
Evidence-based strategies for nurse preceptors
The complex role of nurse preceptor requires a combination of clinical expertise and the ability to balance patient care with learning facilitation. The nursing shortage, high staff turnover rates, and increased patient acuity have amplified the need for the profession to efficiently and effectively prepare new nurses to function as competent members of the healthcare team. However, during the transition from school, new nurses frequently experience an academic–practice gap in which they have difficulty transferring knowledge and theory to the clinical setting.
According to Murray and colleagues, new graduate nurses tend to focus on tasks rather than reasoning skills, which can impair patient safety and holistic care. In addition, many current new nurses have been affected by the early protocols of the COVID-19 pandemic, which included replacing hands-on clinical experience with virtual learning.
A study by Hickerson and colleagues found that graduate nurses recognize their inability to apply knowledge holistically, which causes them psychological stress and increases staff turnover. Successful precepting can help bridge the academic–practice gap, which improves intent to stay in the profession and promotes patient safety. To enhance this positive impact, nurse preceptors must have a firm understanding of learning theory and effective teaching strategies to facilitate clinical reasoning and judgment.
New nurses and clinical judgment
In the Novice to Expert Model, Patricia Benner describes five levels of skill acquisition and proficiency: novice, advanced beginner, competent, proficient, and expert. The nurse starts as a novice and moves through the levels as they develop more experience and skills. New graduate nurses are considered advanced beginners. They have some real-life patient care experience, but they rely on rules and guidelines. Advanced beginners need help with prioritization and pattern recognition in clinical practice.
Connor and colleagues define clinical judgment as a “reflective and reasoning process that draws upon all available data, is informed by an extensive knowledge base, and results in the formation of a clinical conclusion.” The ability of the nurse to clinically reason and form judgments is associated with patient safety. Nurses at Benner’s advanced beginner stage lack the experience and therefore the ability to form clinical judgments.
Recognizing the importance of clinical reasoning on patient outcomes, the National Council of State Boards of Nursing developed the Next Generation NCLEX, which emphasizes clinical reasoning and decision-making to form clinical judgments. The American Association of Colleges of Nursing also calls for threading the concept of clinical reasoning throughout academic nursing programs. Although academic nursing programs are implementing teaching and learning strategies to focus on clinical reasoning skill development, the new nurse still needs guidance to translate knowledge and theory into practice. That’s where the nurse preceptor comes in. As a nurse preceptor, you can provide that guidance with teachable moments during clinical practice. (See Teachable moments.)
Teachable moments
Nurse preceptors face the challenge of teaching while simultaneously overcoming obstacles such as time constraints and complex patient needs. As a result, teaching and learning in clinical practice tend to occur unprompted during a teachable moment—spontaneous events or situations that provide an opportunity for learning in real time.
Teachable moments can happen at any stage of the nursing process. For example, the preceptor can ensure teaching and learning occur during medication administration by asking the new graduate about the medication’s indications, actions, and adverse effect. Both the preceptor and the learner should take advantage of teachable moments to maximize the learning experience.
Evidence-based teaching strategies
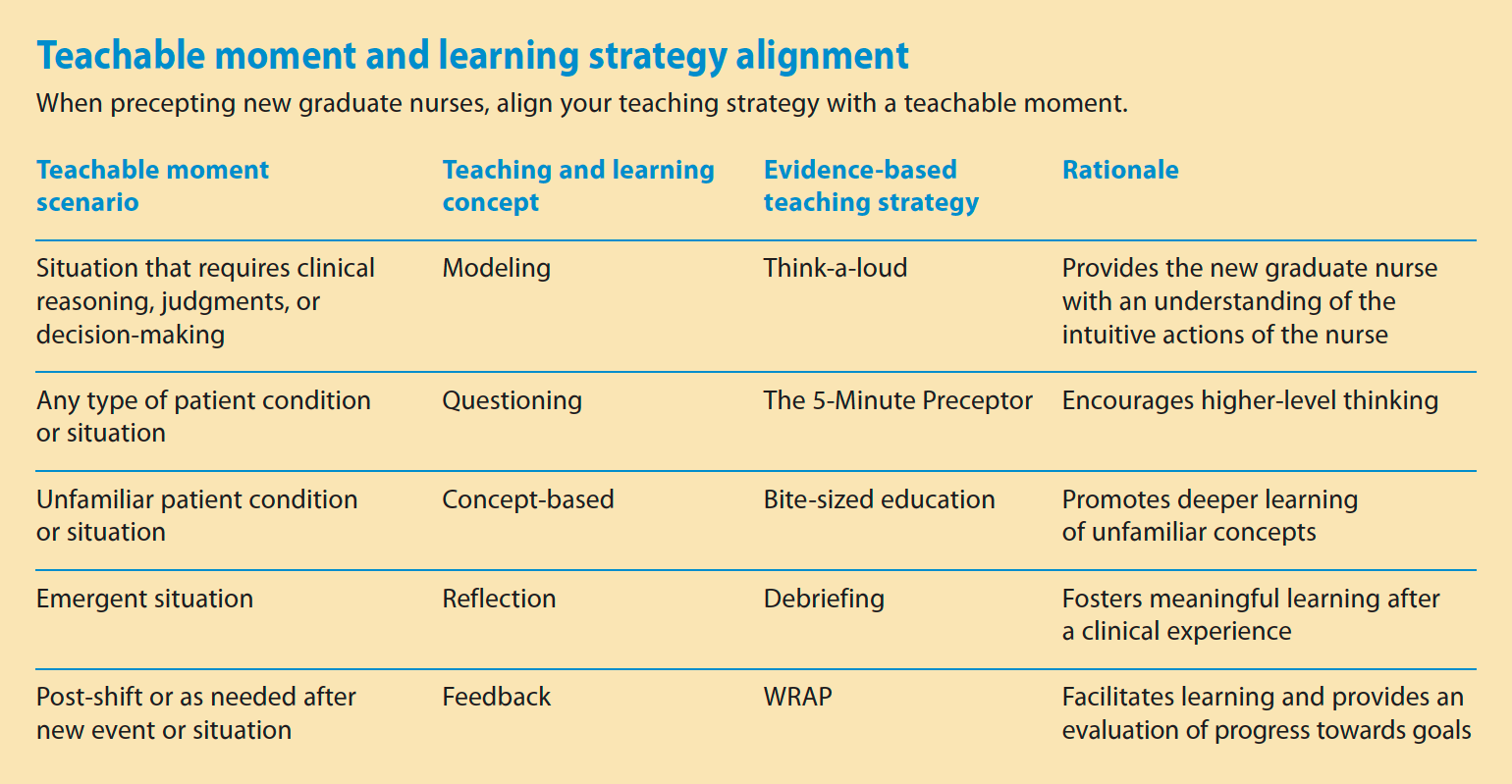
Nurse preceptors provide guidance to graduate nurses and help them apply safe patient care that meets and or exceeds entry-level skills competencies. This includes facilitating clinical reasoning and judgment using an evidence-based approach. The following teaching strategies help facilitate clinical judgment for easy application in clinical practice settings during teachable moments. (See Teachable moment and learning strategy alignment.)
Modeling
Model attributes of a professional nurse to help graduate nurses transition to practice and socialize within the profession. Gcawu and Van Rooyen found that modeling emotional intelligence, self-evaluation, and continuous professional development influences the professional role development of new nurses. Modeling includes not only professional concepts, but also physically demonstrates how to perform skills and critically reason through patient problems and scenarios.
One way to model reasoning in clinical practice is by thinking out loud. You may act intuitively, but new nurses may not understand the thought process behind your actions. When you think out loud, you make what you do explicit to learners. For example, you might intuitively check the oxygen saturation on a patient who’s tachypneic. When thinking out loud, you might say, “I noticed the patient has an increased respiratory rate, which is a sign of respiratory distress. Let’s get the pulse oximeter and check their oxygen saturation.”
Questioning
Many preceptors use lower-order and higher-order (open-ended) questions during teachable moments. Use lower-order questions to determine knowledge comprehension. Typically, these questions can be answered using basic recall of facts or with a “yes” or “no” response (“What is a normal respiratory rate?”). Use higher-order questions to prompt a thoughtful response and clinical reasoning and judgment (“Why do you think this patient is tachypneic?”).
Bott and colleagues adapted a structured approach to questioning. The Five-Minute Preceptor (5MP) is a nursing-focused variation of the One-Minute Preceptor, which was originally created for medical students. The 5MP clinical teaching tool consists of five steps (take a stand, probe for supporting evidence, teach general rules, reinforce what was done right, correct errors) that can be applied to any patient condition or situation.
In the first step—take a stand—ask questions to determine the new nurse’s overall understanding of the patient’s situation or condition. For example, when caring for a patient who requires a blood transfusion, ask, “Why do you think this patient requires a blood transfusion?” Next, probe for supporting evidence to identify any gaps in knowledge or misunderstandings. Examples of probing questions include, “What lab values indicate that a blood transfusion is necessary?” or “What are signs of a transfusion reaction?” The next step—teach general rules—includes addressing misunderstandings, presenting policies and procedures, and explaining guidelines. In the case of a patient receiving a blood transfusion, review care priorities, institutional blood transfusion policies, and I.V. tubing set up. The last two steps involve constructive feedback to reinforce what was done right and guidance to correct errors.
Concept-based teaching
Concept-based teaching focuses on theoretical knowledge rather than hands-on learning. With this approach, new graduate nurses focus on a single topic to gain a deeper understanding. Once an in-depth understanding occurs, they can apply the concept to different patient populations or situations. According to Nielsen and colleagues, concept-based learning increases deep learning and facilitates clinical judgment among nursing students.
Bartram and colleagues found that the bite-sized education approach—one example of concept-based teaching—significantly increased nurses’ knowledge of physical health conditions. Although primarily used in mental health settings, this approach can be applied to any area of nursing. It’s suited for new graduate nurses because it teaches simple concepts with the potential for deep learning.
An ideal situation to implement the bite-sized approach is when the new nurse is caring for a patient with a diagnosis they’re not familiar with. Instruct the new nurse to prepare a brief presentation on the condition, including signs, symptoms, causes, and basic management. Then plan with the new nurse a time for the presentation followed by discussion. If possible, schedule the activity with other new nurses and orientees.
Reflection
Reflection prompts the learner to make meaning from clinical experiences by questioning thinking strategies and examining actions. Taking time to reflect is an essential aspect of teaching and learning; however, the fast-paced clinical environment or an emergent situation may not allow time to pause for reflection. For example, during a code, you can’t pause to explain procedures or review policies.
When this occurs, use debriefing to aid learning. Debriefing (immediately after the event or at the end of shift) provides time for thoughtful reexamination of an experience. Encourage the learner to reflect on the experience while you provide feedback and guide thinking. Dreifuerst’s Debriefing for Meaningful Learning model suggests asking the new nurse to explain the scenario and the first thing that comes to mind about the experience. Ask the nurse to explain what went right and what requires improvement. Also ask them to discuss patient goals, nursing interventions, and care. These talking points facilitate analysis of the situation and provide you with an understanding of the new nurse’s thinking. You can then provide education to clarify any misunderstandings about the experience.
Feedback
Integrate regular, timely feedback into the precepting process. It should be constructive and unbiased. Some teaching strategies, such as 5MP and debriefing, have feedback built into their structure, but others may not. In this case, you can provide meaningful feedback by using a feedback model as a guide.
Besse and Vogelsang proposed the WRAP (Wonder, Reinforce, Adjust, Plan) method to provide constructive feedback that facilitates reflection and a collaborative plan for improvement. During the first step, wonder, encourage the new nurse to reflect on their performance and identify areas of strength and improvement. You might ask questions such as “What do you think went well today and what do you want to improve going forward?” Then affirm the strengths in the reinforcement step. During the adjustment step, discuss the nurse’s identified weaknesses in more detail and together determine reasons why the mistakes occurred. Also note any other opportunities for improvement. The feedback process ends with a plan for what to do next time.
An influential role
Nurse preceptors play an influential role in new nurses’ successful transition to practice. The academic–practice gap frequently leaves new graduates lacking in clinical reasoning skills. Nurse preceptors help to bridge that gap by providing guidance, feedback, and opportunities for socialization. Preceptors, too, can benefit from initial and periodic education to develop precepting skills and to stay current with best practices for educating new graduate nurses.
Taylor Grube is an assistant professor of nursing and director of the RN-to-BSN program at Moravian University in Bethlehem, Pennsylvania.
American Nurse Journal. 2023; 18(6). Doi: 10.51256/ANJ0623115
References
American Association of Colleges of Nursing. The Essentials of Baccalaureate Education for Professional Nursing Practice. Washington, D.C.: American Association of Colleges of Nursing; 2021.
Attenborough J, Abbott S, Brook J, Knight RA. Everywhere and nowhere: Work-based learning in healthcare education. Nurse Educ Pract. 2019;36:132-8. doi:10.1016/
j.nepr.2019.03.004
Bartram R, Dias R, Thompson S, et al. Bitesized teaching: Delivering knowledge of physical health issues in mental health settings. Br J Mental Health Nurs. 2017;6(6):265-71. doi:10.12968/bjmh.2017.6.6.265
Benner P. From novice to expert. Am J Nurs. 1982;82(3):402-7. doi:10.2307/3462928
Besse C, Vogelsang L. The WRAP: An alternative to sandwich feedback in clinical nursing education. J Nurs Educ. 2018;57(9):570. doi:10.3928/01484834-20180815-12
Bott G, Mohide EA, Lawlor Y. A clinical teaching technique for nurse preceptors: The five minute preceptor. J Prof Nurs. 2011;27(1):35-42. doi:10.1016/j.profnurs.2010.09.009
Connor J, Flenady T, Massey D, Dwyer T. Clinical judgment in nursing—An evolutionary concept analysis. J Clin Nurs. 2022. doi:10.1111/jocn.16469
Dreifuerst KT. The essentials of debriefing in simulation learning: A concept analysis. Nurs Educ Perspect. 2009;30(2):109-14
Dreifuerst KT. Getting started with debriefing for meaningful learning. Clin Simul Nurs. 2015;11(5):268-75. doi:10.1016/j.ecns.2015.01.005
Gcawu SN, van Rooyen D. Clinical teaching practices of nurse educators: An integrative literature review. Health SA. 2022;27:1728. doi:10.4102/hsag.v27i0.1728
Gonzalez L, Nielsen A, Lasater K. Developing students’ clinical reasoning skills: A faculty guide. J Nurs Educ. 2021;60(9):485-93. doi:10.3928/01484834-20210708-01
Hickerson KA, Taylor LA, Terhaar MF. The preparation–practice gap: An integrative literature review. J Contin Educ Nurs. 2016;47(1):17-23. doi:10.3928/00220124-20151230-07
Huston CL, Phillips B, Jeffries P, et al. The academic-practice gap: Strategies for an enduring problem. Nurs Forum. 2018;53(1):27-34. doi:10.1111/nuf.12216
Murray M, Sundin D, Cope V. New graduate nurses’ understanding and attitudes about patient safety upon transition to practice. J Clin Nurs. 2019;28(13-14):2543-52. doi:10.1111/jocn.14839
National Council of State Boards of Nursing. Next generation NCLEX: An enhanced NCLEX. 2023. ncsbn.org/exams/next-generation-nclex.page
National League for Nursing. Debriefing Across the Curriculum: A Living Document from the National League for Nursing. June 2015. nln.org/docs/default-source/uploadedfiles/professional-development-programs/nln-vision-debriefing-across-the-curriculum.pdf
Nielsen A. Concept-based learning in clinical experiences: Bringing theory to clinical education for deep learning. J Nurs Educ. 2016;55(7):365-71. doi:10.3928/01484834-20160615-02
Pinto Zipp G, Kolber C. Identifying teachable moments in the clinical setting and possible barriers. J Allied Health. 2014;43(1):32-7.
Reynolds LM, Attenborough J, Halse J. Nurses as educators: Creating teachable moments in practice. Nursing Times. 2020;116(2):25-8.















