
Make a plan to protect yourself and your colleagues.
Takeaways:
- An organization-wide anonymous encrypted screening program to detect nurses at risk for suicide is an evidence-based approach to prevention.
- Speaking directly to a colleague about suicide can save a life: “Are you so sad that you feel like ending your life?”
- Taking a firearm out of the house of a depressed person who needs treatment can prevent suicide.
We know that suicide rates are higher in nurses than the general population, but we don’t yet know the exact reasons why. However, the nature of the work we do increases our risk of anxiety, stress disorders, and depression. The COVID-19 pandemic makes us even more vulnerable (as has been documented during previous disease outbreaks, such as Ebola virus disease). (See Nurse suicide risk factors.)
Nurse suicide risk factors
The following factors place nurses at risk for suicide:
- chronic pain
- depression
- evaluation for substance use disorder at work
- fear for safety or safety of others
- fear of harming a patient
- feeling out of place
- feeling unprepared for the role
- feeling unsupported in the role
- financial stress
- inadequate self-care
- isolation from family and friends
- job loss
- loneliness
A video (youtube.com/watch?v=A1M85tEa6JU) by Laurel Prince, MSN, RN, a trauma nurse, depicts the stress and burnout experienced by many nurses.
We haven’t yet overcome the stigma associated with seeking mental health treatment, but given the increased incidence of suicide among nurses, we need to change our perspective and normalize conversations about mental health and wellness. We must create atmospheres of acceptance and empathy within healthcare organizations and send the message to our colleagues that it’s okay not to be okay.
Not every suicide can be prevented, but accepting the fact that suicide happens is a necessary precursor to prevention. In this article, we’ll build on the resiliency strategies covered in the first article in this series on nurse mental health (myamericannurse.com/?p=70264). The goal is to empower you with concrete steps that will help you protect yourself and identify colleagues in crisis and to provide evidence-based actions you can take to ensure they get the assistance they need. (See Resources for help.)
Resources for help
If you or your colleagues are having thoughts of suicide, call on these resources for help.
Crisis: Thoughts of suicide or self-harm
- Call the National Suicide Prevention Lifeline: 1 800-273-TALK.
- Call 911 immediately.
- Contact your healthcare provider now.
Clinician friendly hotlines
- Safe Call Now (safecallnowusa.org). This crisis referral service supports public safety employees, emergency services personnel, and their families. 206-459-3020.
- Disaster Distress Helpline (samhsa.gov/find-help/disaster-distress-helpline). This 24/7, 365-day-a-year national hotline run by Substance Abuse and Mental Health Services provides crisis counseling for those in trauma-related emotional distress. Call 800-985-5990 or text TalkWithUs to 66746.
- Crisis Text Line (crisistextline.org). Trained crisis responders provide 24/7 support to frontline healthcare workers. In the United States and Canada text HOME to 741741.
Suicide prevention
American Association of Suicidology (suicidology.org) provides toolkits and other resources relevant to suicide prevention.
American Foundation for Suicide Prevention Community Programs (afsp.org/community-programs) provides community programs.
American Psychiatric Nurses Association (APNA) “Psychiatric-mental health nurse essential competencies for assessment and management of individuals at risk for suicide” (apna.org/m/pages.cfm?pageid=5684) outlines skills and competencies relevant to assessing and managing suicide risk.
Johnson & Johnson “Nurses on life support” (https://nursing .jnj.com/see-you-now-podcast/covid-19-the-nurse-responseon-life-support) is a 10-minute podcast about COVID-19 and nurse suicide.
Mental Health First Aid Australia “Suicidal thoughts & behaviours guidelines” (mhfa.com.au/sites/default/files/ suicidal_thoughts_and_behaviours_guidelines_0.pdf) outline risk factors, warning signs, and techniques for starting a conversation with someone who may be at risk of suicide.
National Academy of Medicine “Nurse suicide: Breaking the silence” (nam.edu/nurse-suicide-breaking-the-silence) is a discussion paper that includes individual prevention strategies and current statistics.
Sigma Theta Tau “Suicide in nursing: We are at risk” (nursingcentered.sigmanursing.org/features/more-features/suicide-innursing) offers reflections on nursing leadership and the Healer Education Assessment and Referral (HEAR) program.
Study: Nurses at greater risk of suicide than others (kpbs.org/news/2020/feb/20/ucsd-launches-suicide-prevention-program-address-h/) is a KPBS podcast episode that explains the HEAR program.
Suicide Prevention Resource Center “The role of co-workers in preventing suicide in the workplace” (sprc.org/sites/ default/files/resource-program/V11_Co-worker_May2018.pdf) includes steps for reducing suicide risk among work colleagues.
U.S. Department of Health and Human Resources “Identifying the relative importance of non-suicidal self-injury features in classifying suicidal ideation, plans, and behavior using exploratory data mining” (ncbi.nlm.nih.gov/pmc/articles/PMC6684203) looks at self-injury as a possible precursor to suicide.
U.S. Department of Veterans Affairs National Center for PTSD “Psychological first aid (PFA) online training” (www.ptsd.va.gov/professional/continuing_ed/psych_firstaid _training.asp) is a continuing education course for psychological first aid after a disaster or other trauma.
Zero Suicide (zerosuicide.edc.org) provides a framework for organization-wide safer suicide care, including toolkits, training, and podcasts.
Zero Suicide COVID-19 resources (zerosuicide.edc.org/ movement/innovations/covid-19) offers multiple resources specific to COVID-19 challenges.
Substance use
American Association of Nurse Anesthetists (AANA) “Substance use disorder workplace resources” (aana.com/ practice/health-and-wellness-peer-assistance/About-AANAPeer-Assistance/substance-use-disorder-workplace-resources) offer recommendations for addressing substance use disorder and ensuring patient safety.
AANA “Substance use disorder – Peer support: An empathetic information resource” (topmedtalk.libsyn.com/ website/topmedtalk-substance-use-disorder-peer-supportan-empathetic-information-resource-0) is a podcast that discusses how to address substance use disorder among healthcare workers.
APNA Substance use resources (apna.org/i4a/pages/index.cfm?pageid=4792) provide substance use statistics, screening tools, and other resources.
Lippincott NursingCenter “Programs and resources to assist nurses with substance use disorders” (nursingcenter.com/ journalarticle?Article_ID=3386413&Journal_ID=1444159 &Issue_ID=3386006) is an article from the Journal of Addictions Nursing that includes information about programs throughout the United States.
National Council of State Boards of Nursing (NCSBN) “Substance use disorder” (ncsbn.org/substance-use-disorder.htm) provides continuing education courses at no cost.
National Institute of Alcohol Abuse and Alcoholism Rethinking Drinking (rethinkingdrinking.niaaa.nih.gov) includes information about drinking levels, warning signs of a problem, and resources for making changes.
NCSBN “Alternative to discipline programs for substance use” (ncsbn.org/alternative-to-discipline.htm) includes stateby-state information about these programs.
NCSBN “Understanding substance use disorder in nursing (ncsbn.org/5127.htm) is a free course that discusses substance use and abuse, early identification and intervention, how to protect the public, treatment, and return to practice.
U.S. Department of Health and Human Resources “Facing addiction in America: The Surgeon General’s report on alcohol, drugs, and health” (ncbi.nlm.nih.gov/books/ NBK424857/pdf/Bookshelf_NBK424857.pdf) reviews substance use disorder and opportunities to bring treatment and mainstream healthcare into alignment.
Be aware, identify, and recognize
Most people who are having suicidal thoughts are in too much distress to get help on their own. Their view of the world becomes myopic and focused on the negative. They need a friend or colleague to encourage them to use resources to seek help or to even make the call for them. Nurses aren’t immune to the effects of depression, and we’re socialized to “buck up and take it,” making it difficult for us to recognize overwhelming feelings of sadness or depression in ourselves, or that we’ve reached the point where we can’t function. However, we can help each other if we know what to do and how to take action to save a life.
Use the acronym AIR (Awareness, Identify, Recognize) to help you identify colleagues who are at risk.
Awareness
Be aware of the warning signs frequently seen in someone in crisis. Listen for them during conversations with colleagues and watch for behavior changes. (See Crisis warning signs.)
Crisis warning signs
Watch for these crisis warning signs to help prevent suicide.
- Acting anxious, agitated, or unusually angry
- Erratic or unusual behavior
- Extreme mood swings
- Giving away belongings
- Increasing use of alcohol/drugs
- Looking for a suicide method (for example, searching online)
- Rumination (can’t get rid of negative thoughts)
- Self-injury (for example, cutting)
- Sleeping too much or too little
- Talking about feeling hopeless, having no reason to live
- Talking about feeling trapped or being a burden to others
- Talking about unbearable physical or psychological pain
- Talking, writing, or creating art about wanting to die or kill themselves
- Withdrawal or isolation
Because someone can have suicidal thoughts and not display any noticeable signs, regularly check in with colleagues, giving them space to discuss their feelings. Open the door by asking, “I’ve noticed you’re more down than usual. Do you want to talk about it?”
Identify
Your awareness of the warning signs and the conversations you have with colleagues will help you identify when someone is at risk of suicide.
Have the conversation. The most important thing you can do is start a conversation. Empathy makes a powerful connection to reduce the risk of loneliness. Direct questions can be lifesaving. (See Key conversation elements.)
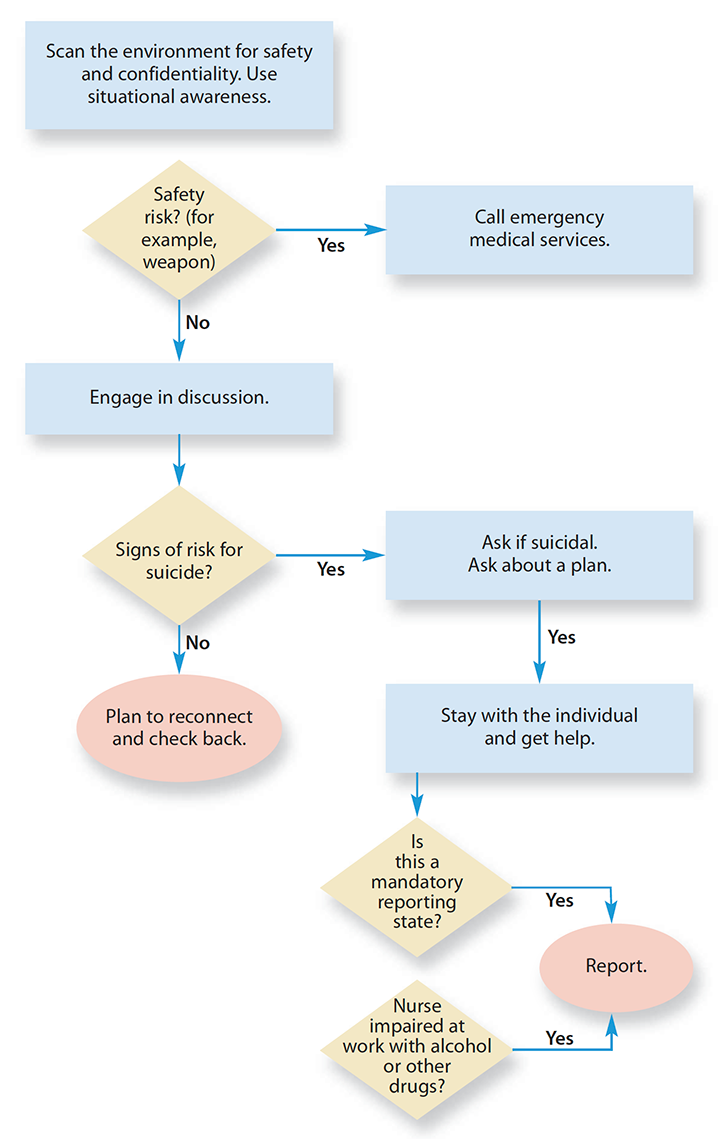
Key conversation elements
Use this algorithm to guide your conversation with a colleague who might be at risk of suicide.
Motivational interviewing can help, especially if your colleague is ambivalent about making change. This nonjudgmental conversational style uses empathy and collaboration to strengthen a person’s motivation for commitment and change. The discussion becomes a partnership and focuses on next steps. You assume the position of the learner, not the teacher, where you ask about goals and what could be done next, rather than telling your colleague what to do. This approach may encourage them to be more open to seeking help. (See Conversation dos and don’ts.)
Conversation dos and don’ts
When talking to a colleague you fear may be having suicidal thoughts, use this list of dos and don’ts to ensure you’re providing a nonjudgmental space for them to express their feelings and experiences.
Do
- provide empathy
- listen authentically
- be a friend or colleague
- be curious (“Tell me more.”)
- use silence to help them open up
- have the moral courage to ask the question, “Are you thinking about suicide?”
- paraphrase back what you’ve heard (“It sounds like your workload is causing you a lot of stress at home.”)
- name emotions (“I hear that you’re sad.”)
- make an appointment to talk again if they don’t need crisis intervention.
Don’t
- try to fix the problem
- be a teacher or therapist
- minimize (“It’s not that bad.”)
- assume you know how they’re feeling
- try to find a silver lining (“At least you have a job.”)
- make it about you
- try to change what they’re feeling
- leave the person alone if they’ve admitted an intent to self-harm.
To better understand empathy, view the video at youtu.be/1Evwgu369Jw. Learn more about motivational interviewing at sciencedirect.com/topics/medicine-and-dentistry/motivational-interviewing.
Learn evidence-based communication skills. Training is available on peer suicide evaluation and self-screening tools. Here are three examples:
- A series of eight videos prepared by Sharon Tucker, PhD, RN, is available to the public and provides examples of words to say to someone you think is at risk of suicide. u.osu.edu/cliniciansindistress/videos
- The American Foundation for Suicide Prevention (AFSP) developed “Have a #RealConvo,” which includes guidance and real stories using lay language to help anyone learn how to talk to someone they think may be at risk of suicide. https://afsp.org/realconvo
- A video from AFSP describes how to bring up the conversation and why. An opener like this can help start the conversation: “The way you’ve been talking lately really concerns me [pause] can we talk? I’m here for you.” afsp.org/healthcare-professional-burnout-depression-and-suicide-prevention
Implement proactive screening. A proactive approach to regular screening can help you identify colleagues with mental health conditions or risky substance use before it becomes a matter of suicidal ideation or legal action. The Healer Education, Assessment and Referral (HEAR) program (based on AFSP’s Interactive Screening Program afsp.org/interactive-screening-program) provides a comprehensive tool that can be deployed by any organization to proactively evaluate the suicide risk of faculty, employees, and students. This anonymous, encrypted survey is sent via a simple email with a link. The organization must have therapists on hand to engage through encrypted email and a referral system for those identified as at-risk. This process is cost-effective, can be scaled to any size or type of organization, and has been successfully transferring clinicians who are depressed and suicidal into treatment for over 10 years.
Recognize
Recognize the urgency to intervene. Once you’ve seen the warning signs, don’t hesitate. Assume you’re the only one who has noticed the colleague in distress and speak up. If something is making you feel that a colleague is in trouble, speaking up could save their life. If you’re wrong and they’re okay, you’ve opened the door to future conversations because they know you care.
Recognize when to treat the situation as an emergency. When someone says they’re thinking about suicide, always take them seriously. If at any point you have doubts about whether the person can stay safe (keep in mind a safety plan doesn’t guarantee safety), don’t leave them alone. Discuss your concern with them and give them the opportunity to choose to go to the hospital, but be prepared to call 911. Although making that call is difficult, especially when you have a relationship with the individual in crisis, it must be part of your plan. Relationships can be repaired. Life can’t be restored. Make the call.
Safety planning
Every nurse should create a safety plan for themselves. Self-care and talking about your problems with a trusted coworker, family member, or friend are excellent ways to help you deal with stress and anxiety. Encourage your colleagues to do the same.
Being familiar with your resources makes it more likely that you’ll use them when a crisis occurs. Your safety plan should include knowing suicide risk warning signs and the coping strategies that work best for you, including the people who can help calm or distract you. Your plan also should include maintaining in your contacts the names and numbers of people to call for help as well as emergency phone numbers. The Suicide Prevention Lifeline offers a Patient Safety Plan Template (bit.ly/3mvblGF), and Staying Safe from Suicidal Thoughts has a quick online plan (https://stayingsafe.net/node/7) to help start the process.
After you’ve completed your own safety plan, you’ll be better prepared to help colleagues develop theirs. Safety plan prompts about resources—such as “Who do you normally go to when things get rough?” “What activities normally calm you down when you’re stressed?”—also can help you during conversations with colleagues who’ve become tunnel-visioned by stress or depression to remind them of help they may not have accessed.
Removing access to means: Firearm and medication safety
Suicide frequently is impulsive. Removing immediate access to lethal methods—such as firearms and medications—reduces the likelihood that an individual having suicidal thoughts will act impulsively and increases the chance that they’ll seek help instead.
The use of firearms by nurses who die by suicide is rising, so any screening should include a direct question to determine whether the person has access to a firearm. Removing firearms from the home during treatment for depression is an evidence-based strategy to reduce suicide incidence. The same is true of medications. If someone you know has talked about a suicide plan that involves medications found in the home, remove the medications.
When medications or firearms can’t be removed from the home, steps can be taken to store them in a safe.
Nurses who are gun owners are encouraged to follow firearm safety recommendations. Store firearms locked and unloaded, and store ammunition separately from firearms. Using firearm safety precautions may save the life of a friend or family member. (See Firearms and medication safety resources.)
Firearms and medication safety resources
Reducing access to lethal methods is key to suicide prevention. These resources offer information, toolkits, and training.
- American Foundation for Suicide Prevention (AFSP): Firearms and suicide prevention (afsp.org/firearms-and-suicide-prevention).
- National Shooting Sports Foundation (NSSF): Suicide prevention program (nssf.org/safety/suicide-prevention/suicide-prevention-toolkit/). A toolkit developed through a partnership between NSSF and AFSP to promote suicide prevention through firearms safety.
- Suicide Prevention Resource Center: CALM (Counseling on access to lethal means) (sprc.org/resources-programs/calm-counseling-access-lethal-means). A training course that includes how to identify people who might benefit from lethal means counseling, ask about access to lethal methods, and work with them to reduce access.
- U.S. Department of Health and Human Resources: How to safely dispose of drugs (hhs.gov/opioids/prevention/safely-dispose-drugs/index.html). Provides information about safe medication storage and disposal.
Risky substance use and substance use disorder
Risky substance use is best understood on a continuum, where one end represents little use and little risk of harm and the other represents acute addiction and extreme risk for harm. In the middle of the continuum, many people use substances in a way that negatively impacts their well-being and increases the risk for addiction.
 Substance use in the nursing profession is especially challenging because of the potential for harm not only to yourself but also to patients. The first step is to understand your own risks and honestly evaluate your substance use. Risky substance use and substance use disorder can be detected using common assessment tools, which are available from the National Institute on Drug Abuse at drugabuse.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools.
Substance use in the nursing profession is especially challenging because of the potential for harm not only to yourself but also to patients. The first step is to understand your own risks and honestly evaluate your substance use. Risky substance use and substance use disorder can be detected using common assessment tools, which are available from the National Institute on Drug Abuse at drugabuse.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools.
After you’ve evaluated your own risk, think about how to support your colleagues with risky behaviors. Approaching a colleague early in the substance use continuum makes it more likely that they’ll get help before they’re found impaired at work, diverting medications, or driving under the influence. A conversation between friends—using motivational interviewing techniques and reflective listening—in which you share your feedback and concerns can be an effective way to open the door to help.
If a nurse is found impaired at work, your options are limited and guided by your state’s reporting mandates. For patient safety, the situation must be reported to a manager who will remove the nurse from duty and then follow the organization’s process. Ethically, we have a duty to support the nurse through treatment and welcome them back to the workforce when treatment is completed.
Nurses die by suicide during formal investigations for substance use disorder. Talking to a colleague who’s struggling with risky behavior before they’re found impaired on the job can save a life.
Speak with empathy
Suicide prevention requires that we overcome the stigma associated with mental health concerns and instead view the stress, anxiety, and depression we sometimes experience as part of being human. We must be open to discussing our emotions and actively listening to someone who may be at risk for suicide. Save a life by learning the skills to speak empathically with a colleague you’ve identified as being at risk.
Judy E. Davidson is a nurse scientist at the University of California San Diego Health and in the department of psychiatry at the University of California San Diego School of Medicine. Amanda Choflet is an assistant professor at the San Diego State University School of Nursing in San Diego, California. M. Melissa Earley is a mental health professional and nurse consultant in Richmond, Virginia. Paul Clark is an assistant professor in the school of nursing at the University of Louisville in Louisville, Kentucky. Sattaria Dilks is president of the American Psychiatric Nurses Association in Falls Church, Virginia. Linda Morrow is a clinical associate professor at Sacred Heart University College of Nursing in Fairfield, Connecticut. Sharon Tucker is the Grayce Sills Endowed Professor of Psychiatric Mental Health Nursing at The Ohio State University College of Nursing in Columbus. Trisha Mims is director of program and education at the National Student Nurses Association in New York City, New York.
To learn about suicide prevention in the educational setting and access additional resources, as well as creative expressions related to this issue, visit myamericannurse.com/?p=72015.
The painting on the first page of this article is “Dread” by Sarah Pai, MSN, APRN, PMHNP-BC.
References
Burke TA, Jacobucci R, Ammerman BA, et al. Identifying the relative importance of non-suicidal self-injury features in classifying suicidal ideation, plans, and behavior using exploratory data mining. Psychiatry Res. 2018;262:175-83.
Coleman D, Black N, Ng J, Blumenthal E. Kognito’s avatar‐based suicide prevention training for college students: Results of a randomized controlled trial and a naturalistic evaluation. Suicide Life Threat Behav. 2019;49(6):1735-45.
Davidson JE, Proudfoot J, Lee K, Terterian G, Zisook S. A longitudinal analysis of nurse suicide in the United States (2005–2016) with recommendations for action. Worldviews Evid Based Nurs. 2020;17(1):6-15.
Davidson JE, Accardi R, Sanchez C, Zisook S, Hoffman LA. Sustainability and outcomes of a suicide prevention program for nurses. Worldviews Evid Based Nurs. 2020;17(1):24-31.
Dickens C, Guy S. ‘Three minutes to save a life’: Addressing emotional distress in students to mitigate the risk of suicide. Mental Health Practice. March 11, 2019.
Goetz CS. Are you prepared to S.A.V.E. your nursing student from suicide? J Nurs Educ. 1998;37(2):92-95.
Leal SC, Santos JC. Suicidal behaviors, social support and reasons for living among nursing students. Nurse Educ Today. 2016;36:434-8.

















