
The power of dignity-conserving care to promote nurse and patient well-being
- When providing end-of-life care, nurses face ethical dilemmas related to the dying process and the relief of suffering, which can lead to moral distress.
- Moral distress can have a significant negative impact on nurses, potentially hindering a their ability to provide care and leading some to leave their role or the profession entirely.
- Dignity-conserving care provides existential support and preserves dignity to patients in the setting of palliative or end-of-life care. It also offers the potential to strengthen the nurse–patient relationship and reduce the nurse’s moral distress.
The nursing profession requires intelligence and compassion. This combination, along with a commitment to their patients, pushes nurses to offer comfort and supportive care during every stage of illness and in the face of distressing challenges. According to Amos and Epstein, when providing end-of-life care, nurses face ethical dilemmas related to the dying process and the relief of suffering, which can lead to moral distress. Morley and colleagues define moral distress as the disequilibrium and negative emotions we feel when we know the action we wish to take but are constrained from doing so.
While providing end-of-life care for Sara*, a nursing team struggled to reconcile their role of providing comfort when faced with a complex disease presentation within the restrictions of the hospital environment. According to Grech, acknowledging such self-reflection helps the nurse gain insight and improve practice. Sara’s story furthers the discussion around ensuring a higher quality of life for individuals with a life-limiting illness and simultaneously supporting nurses who experience moral distress while providing end-of-life care.
Sara’s story
Sara was admitted to the hospital with complications related to Huntington’s disease. This rare neurodegenerative disease leads to progressive motor, cognitive, and behavioral impairment and has no disease-modifying treatments. As described by Booij and colleagues, during end-of-life care, individuals with Huntington’s disease experience severe spiritual, emotional, and psychological distress and describe a concern over a loss of their dignity. According to Samperi and associates, Huntington’s disease presents unique care challenges that require nursing staff to identify behavioral triggers, create safe and low-stimulus environments, and provide a structured routine.
Nursing reflection
Huntington’s disease comes with finality, and healthcare providers must fight to endure its endless toll on the human spirit. During her hospitalization, Sara experienced outbursts of extreme anger, spouting obscenities and swinging her arms at those trying to help her. Nursing staff frequently left the room shaken after caring for Sara. Self-awareness and tearful remorse immediately followed these eruptions. She gushed apologies, embarrassed by her behavior. Sara would repeat, “I love you guys. Thank you for everything. Thank you for putting up with me. I’m sorry.” As the disease advanced, Sara’s emotional control diminished. Her compulsive behavior, irritability, and lack of restraint weren’t malicious, but rather a consequence of the disease’s effects on the brain.
Sara moaned and called out for help at all hours of the day and night. The hospital staff attempted to soothe Sara’s anxieties by providing 24-hour in-room companionship. Her escalating behavior alarmed new staff; experienced staff provided education about the disease and Sara’s level of care. However, separating this “angry” and “irrational” patient from Sara, the human living with advanced Huntington’s disease, presented challenges. Many members of the nursing staff lacked the exposure and education to accurately understand the origins of her outbursts.
Over the course of Sara’s hospital stay, her symptoms rapidly progressed. She lost her ability to walk, get in and out of bed, and swallow food. As the disease advanced, her family realized at-home care wasn’t possible. As the goal of returning home with her family slowly slipped away, Sara became increasingly distraught. She verbalized suicidal ideation. “I’m going to throw myself on the floor so I can go home,” she would shout, lunging forward and throwing her body to the ground. Another time, Sara yelled, “I’m going to choke myself,” as she shoveled food into her mouth. In one instance, Sara announced, “I’m going to starve myself,” but later, forgetting her declaration, requested a cup of ice cream.
In these moments, the nursing staff saw Sara’s desperate acts to end her suffering. They witnessed a woman mourning her loss of autonomy, loss of family connections, and loss of hope. The nurses understood that their role was shifting and no longer focused on offering hope of returning home. However, they struggled to define a new focus for their nursing care.
During Sara’s prolonged hospitalization, her family wasn’t able to visit. The nursing staff attempted to connect Sara with her loved ones via phone calls and video conferencing, but these interactions frequently ended in outbursts. Sara cried, lashed out, and threw items across the room. Family contact became a painful reminder of the life that Sara had lost.
Sara was hospitalized for over 6 months before being discharged to a community setting where, only a few weeks later, she died. The nursing staff discovered Sara’s obituary printed in the local newspaper. Her suffering was over, which is what she wanted—what she had been trying to communicate to her caregivers. However, the staff couldn’t help but feel grief that her last few months were spent away from family. The obituary highlighted her accomplishments, her career, and her children. The published photo was almost unrecognizable by the nurses who cared for her. Reading about Sara’s life, the nurses lamented what Huntington’s disease had stolen from her. The incredible woman in the obituary seemed so distant from the Sara they met in the hospital.
Dignity-conserving care
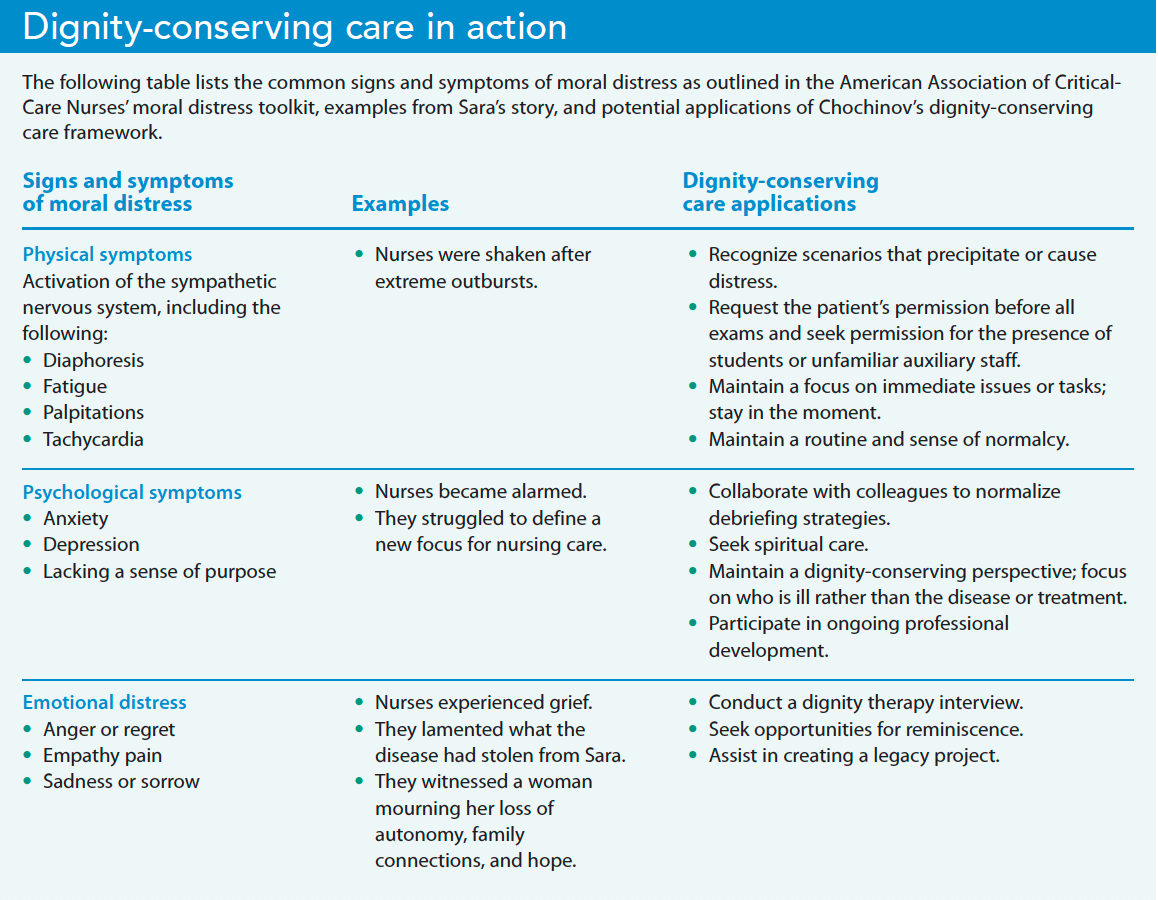
Nurses’ feelings of guilt, sadness, anxiety, and powerlessness are completely reasonable in the face of an ethically complicated clinical situation. According to the American Association of Critical-Care Nurses (AACN), moral distress can have a significant negative impact on healthcare providers, potentially hindering a nurse’s ability to provide care and leading some to leave their role or the profession entirely. The AACN has created a toolkit to help nurses recognize signs of moral distress, differentiate those feelings from those related to burnout or compassion fatigue, and identify the factors that lead to distress. Consider an additional approach to mitigate moral distress experienced by nurses—dignity-conserving care.
Dignity-conserving care not only serves to provide existential support and preserve dignity to patients in the setting of palliative or end-of-life care, it also offers the potential to strengthen the nurse–patient relationship and reduce the nurse’s moral distress. Chochinov created a framework to guide palliative care that seeks to protect the patient’s worth, identity, and honor. The dignity-conserving care model asks providers to view the patient apart from their disease, affirms the individual’s personhood, and supports the patient’s quality of life. For example, nurses, social workers, end-of-life doulas, and palliative care practitioners have used dignity therapy and legacy work—two dignity-conserving interventions—together and separately to mitigate moral distress. (See Dignity-conserving care in action.)
Dignity therapy
Dignity therapy begins with an interview in which the trained nurse (or other facilitator) asks open-ended questions for patient consideration and reflection. Questions such as, “Are there particular roles or accomplishments that you feel most proud of?” offer an opportunity for the individual to see themselves apart from their illness and may bring additional meaning to their end-of-life experience. In addition, research by Saracino and colleagues and Martinez and colleagues points to statistically significant decreases in anxiety and depression among patients who initially reported high levels of psychological or existential distress before participating in dignity therapy.
The nurse and patient can choose to record or transcribe their discussions and incorporate them into a legacy document to share with family and loved ones. Chochinov, who offers guidance on how to introduce dignity therapy and set the stage for an interview, stresses that this intervention is just as much about the process of the interview as it is the answers. Dignity therapy can offer healthcare providers an opportunity to assess the individual’s legacy needs.
Researchers, including Hadler and colleagues, cite mounting evidence that engaging with patient stories significantly impacts patients and providers by generating understanding, improving relationships, and accentuating personhood. When studying the effects of dignity therapy, Nunziante and colleagues found that nurses express a boost in personal and professional growth.
Although dignity therapy offers positive experiences for both nurses and patients, it entails a time commitment that requires leadership support. Even if a nurse can’t access the resources to undergo dignity therapy training, they can adopt Chochinov’s dignity-conserving person-first approach, which focuses on who is ill, rather than only what ails them.
Legacy work
Collins describes the goal of legacy work, a less-formal approach to the dignity-conserving psychotherapy practice of dignity therapy, as creating a document or work of art that serves as a record of the individual’s life experiences. These projects might incorporate a formal dignity therapy interview transcript, but facilitators also can support the individual in creating a scrapbook, playlist of favorite songs, video diary, or letters to loved ones. Cahalan and colleagues describe digital storytelling or narrative legacy projects as facilitating emotional expression for individuals who are more comfortable with technology or perhaps seek a level of distance.
According to Collins, nurses who participate in legacy work express a sense of personal fulfillment and job satisfaction. Whether it’s a transcript of the dignity therapy discussion or a painting produced by the patient, Cahalan and colleagues describe these items as providing family members with a tangible memory during their bereavement and enhancing feelings of purpose and meaning among patients with terminal illnesses.
Legacy work and dignity therapy engage the nurse in dignity-conserving care that brings additional meaning to themselves and the patient. When symptom management proves difficult, these practices may help the nurse re-focus to better support the patient’s sense of identity and hold space for that individual’s lived experience.
Evolving end-of-life care
The increased feelings of fulfillment and personal growth experienced by nurses who participate in dignity therapy or legacy work may help ease feelings of powerlessness and frustration associated with moral distress. Although Sara didn’t have a chance to complete a legacy project, her impact on the nursing unit endures as nurses reflect on their efforts to meet her care needs. They experienced intense grief when they learned about a side of Sara they never had the chance to know. They recognize Sara’s individuality and personhood, which motivates them to seek connection with future patients and their caregivers. The nurses providing Sara’s care lacked the knowledge of Chochinov’s model of dignity-conserving care, and they may have been unaware that, according to Sokol and colleagues, increased feelings of meaning and purpose are associated with higher levels of well-being among individuals with Huntington’s disease.
We must evolve our end-of-life nursing care to incorporate palliative approaches that honor the patient’s identity separate from their illness, strengthen the connection between patient and caregiver, protect dignity at end-of-life, and potentially increase support to nurses facing moral distress.
The authors are clinical assistant professors at the University of Vermont in Burlington. Emily Glassman’s certification as an end-of-life doula informs her RN practice. Abilene Smith specializes in neurology, neurosurgical services, and rehabilitation.
*The patient’s profile has been changed to maintain confidentiality.
American Nurse Journal. 2023; 18(10). Doi: 10.51256/ANJ102318
References
American Association of Critical-Care Nurses. Recognize & address moral distress. July 2020. aacn.org/~/media/aacn-website/clincial-resources/moral-distress/recognizing-addressing-moral-distress-quick-reference-guide.pdf
Amos VK, Epstein E. Moral distress interventions: An integrative literature review. Nurs Ethics. 2022;29(3):582-607. doi:10.1177/09697330211035489
Booij SJ, Tibben A, Engberts DP, Marinus J, Roos RAC. Thinking about the end of life: A common issue for patients with Huntington’s disease. J Neurol. 2014;261(11):2184-91. doi:10.1007/s00415-014-7479-4
Cahalan L, Smith A, Sandoval M, Parks G, Gresham Z. Collaborative legacy building to alleviate emotional pain and suffering in pediatric cancer patients: A case review. Children. 2022;9(1):33. doi:10.3390/children9010033
Chochinov HM. Dignity and the essence of medicine: The A, B, C, and D of dignity conserving care. BMJ. 2007;335(7612):184-7. doi:10.1136/bmj.39244.650926.47
Chochinov HM. Dignity-conserving care—A new model for palliative care: Helping the patient feel valued. JAMA. 2002;287(17):2253-60. doi:10.1001/jama.287.17.2253
Chochinov HM. Dignity Therapy: Final Words for Final Days. Oxford, England: Oxford University Press; 2012.
Collins A. “It’s very humbling”: The effect experienced by those who facilitate a legacy project session within palliative care. Am J Hosp Palliat Med. 2019;36(1):65-71. doi:10.1177/1049909118787772
Grech J. Critical self-reflection for nurse educators: Now more than ever! Teach Learn Nurs. 2021;16(1):89-91. doi:10.1016/j.teln.2020.09.001
Hadler RA, Goldshore M, Rosa WE, Nelson J. “What do I need to know about you?”: The patient dignity question, age, and proximity to death among patients with cancer. Support Care Cancer. 2022;30(6):5175-86. doi:10.1007/s00520-022-06938-2
Martinez M, Arantzamendi M, Belar A, et al. ‘Dignity therapy,’ a promising intervention in palliative care: A comprehensive systematic literature review. Palliat Med. 2017;31(6):492-509. doi10.1177/0269216316665562
Morley G, Ives J, Bradbury-Jones C, Irvine F. What is ‘moral distress’? A narrative synthesis of the literature. Nurs Ethics. 2019;26(3):646-62. doi:10.1177/0969733017724354
Nunziante F, Tanzi S, Alquati S, et al. Providing dignity therapy to patients with advanced cancer: A feasibility study within the setting of a hospital palliative care unit. BMC Palliat Care. 2021;20(1):129. doi:10.1186/s12904-021-00821-3
Samperi SV, Kwong P, McGill T, Tsui DS. Huntington’s disease: A nursing perspective. Australasian J Neurosci. 2021;31(2):18-26. doi:10.21307/ajon-2021-007
Saracino RM, Rosenfeld B, Breitbart W, Chochinov HM. Psychotherapy at the end of life. Am J Bioeth. 2019;19(12):19-28. doi:10.1080/15265161.2019.1674552
Sokol LL, Troost JP, Kluger BM, et al. Meaning and purpose in Huntington’s disease: A longitudinal study of its impact on quality of life. Ann Clin Transl Neurol. 2021;8(8):1668-79. doi:10.1002/acn3.51424
Key words: moral distress, end-of-life care, dignity-conserving care


















