Identification, prevention, and management
Learning Objectives
- Describe causes and risk factors for moisture-associated skin damage (MASD).
- Describe the pathophysiology related to the four most common types of MASD.
- Define the prevention and management strategies for the four most common types of MASD, including incontinence-associated dermatitis, intertriginous dermatitis, periwound MASD, and peristomal MASD.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 10/1/25
Skin integrity and steroid medications
Obesity: Skin issues and skinfold management
Takeaways:
- The four most common types of MASD are incontinence-associated dermatitis, intertriginous dermatitis or intertrigo, periwound MASD, and peristomal MASD.
- Identifying the cause MASD is critical in addressing the issue.
- A structured skin care protocol that decreases the incidence of IAD includes gentle cleansing, moisturizing, and protection of the skin.
- Comorbidities such as diabetes and obesity contribute to MASD and addressing any contributing health issues will help improve patient outcomes.
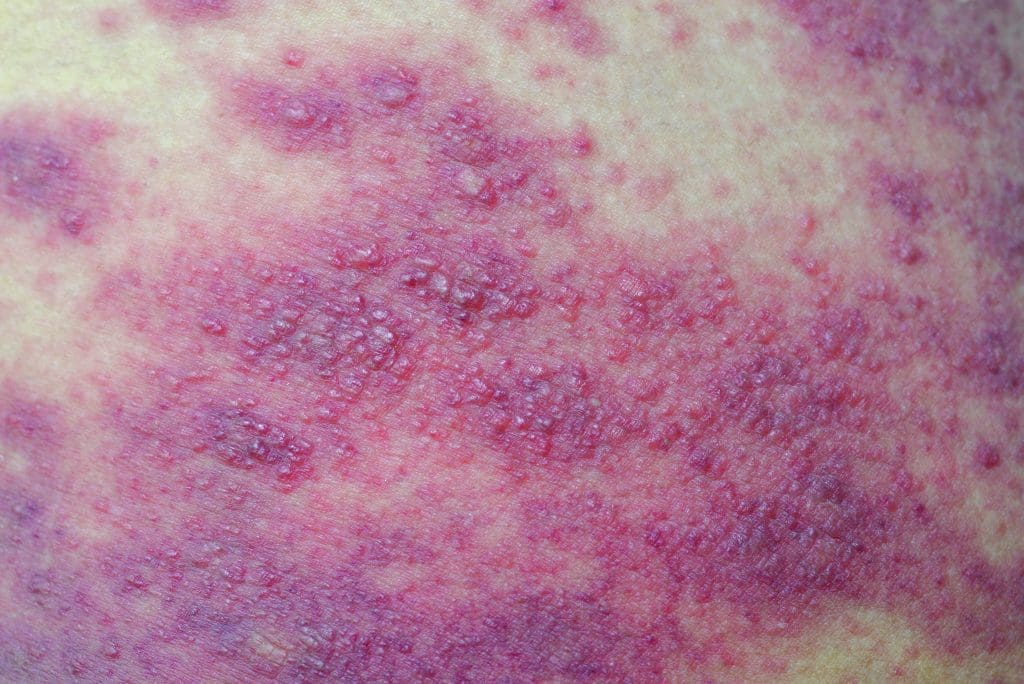
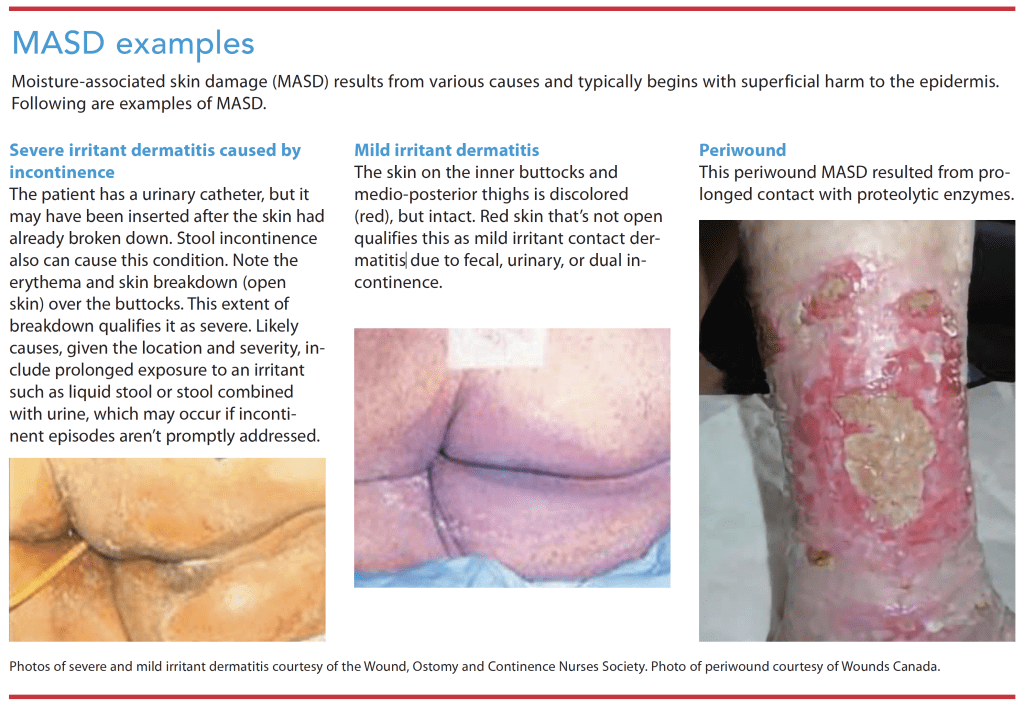
Moisture-associated skin damage (MASD), inflammation and erosion of the skin, results from prolonged exposure to different sources of moisture such as feces, urine, sweat, saliva, wound exudate, mucus, perspiration, digestive secretions, and other bodily fluids. This prolonged exposure leads to irritant contact dermatitis. Common manifestations include local inflammation with erythema (pink or red color or lighter or darker than usual skin tone), inflamed skin with irregular borders, erosion of superficial skin layers, and sometimes rash from fungal or bacterial skin infection. Considered top down skin damage, MASD begins with superficial damage to the epidermis (“bottom up” damage, such as pressure injuries [PIs], begins with deeper tissue as a result of ischemia and then progresses to the superficial tissue and skin). (See MASD examples.)
The four most common types of MASD are incontinence-associated dermatitis (IAD), intertriginous dermatitis (ITD) or intertrigo, periwound MASD, and peristomal (skin around stomas such as fecal and urinary ostomies, tracheostomies, and gastrostomies) MASD. Other forms of MASD not covered in this article include irritant contact dermatitis caused by contact with saliva and irritant contact dermatitis related to unspecified stoma or fistula.
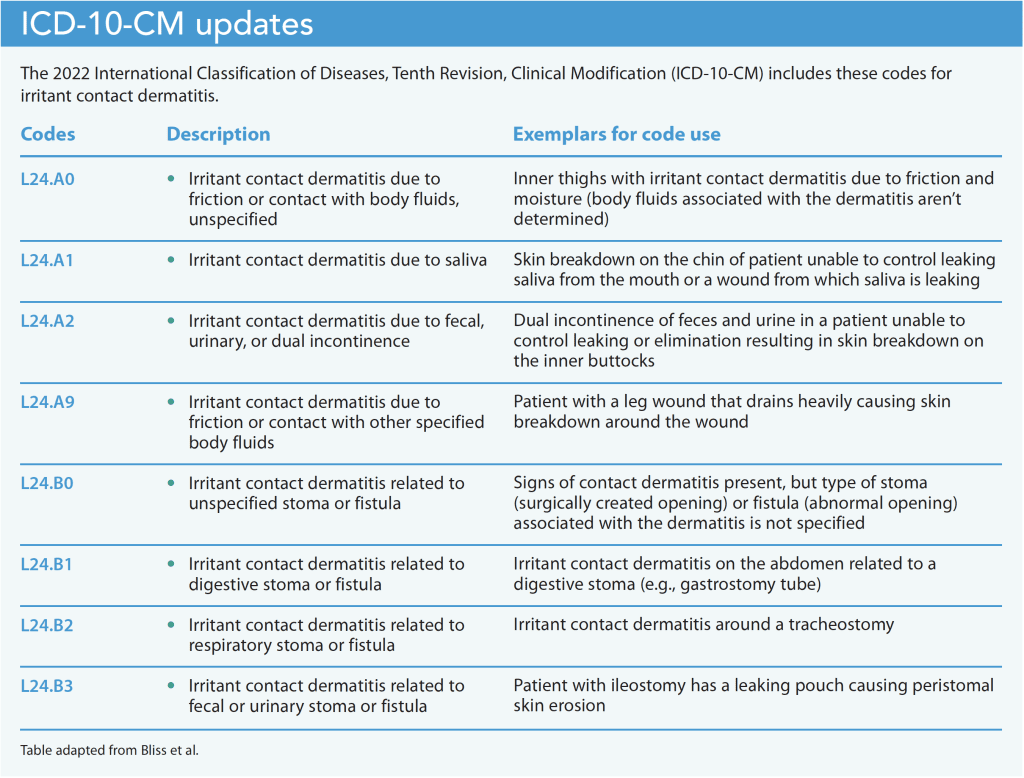
In October 1, 2021, the Wound, Ostomy and Continence Nurses Society (WOCN) spearheaded important updates in the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) related to differentiation and documentation of various MASD. The ICD-10-CM codes, applied worldwide for disease identification, are used in the United States for insurance and healthcare supply reimbursements. The WOCN added several codes under the category of Contact Dermatitis, using different MASD etiologies to make distinctions. To ensure consistent documentation, all clinicians should review and correctly use the new codes. (See ICD-10-CM updates.)
MASD pathophysiology
Overhydration of the stratum corneum, the outermost layer of the skin’s epidermis, compromises the structure of the epidermal layer. This allows penetration of the skin by irritants that cause inflammation and skin erosion, which can result in the entry of microorganisms that lead to infection. Prolonged exposure of the skin to moisture, such as from urine or feces, changes the skin’s pH, which makes it more penetrable to irritants and infectious organisms. Skin exposed to excess moisture also has reduced resistance to mechanical stresses of pressure, shear, and friction.
Some interventions meant to address skin moisture may cause further damage. For example, forcefully rubbing the perineal skin during incontinence clean up can result in friction injury. Alkaline soap used for cleansing can reduce the stratum corneum thickness and alter the skin’s pH, which is naturally acidic (pH between 4 to 6.8). Excess moisture or alkaline soap can destroy this acid mantle and allow irritants and pathogens to enter the skin.
Several factors increase a person’s MASD risk. These include advanced age, obesity, environmental factors, immobility, use of occlusive containment products such as plasticized undergarments, diminished cognition, an inability to perform personal hygiene, fever, medications such as antibiotics and immunosuppressants, poor nutrition, and critical illness.
Incontinence-associated dermatitis
Skin inflammation from prolonged exposure to urine or stool, particularly liquid stool, can result in IAD. Signs include redness, swelling, pain, and in some cases, pruritus. In people with darker skin, IAD may present with subtle redness or discoloration of the surrounding area. Anyone with IAD may have blistering and confluent or patching lesion distribution with irregular edges and erythema. The lesions may be shallow, denuded, and macerated. Most IAD lesions occur in the perineal area, buttocks, inner thighs, groin, and the lower part of the abdominal skin folds. If the lesions are draining, typical exudate is clear, serous, weepy, or sanguineous.
IAD can place an individual at increased risk for PI. In fact, IAD frequently is misidentified as superficial (stage 1 or 2) PI.
Prevention and management
When possible, IAD prevention starts with a bowel and bladder program (timed or prompted toileting). Identifying the cause of the incontinence also is key. For example, a resident in a nursing home who reports being incontinent at night may not be able to reach the bathroom in time because of mobility and visual issues. A bedside commode and a clap-activated bedside lamp may help solve the issue.
Depending on circumstances, other IAD interventions may be appropriate. For example, patients with stage 3 or 4 PIs may benefit from an indwelling urinary catheter. In hospital units, patients with liquid stool may benefit from internal or external fecal management or containment systems. Absorptive wearable incontinence garments can be used; however, these products create an occlusive environment that increases skin temperature and humidity, which contribute to IAD development. Instead, most hospitals use nonwearable absorptive products (disposable pads) and limit wearable incontinence garments to physical therapy or ambulation. In the community setting, caregivers and patients frequently choose wearable incontinence garments to promote dignity. To help avoid IAD, advise patients to select products that wick wetness from the skin, schedule regular cleaning, and promptly change soiled or wet garments.
A landmark systematic literature review by Beeckman and colleagues identified a structured skin care protocol that helps decrease IAD incidence. The three-step process includes gentle cleansing, moisturizing, and protection of the skin. No-rinse cleansers containing surfactants are recommended over standard soap and water for clean-up. Moisturizers that replace the lipid on the skin and products that coat the skin to protect it from overhydration, irritants, and urinary/fecal pathogens also are recommended. Advise patients to avoid products with fragrance and dyes, which may cause irritation.
Intertriginous dermatitis
ITD Lesions are erythematous, moist red or red-brown, and beefy. Linear erosions also occur. Pruritus, pain, and foul odor frequently are reported. ITD can occur anywhere on the body where skin opposes skin and traps moisture. Common locations include the axillae, inguinal areas, abdominal skin folds, inframammary folds, and the intergluteal cleft. Lesions also occur in the umbilicus, neck folds, and web spaces of fingers and toes. Patients with limb contractures may develop ITD in the antecubital and popliteal fossae. Risk factors include immobility, obesity, hyperhidrosis, immune deficiencies, diabetes, and malnutrition.
Prevention and management
To prevent and manage ITD, provide careful and diligent skin care, wick or absorb trapped moisture from skin folds, and separate skin folds to prevent skin damage from friction. Recommended skin care regimens include using pH-balanced skin cleansers, gentle cleansing (without scrubbing), using soft cloths (not washcloths), and patting (not rubbing) the skin dry. Avoid talc, cornstarch, antiperspirants, and placing bed or bath linens in skin folds.
Other interventions to treat ITD include drying the affected area with a hair dryer on the cool setting, using absorptive clothing such as cotton to separate skin folds, applying a skin sealant, and applying preservative- and fragrance-free moisture barrier ointments combined with soft folded sponges to maintain skin fold separation. Commercially available wicking textiles, some impregnated with antimicrobial agents, can help decrease the risk of developing skin infections. Weight loss and diabetes treatment, as applicable, also can help manage ITD.
Common ITD complications include secondary infections such as candidiasis and Staphylococcal infections. To treat candidiasis, lightly dust the affected area with antifungal powder. Avoid excessive use of powder, which can lead to caking and increased skin damage caused by friction. If applicable, the provider may prescribe azole antifungal creams (such as miconazole), which have antifungal, anti-inflammatory, and antibacterial effects. For patients with significant pruritus, a low-potency corticosteroid may help.
Periwound MASD
Periwound MASD occurs when wound exudate, containing proteolytic enzymes, comes into prolonged contact with skin. Compared to acute wounds, chronic wounds have higher levels of these enzymes and are more likely to cause periwound MASD. Chronic wounds also tend to be infected and thus more exudative. Associated irritation and pruritus cause the patient to scratch skin, leading to further damage.
Signs of periwound MASD include erythema, maceration, and skin loss. Macerated skin is soggy and soft, and it may be whiter than usual. Among darker-skinned patients, maceration presents as gray-white and wrinkled skin.
Prevention and management
Prevention and management of periwound MASD include selecting dressings with adequate absorptive capacity, changing dressings before they become saturated, and using moisture barrier products to protect periwound skin. Commonly used products include skin sealants, skin barrier ointments or paste, and solid-wafer skin barriers. Ensure periwound skin is kept clean and dry. For seriously ill patients with wounds that have large surface areas, consider obtaining a low air loss mattress.
Peristomal MASD
Peristomal MASD—inflammation or erosion of the skin around ostomies—results from exposure to fecal or urine drainage. Peristomal skin starts at the beginning of the stoma-skin junction and extends outward in an approximately 4-inch radius. Common clinical signs of peristomal MASD include maceration, erythema, and superficial skin loss. Around fecal and urine ostomies, if the skin barrier is cut too large or isn’t correctly fitted around the ostomy, the peristomal skin can be exposed to stool or urine, leading to skin damage.
Prevention and management
To help prevent peristomal MASD provide ostomy care education that focuses on correct sizing of the barrier opening and skin barrier selection. In addition, assess the patient’s technique in applying and removing their pouch to ensure they’re following the correct procedure.
Depending on the source of the peristomal MASD, management may include modifying the pouching system, educating the patient about proper ostomy care, or increasing the frequency of ostomy appliance changes. Consider consulting with a certified ostomy nurse (COCN®) or certified wound, ostomy and continence nurse (CWOCN®), who may implement a convex skin barrier, ostomy accessories (ring barriers or ostomy belts), the “crusting method” (applying powder and a no-sting skin barrier film to create a dry surface for pouch adhesion), or a cyanoacrylate-based product as a protective layer over the skin.
In cases of high stool output or runny consistency that undermines the skin barrier, diet modifications and medications to thicken stool or slow peristalsis may be prescribed. If the patient has diarrhea as the result of an infection, the infection should be treated with antibiotics as appropriate.
For peristomal MASD resulting from leakage around tubes, for example a leaking feeding gastrostomy tube, consult a physician (in this case an interventional radiologist) to help determine the cause of the leak, confirm proper tube placement, and to stabilize the tube. Other interventions include applying a skin sealant, skin barrier ointment or paste, or a solid-wafer skin barrier to protect the skin around the tube. Also consider using a dressing with appropriate absorptive capacity, increasing the frequency of dressing changes as needed, and gently cleansing and drying the peristomal skin.
Complications
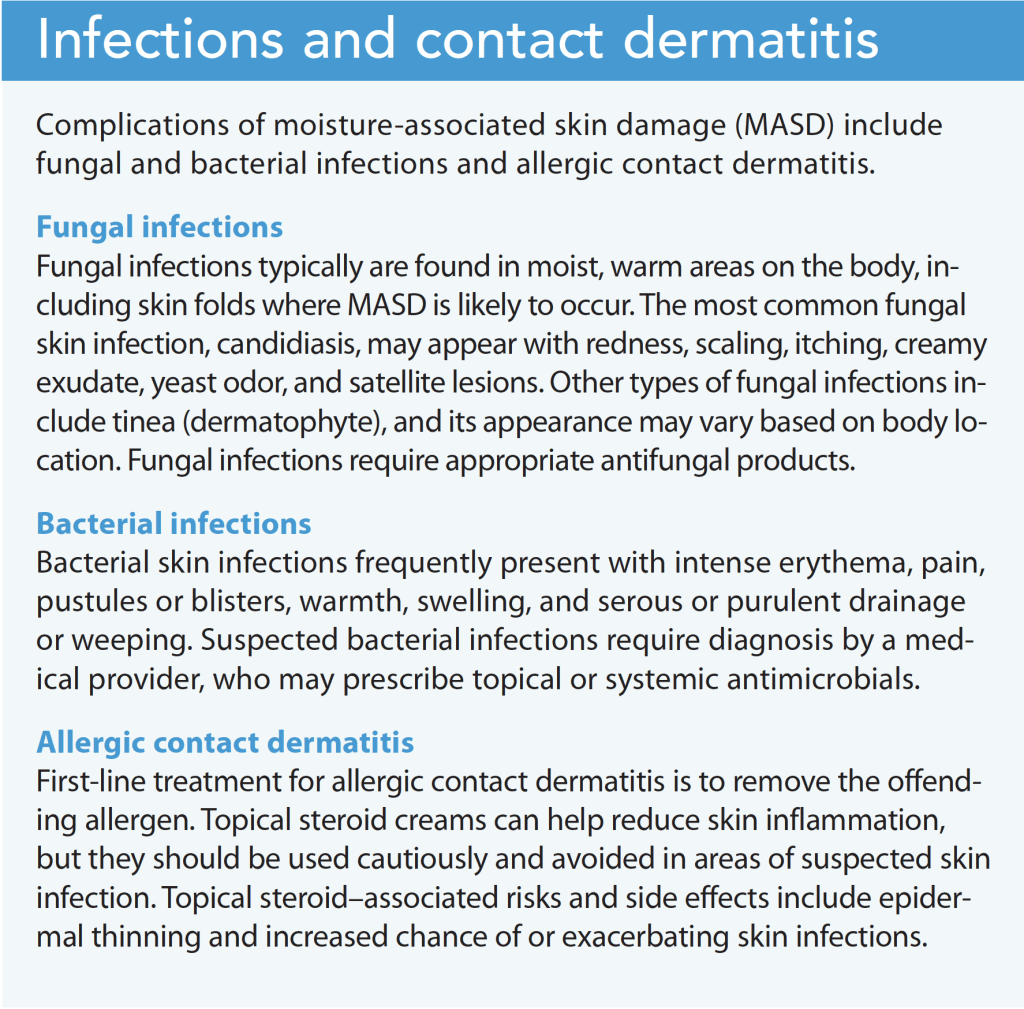
MASD complications include fungal and bacterial skin infections that require identification and treatment by a provider. Viral skin infections aren’t associated with moisture, but some, such as herpes simplex and varicella-zoster viruses, may be found in areas where IAD is common. Some patients may develop localized allergic responses (allergic contact dermatitis). (See Infections and contact dermatitis.)
Improve outcomes
MASD can cause pain and discomfort, secondary infections, and further debilitation. Management requires identifying and treating the cause. Cleansing, moisturizing, and protecting the skin aid in skin repair, help keep the skin intact, and prevent breakdown. Other crucial steps include educating and involving the patient and caregivers in management steps, as well as collaborating with other disciplines, such as physicians, dietitians, and physical therapists. Consulting a wound care specialist, such as a CWOCN, is especially important if MASD worsens or fails to improve after initial interventions. Additionally, for assistance in selecting incontinence garments, consider consulting a wound and incontinence specialist. Addressing contributing health issues, such as diabetes and obesity, also may help improve patient outcomes. AN
At the time of manuscript submission through to acceptance, Armi Earlam worked as a clinical trial recruiter for Indegene. Her background includes working as a lead certified wound, ostomy, and continence nurse. Lisa Woods is a wound, ostomy and continence nurse and nurse educator residing in Littleton, Colorado.
References
Beeckman D, Campbell J, Campbell K, et al. Incontinence-associated dermatitis: Moving prevention forward: Addressing evidence gaps for best practice. Proceedings of the Global IAD Expert Panel. Wounds International. 2015.
Beeckman D, Schoonhoven L, Verhaege S, Heyneman A, Defloor T. Prevention and treatment of incontinence-associated dermatitis: Literature review. J Adv Nurs. 2009;65(6):1141-54. doi: 10.1111/j.1365-2648.2009.04986.x
Bliss DZ, McNichol L, Cartwright D, Gray M. Practice alert: New ICD-10 Codes for MASD. J Wound Ostomy Continence Nurs. 2022;49(1):15-19. doi:10.1097/WON.0000000000000842
Bryant RA. Types of skin damage and differential diagnosis. In: Bryant RA, Nix DP, eds. Acute and Chronic Wounds: Current Management Concepts. St. Louis, MO: Elsevier; 2016; 82-108.
Brodell RT, Dolohanty LB. Intertrigo. UpToDate. 2018. uptodate.com/contents/intertrigo#H1252008555
Earlam A. How to manage peristomal skin problems. Wound Care Advisor. 2016;5(3):8-12.
Gray M, Bliss DZ, McNichol L. Moisture-associated skin damage: Expanding and updating practice based on the newest ICD-10-CM Codes. J Wound Ostomy Continence Nurs. 2022;49(2):143-151. doi:10.1097/WON.0000000000000865
Ketchen R, McCallum C, Onsted HL, Parsons L, Rosenthal S. Caring for easily injured skin: Preventing and managing moisture-associated skin damage. Wounds Canada. February 1, 2021. www.woundscanada.ca/docman/public/1824-home-masd-care-1944e/file
McNichol LL, Ayello EA, Phearman LA, Pezzella PA, Culver EA. Incontinence-associated dermatitis: State of the science and knowledge translation. Advances in Skin and Wound Care. 2018;31(11):502-513. doi:10.1097/01.ASW.0000546234.12260.61
McNichol L, Bliss DZ, Gray M. Moisture-associated skin damage: Expanding practice based on the newest ICD-10-CM Codes for irritant contact dermatitis associated with digestive secretions and fecal or urinary effluent from an abdominal stoma or enterocutaneous fistula. J Wound Ostomy Continence Nurs. 2022;49(3):235-239. doi:10.1097/WON.0000000000000873
Pather P, Hines S, Kynoch K, Coyer F. Effectiveness of topical skin products in the treatment and prevention of incontinence-associated dermatitis: A systematic review. JBI Database System Rev Implement Rev. 2017;15(5):1473-96. doi: 10.11124/JBISRIR-2016-003015
Thayer DM, Rozenboom B, Baronski S. “Top-down” injuries: Prevention and management of moisture-associated skin damage (MASD), medical adhesive-related skin injury (MARSI), and skin tears. In: Doughty DB, McNichol LL, eds. Wound, Ostomy and Continence Nurses Society® Core Curriculum: Wound Management. Philadelphia, PA: Wolter Kluwer; 2016; 281-312.
Wound Source. MASD: What are the types of moisture-associated skin damage? February 1, 2018. woundsource.com/blog/masd-what-are-types-moisture-associated-skin-damage
Wound Source. Preventing maceration in wounds. June 11, 2020. woundsource.com/blog/preventing-maceration-in-wounds#:~:text=Maceration%20occurs%20when%20skin%20has,exposure%20to%20too%20much%20drainage
Wound Source. Complications associated with moisture-associated skin damage. February 1, 2018. woundsource.com/blog/complications-associated-moisture-associated-skin-damage#:~:text=If%20left%20untreated%20or%20not,related%20skin%20injury%20(MARSI)
Key words: moisture-associated skin damage, MASD, incontinence-associated dermatitis, intertriginous dermatitis, intertrigo, periwound MASD, peristomal MASD, wound care

















4 Comments. Leave new
The Moisture-associated skin damage course was very well written.
I appreciated the review of MASD pathophysiology & prevention & management
strategies.
Excellent review of moisture associated skin damage and care.
I feel the article was very complete including all types of moisture associated skin problems. I appreciated the detailed interventions outlined under each section.
Thank you. The table included lists the updated terms used. Exemplars we’re also cited. Appreciate your comment.