nurse on a 45-bed acute care unit in a busy hospital, wants to quit her job again. She starts today like every other day this week—feeling overwhelmed. Jennifer has five patients: Maria is anxiously waiting for a test to determine if she has cancer. The prep for the test has her going to the bathroom every 10 minutes for several hours. Angelica, who’s 22 years old, has sickle cell disease. She is using a patient-controlled analgesia (PCA) pump but remains in significant pain and requires constant respiratory mon itoring and hourly medications as needed. Roberto is a postoperative patient with continuous bladder irrigation who also needs hand irrigation in addition to vital signs every hour times four and then every 4 hours. Henry, a 91-year-old man whose hemoglobin is 6.2 g/dL after a GI bleed, needs 2 units of blood. He’s forgetful, and this is his first hospitalization, so he’s frightened. Hazel is an 81-year-old grandmother with pneumonia who rarely sees Jennifer, who is busy caring for the more acutely ill patients.
*Names are fictitious.
A nurse’s workload has a significant effect on patient out comes, yet too often assignments don’t take into account all the factors contributing to that workload. For example, nursing assignments based on ratios or patients’ geographic location on the unit, without considering the intensity of work required to care for individual patients, can lead to unequal workloads, frustration, and reduced satisfaction. Patients may feel that nurses are rushed or don’t have time for them, and nurses may feel guilty about not spending enough time with their patients.
Our hospital system (Cone Health in Greensboro, North Carolina) successfully used Lean methodology to address the issue of ensuring equitable workload when making staff assignments. An interdisciplinary team made up of content experts, stakeholders, and “fresh eyes” (people not directly involved in the assignment process) assembled to complete a weeklong nursing assignment rapid improvement event (RIE), which included describing the current situation, analyzing gaps, and brainstorming and implementing solutions. Our objective during the RIE was to create a dynamic staffing model that allows for assignment level loading and equitable resource allocation.
Where we started
When we started this project, staffing was based on standard ratios, geography, and patient volume; the complexity of the patient wasn’t always taken into account. Nurses felt overburdened with the intensity of work in their individual assignments and that the workload wasn’t fairly distributed. A staff survey demonstrated that nurses felt inefficient, stressed, and short-staffed. In addition, nursing supervisors had difficulty appropriately allocating resources without an accurate nursing workload evaluation.
Several existing tools measure patient acuity, but effectiveness often varies by specialty and level of care. The Cone Health Work Intensity Tool (CHWIT) uses objective and subjective criteria to assign a score (from 1 [lowest intensity] to 20 [highest intensity]) to each patient, making this tool more widely applicable.
For example, a patient with heart failure who needs medications every 4 hours and frequent assistance to the bathroom would be a level 2. However, a complex patient in the intensive care unit who requires continuous renal replacement therapy and a nursing ratio of 1:1 would be a level 10.
With this example in mind, a nurse caring for five level 2 patients and a nurse caring for one-level 10 patient would have equitable assignments based on work intensity. Geography and continuity of care aren’t calculated in the work intensity level, but they’re taken into consideration when making assignments.
What we discovered
Our initial analysis revealed that staffing assignments weren’t made based on work intensity. Instead, each charge nurse used his or her judgment, geography, and budgeted ratios to allocate nursing resources. Without a measured process, charge nurses had no way to accurately gauge which patients required more resources. And even if a charge nurse felt that a group of patients needed more, he or she couldn’t define the work intensity to make adjustments accordingly.
Nursing supervisors frequently are required to make complex decisions related to staff distribution across multiple work units, but they didn’t have a way to make rational and fair decisions about where scarce resources should be allocated. They relied on budgeted matrices. Patient complexity and total departmental workload weren’t considered.
Failure to question existing practice, unclear expectations, and ineffective resource utilization were a few of the root causes identified in the gap analysis. Other challenging components included census disparity, patient churn, and compression complexity (what nurses experience when they’re expected to assume additional, unplanned responsibilities while also performing their regular duties in a condensed time frame).
Finding a solution
The work intensity for each patient had to be quantified to create fair and equitable assignments and to facilitate staff allocation. A process for measuring work intensity and patient level loading was developed by providers, nurses, and clinical experts and rolled out throughout the hospital. An interdisciplinary team developed standard work for the new process, and then department champions and RIE team members provided education to nurses on each department. Key points (such as who was responsible for assigning numbers to the patients and the process for dividing assignments based on work intensity) were developed for the charge nurse, staff nurse, and leadership to follow daily, and champions (RIE team members and department directors and assistant directors) for each department assisted staff with the new pro cess. Follow-up meetings with the champions, pro cess owner, and RIE team leader were scheduled to address any issues. Process control boards, which displayed the department’s progress, opportunities for improvement, and ongoing direct-care problem solving, were posted on each department for use in daily huddles.
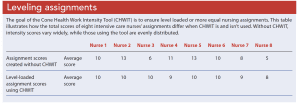
We also developed the Cone Health Work Intensity Tool (CHWIT), which is used to assign a score to each patient based on objective and subjective criteria. (See Measuring intensity.) Individual patient scores are added to calculate a cumulative score for the department, which is then divided by the number of nurses working to come up with the department’s work intensity score. This final score allows nursing supervisors to view the total points for each department and reallocate staff accurately to the higher-scoring departments. CHWIT serves as a guide to standardize work intensity across all departments, so that all nurses and nursing departments speak a common language. The result is equitable assignment distribution (level loading) among the nursing staff. (See Leveling assignments.)
Results
To track tool use and equal workload distribution, the scores were entered into a database and the assignment variance scores were calculated to show how far each nurse’s score was from the average. In other words, if the total work intensity score for the department was 40 and four nurses were working, the average was 10 points per nurse. Target state was +1 to -1 from the average. In this example, an acceptable range would be a score of 9 to 11 per nurse. The assignment variance score was tabulated per department and for the hospital every 2 weeks. The pre-intervention work intensity variance was -2.5 to +2.6 from the average. The variance 60 days after implementing CHWIT was -.83 to +.86. The large pre-intervention variance showed that assignments weren’t level loaded—some nurses’ scores were 2.6 higher (heavier load) than other nurses’, and some were 2.5 lower (lighter load). With time, the variance score decreased, indicating that assignments were more even.
The RIE team administered a pre-intervention nursing satisfaction survey to all inpatient departments and post intervention surveys at 30, 60, and 90 days. At each interval, respondents were asked, “How often do you feel assignments are fairly distributed?” At 90 days, results yielded 97.7% favorable results compared to 63% pre-intervention. Nurses reported that they had more input in each shift assignment and that the assignments were more evenly distributed. Initially, geography issues were posted at the process control boards as barriers, but they declined significantly when the effects of more even assignments were realized.
Making a difference
Today is a new day for Jennifer. Her department now uses CHWIT and nursing assignments are level loaded by work intensity for the oncoming shift. Jennifer still has five patients, but because the entire department is evaluated as a whole with each patient having his or her own work intensity score, assignments are more equitable. Jennifer is still busy with Angelica’s PCA pump, and she will make sure that Henry receives another unit of blood. However, her two new patients are stable with scheduled meds and procedures, giving Jennifer adequate time to spend with Hazel. Jennifer can leave work knowing that she had time to spend with her patients and that she made a difference.
The authors work at Cone Health in Greensboro, North Carolina. Tara Dark is an RN4. Waqiah M. Ellis is executive director of nursing and patient services.
References:
Al-Balushi S, Sohal AS, Singh PJ, Al Hajri A, Al Farsi YM, Al Abri R. Readiness factors for lean implementation in healthcare settings—A literature review. J Health Organ Manag. 2014;28(2):135-53.
Drotz E, Poksinska B. Lean in healthcare from employees’ perspectives. J Health Organ Manag. 2014;28(2):177-95.
Firestone-Howard B, Zedreck Gonzalez JF, Dudjak LA, Ren D, Rader S. The effects of implementing a patient acuity tool on nurse satisfaction in a pulmonary medicine unit. Nurs Adm Q. 2017;41(4):E5-14.
Kidd M, Grove K, Kaiser M, Swoboda B, Taylor A. A new patient-acuity tool promotes equitable nurse-patient assignments. Am Nurse Today. 2014;9(3). myamericannurse.com/a-new-patient-acuity-tool-promotes-equitable-nurse-patient-assignments/


















2 Comments.
only 5 patients? try 8-9 patients, 7 on a good day
Is there any way I can get hold of the author to request for permission to access and utilize this tool?
Thank you.