Learn how to bring the patient-simulator experience to nursing units to prepare for emergencies.
Takeaways:
- Bring the patient simulator experience to your unit to practice mock codes.
- Ensure your nursing staff knows how to call a code.
- Confirm nurses are comfortable with their crash carts on the unit.
By Deb Sitter, MA, BSN, BSM, RN-BC, NEA-BC
Because of low acuity and patient census, the critical access hospitals (CAH) where I work don’t experience many code blue and rapid response events. As a CAH nurse educator, I started looking for ways to practice emergency responses in reality-based scenarios. Eventually, I collaborated with a small team of interdisciplinary professionals to bring a simulator experience to the hospitals using a portable, medium-fidelity manikin (patient-simulator). If you’re interested in creating a similar project at your organization, my experience may help.
Get leadership support
Before the project started, I approached nursing leadership to gain support for performing surprise mock code exercises at two rural CAHs, using nursing time and supplies. My main objective was to learn more about our code response and improve response times. I provided logistical information to nurse leaders along with answers to their when, where, who, how, and what questions. I felt that the answer to the why question was the most important: Nurses appreciate the opportunity to practice in a safe and supportive environment. And nursing experts agree that simulations are essential to fully engage learners and achieve successful training.
Financial considerations

The mock code exercises used less than 1 hour per mock code per hospital. This time included planning, setup, and execution of the drills. Support staff time was less than 1 hour for each drill. Leadership supported the surprise mock code exercises based on the importance of the learning exercise and the responsible use of personnel time.
Form the team
With leadership’s full support, the code training team began to take shape. The emergency medical services (EMS) instructor manager assisted with the use of a medium-fidelity manikin. The team, which varied according to availability, included hospital EMS staff, the CAH quality coordinator, and unit secretaries. They observed drills, timed them, and provided valuable insight.
Set the objectives
The objective of the project was to provide practice in emergency and nonemergency situations. The team agreed that we also wanted to provide time to debrief after each mock emergency.
Call a code
With no department boundaries, the team took the patient-simulator to all areas of the hospital, providing realistic educational opportunities while staff practiced emergency response scenarios. Code blue buttons were pushed, pages sent over nurses’ phones, overhead announcements made, cardiopulmonary resuscitation (CPR) performed, automatic compression devices brought to the patient-simulator and put in position, crash carts opened, I.V. lines started, “medications” administered, defibrillator monitors charged, and patient-simultors defibrillated and intubated. All the while, healthcare staff hearts raced with adrenaline; many participants said they were surprised that the mock codes created the same nervousness they might experience in an actual emergency, which helped it feel real.
At the end of each scenario, the staff explored equipment and supplies and participated in a short debriefing session to review what went well and what opportunities existed for improvement. Several participants requested a “do-over,” knowing that they could do better; the team happily complied.
Uncover opportunities
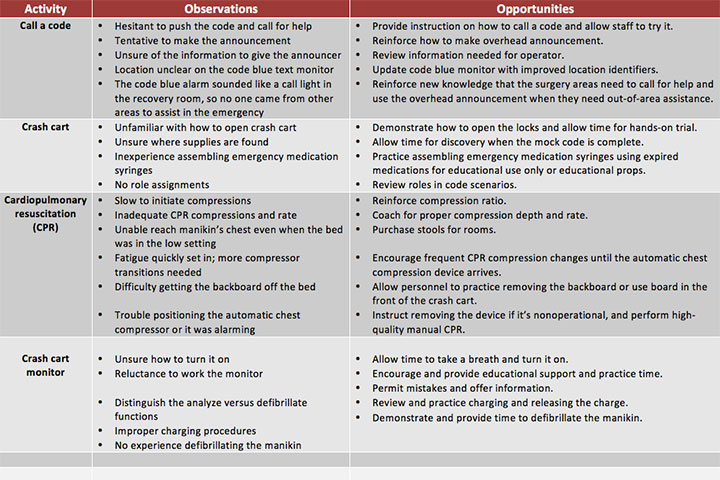
During each mock code, mistakes occurred, educational opportunities arose, teachable moments were taken advantage of—all leading to improved processes, enhanced teamwork, and increased staff confidence. (See Mock code observations and opportunities.) Some challenges required immediate action, and others took time to correct because of financial constraints or personnel capability. The team was prepared for this but surprised by the variety of items that needed attention and follow-up.
Mock code observations and opportunitiesDuring debriefing sessions after mock codes, the team and staff made several observations and discovered many opportunities for improvement. |
 |
One item that needed immediate attention was the information used to trigger the overhead announcement that calls responders to an emergency. The system sends a text message to a monitor at the reception area, which staff use to make code blue announcements. However, the monitor allowed a limited number of characters to identify the location, which meant that only the room number was announced, not the floor or department. As nurses know, a room number isn’t enough information to get responders to an emergency quickly. Through collaboration with leadership, facilities management, the biomedical department, and the quality coordinator, we created an identification process for all code blue buttons that includes announcing the floor, department, and room number—in that order—to direct emergency responders.
Share the outcomes
I shared the results of the mock codes at nursing leadership meetings and with the unit supervisors and managers. The time to activate a code blue in one hospital setting went from 4 minutes to less than 1 minute, and the start of CPR chest compressions decreased from 5 minutes to 1 minute. The most impressive outcome was the decrease in the amount of time to the first defibrillation, which improved by 6 minutes to a time of less than 4 minutes. We also shared the outcomes in the monthly newsletter and offered process updates. As changes were made, staff members were kept informed for future drills and real patient emergencies.
Celebrate the success
The goal of the mock code project was to improve initial staff response to emergencies, but it became much more. As the mock codes progressed, the focus shifted to the delivery of high-quality CPR, limited compression interruptions, proper hand placement, initiation of the automatic chest compression device, recognition of lethal heart rhythms, and administration of defibrillating shocks—all critical to improving cardiac arrest outcomes. The CAH nursing staff are more confident and better prepared to respond to emergency situations.
Deb Sitter is the clinical operations director at Lakeview Specialty Hospital & Rehab in Waterford, Wisconsin. This project was conducted at the critical access hospitals of Mercyhealth™ Hospital and Medical Center—Walworth in Lake Geneva, Wisconsin, and Mercyhealth™ Hospital and Medical Center—Harvard, in Harvard, Illinois.
Selected references
Herbers MD, Heaser JA. Implementing an in situ mock code quality improvement program. Am J Crit Care. 2016;25(5):393-9.
Johnson G. Before the code team arrives: Insitu simulations for non-code team staff. Clin Simu Nurs. 2012;8(8):e401.
Lavoie P, Clarke SP. Simulation in nursing education. Nurs Manage. 2017;48(2):16-7.
Rudy S, Rooney V, Westley-Hetrick, E. Mock codes in a radiology department for systems improvement and staff competency. J Radiol Nurs. 2015;34(4):193-9.
Strong J. Be prepared, not scared: Making the most of mock codes. J Radiol Nurs. 2016;35(2):151-2.

















