
Controlling symptoms and preventing exacerbations are the key to patient quality of life.
Takeaways:
- Nurses must be able to identify patients with chronic obstructive pulmonary disease (COPD) early in the disease process to provide education that helps prevent exacerbations, decreases co-morbidities, and improves quality of life.
- Patient history is crucial in the early stages of COPD because the physical exam may not reveal many abnormal findings.
- Nurses play an important role throughout COPD treatment, educating patients, assisting with medication plans, and helping to prevent exacerbations.
 ACCORDING TO the Centers for Disease Control and Prevention, chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death in the United States. The World Health Organization reports that it’s the third leading cause of death in the world and that worldwide COPD mortality in both high- and low-income countries is expected to double by 2030. The condition also contributes to other diseases, such as coronary artery disease and hypertension.
ACCORDING TO the Centers for Disease Control and Prevention, chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death in the United States. The World Health Organization reports that it’s the third leading cause of death in the world and that worldwide COPD mortality in both high- and low-income countries is expected to double by 2030. The condition also contributes to other diseases, such as coronary artery disease and hypertension.
The multifaceted pathophysiology of COPD causes progressive symptoms that require comprehensive management. (See Pathophysiology.) Nurses care for patients with COPD in a variety of outpatient settings (home, pulmonary rehabilitation, and clinics); acute care settings are reserved for those who are acutely ill. It’s important that nurses be able to identify patients with COPD early in the disease process and provide education to help prevent exacerbations (sudden worsening of respiratory symptoms that requires additional treatment or therapy), decrease comorbidities, and improve quality of life.
Causes and risk factors
Long-term exposure to irritants that damage the lungs and airways is the most common cause of COPD, and cigarette smoke (from smoking or secondhand smoke) is the most common irritant. Other irritants include particles from fires used in the home for cooking or heating and workplace exposure to chemical fumes, dust, and particles. Occupational exposures often are overlooked and underdiagnosed. COPD risk increases when those exposed to lung irritants in the home or at work also smoke.
Some people carry a rare familial gene (alpha-1 antitrypsin) that predisposes them to COPD-type lung damage. Testing is available to identify those with the gene so treatment can be started to halt the damage. However, once the injury occurs, it can’t be reversed. Other factors that contribute to COPD include low birth weight, a diet low in fruits and vegetables, and poverty.
Signs and symptoms
A patient in the early stages of COPD may report cough and sputum production, but he or she may dismiss the symptoms as “typical” of smoking. Worsening symptoms include shortness of breath with exertion and wheezing with or without exercise, and many patients report that they catch respiratory illnesses easily and don’t recover as quickly as they did in the past. Late-stage symptoms include continuous shortness of breath (even at rest) and fatigue. Patients also may report chest pain because of muscle strain related to the increased work of breathing. As the disease progresses, patients may begin to report problems sleeping and may need to sleep upright to feel comfortable. Depression symptoms are common in patients with COPD, so depression screening is recommended. Comorbidities include hypertension and heart failure as well as gastro esophageal reflux disease and diabetes. Patient history is crucial in the early stages of COPD because the physical exam may not reveal many abnormal findings. (See Monitoring symptom impact.)
Physical assessment
Physical assessment findings may remain normal for many patients in the early stages of COPD. As the disease progresses, oxygen saturation may decrease with exertion only to improve again at rest. Lung sounds may reveal rhonchi or wheezes only during illness or exacerbations and then return to normal. As the disease progresses, patients with COPD may have diminished breath sounds in the lower lobes of both lungs.
Later-stage physical exam findings include a round “barrel chest” caused by chronic hyperinflation of the lungs. The patient may sit or stand in a tripod position (leaning forward and supporting the upper body with hands on the knees or another surface). This classic respiratory position is used for comfort because accessory muscles are needed to help open the lungs. As the work of breathing becomes more difficult, the patient’s caloric requirements increase. Nurses should ask focused questions about the patient’s dietary habits; patients who are short of breath may struggle to eat traditional meals and begin to lose weight.
Ankle and pedal edema also may be noted because of decreased physical activity and increased work on the right side of the heart. Lung sounds in the late stages of COPD may be decreased or exhibit wheezing due to alveolar collapse. The physical assessment also should include any systems (GI, cardiovascular, neurologic, and musculoskeletal) related to possible comorbidities.
Chronic obstructive pulmonary disease (COPD) begins in susceptible individuals whose lungs are repeatedly exposed to irritants, which sparks an inflammatory response.
• Damage occurs to the lungs’ medium and small airways that lead to the alveoli, where oxygen exchange takes place. Over time, the bronchial tree’s smooth muscle becomes more rigid (fibrotic), leading to progressive airway narrowing.
• Increased mucous production begins, clogging larger airways and elevating neutrophils. Cilia stop working efficiently, which leaves mucous trapped in the lungs. The increased mucous coupled with bronchial fibrosis contribute to progressively narrowing airways.
• Alveoli are damaged as inflammatory cells break apart the individual alveolar units, resulting in the loss of useful alveoli for oxygen and carbon dioxide exchange. Patients exhibit signs of decreasing oxygenation, and air becomes trapped inside the increasingly narrowing airways.
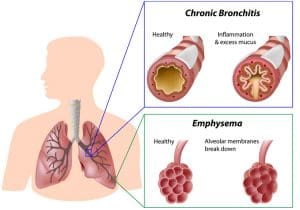
Chronic bronchitis and emphysema
The two types of COPD are chronic bronchitis and emphysema. The conditions are distinguished by history, symptoms, and diagnostic pulmonary function testing.
• A patient is diagnosed with chronic bronchitis if he or she has a productive cough that lasts for more than 3 months in 2 consecutive years.
• In emphysema, air is trapped in the damaged areas of the lungs. The buildup during expiration leads to lung hyperinflation.
Inflammatory changes occur with both chronic bronchitis and emphysema. However, emphysema is marked by damage to the alveoli while chronic bronchitis is characterized by cough and increased mucous production.
Diagnosis
COPD is diagnosed through a combination of patient history, physical assessment, and spirometry. Guidelines and recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the American Thoracic Society/European Respiratory Society (ATS/ERS) endorse spirometry for diagnosis.
Chest x-rays, although frequently ordered for patients with COPD, typically are used to rule out other causes of shortness of breath. Highresolution computed tomography scans aren’t currently recommended as a screening or diagnostic tool for all patients with COPD; however, they may be used for some patients. Arterial blood gases help determine blood oxygen and carbon dioxide levels for patients experiencing exacerbations, but they aren’t a standard diagnostic tool.
GOLD standard
GOLD is an international organization composed of health professionals who provide education and evidence-based guidelines focused on the care and prevention of COPD. The organization recommends evidence- based guidelines that include outpatient and inpatient care strategies to reduce respiratory exacerbations and improve patient-perceived quality of life.
Patients are classified into treatment groups based on spirometry scores (which are given a number designation from 1 to 4) and how many respiratory exacerbations they’ve had in the past year combined with a quality-of-life symptom screening tool score (which are given a letter designation from A to D). A higher number indicates airflow limitation. A and B indicate no more than one exacerbation per year; C and D indicate two or more exacerbations in a year. A and C indicate lower quality-of-life symptom scores and B and D represent higher scores. For more information, refer to the GOLD pocket guide.
Outpatient management
When COPD exacerbations occur, lung function is lost and doesn’t return, so treatment focuses on preventing and minimizing them. Nurses play an important role throughout treatment, educating patients, assisting with medication plans, and helping to prevent destructive exacerbations.
Primary interventions
All patients with COPD are encouraged to remain current with recommended immunizations, including a yearly flu vaccine to prevent infection and subsequent COPD exacerbations. Currently, two pneumococcal vaccines (PPSV23 and PCV13) are recommended for all patients over 65 years old and any patient with COPD. Patients who’ve never received a pneumococcal vaccine should start with PCV13, get the PPSV23 a year later, and then alternate the vaccines each year going forward. For more information about pneumococcal vaccine protocols, visit cdc.gov/pneumococcal/vaccination.html.
All treatment plans for patients with COPD who smoke must include smoking cessation. The United States Preventive Services Task Force recommends that all adults should be asked about tobacco use, and any patient who smokes should be advised to stop and offered a cessation method. Research indicates that a combination of behavioral interventions and medications is more successful than either method alone.
All inhalant exposure should be minimized. Workers with occupational risk must wear adequate protective masks to protect them from fumes, dust, and vapors. Wood or biofuel stoves should vent outside and remain tightly sealed to prevent leaks indoors.
GOLD guidelines recommend frequent monitoring for all comorbidities, such as heart failure and gastroesophageal reflux disease, that can exacerbate COPD symptoms. Worsening shortness of breath and decreased mobility related to COPD can contribute to hypertension and diabetes.
Scientifically validated and standardized screening questionnaires are recommended to assess chronic obstructive pulmonary disease (COPD) symptoms and learn how they’re affecting a patient’s daily life. These tools examine:
• symptom control
• activity level
• quality of life.
They can be self-administered by the patient in a provider’s office or by a nurse during a bedside assessment.
COPD Assessment Test
One example of a screening tool is the COPD Assessment Test. This eight-question survey is recommended for use with the current Global Initiative for Chronic Obstructive Lung Disease guidelines and has been validated in multiple languages. Access the tool at www.aafp.org/afp/2013/1115/afp20131115p655-fa.pdf
Medications
The COPD medication plan is dedicated to preventing exacerbations and reducing symptoms. Medicationbased treatments using the GOLD recommendations begin with the patient’s classification, which helps providers identify the initial medications. Nurses should confirm that patients understand their medication regimen and are using their inhaled medications correctly. Bronchodilators. Bronchodilators, delivered via inhaler or nebulizer, are recommended for all patients with COPD to relieve shortness of breath. Short-acting bronchodilators have a rapid onset and typically offer symptom relief for 4 to 6 hours. Long-acting beta agonists and antimuscarinic antagonists are taken once or twice a day based on the medications’ length of action. For patients with worsening symptoms, short- and long-acting bronchodilators can be used in combination.
Inhaled corticosteroids. According to the GOLD guidelines, patients with more than two exacerbations in the past year or one that led to a hospitalization may benefit from adding inhaled corticosteroids (ICSs) to long-acting bronchodilator therapy. This combination is recommended only for treating COPD, and ICSs should be used with caution because they increase the risk for pneumonia in patients with worsening respiratory disease.
Other medications. As patient symptoms progress, other classes of medications may be added. Regular use of macrolide antibiotics have been recommended to decrease possible exacerbations. Xanthine derivatives, such as theophylline, are used for select patients who require additional symptom relief with a centrally acting bronchodilator. Theophylline requires regular blood monitoring for drug levels, but it continues to be a valid option for some patients because of its effectiveness and lower cost.
Tertiary interventions
The GOLD guidelines recommend physical activity for patients with COPD. Although the specific length and level of exertion are debated, patients should be encouraged to continue physical activity as tolerated. Physical activity and nutrition education provided early in the disease gives patients a strong foundation for long-term success. Nurses also should provide support to help patients learn how to self-manage their conditions.
Pulmonary rehabilitation referrals are recommended at COPD diagnosis, after a hospitalization, and after exacerbations. Pulmonary rehabilitation offers a structured environment where patients can participate in monitored exercise training, smoking cessation, nutritional support, and education while under their medical team’s care. Patients who’ve participated in pulmonary rehabilitation report reduced shortness of breath and better quality of life, especially when therapy is performed before the disease state is severe. Nurses can educate patients about the benefits of pulmonary rehabilitation and advocate for early referral to providers.
Long-term oxygen therapy may be required for some patients with COPD. Current recommendations include continuous oxygen use (> 15 hours/day) for patients whose resting arterial oxygen saturation (SaO2) is less than 88%. Oxygen alone won’t improve shortness of breath for patients who don’t have a decreased SaO2; however, oxygen therapy can improve survival for patients with severe resting hypoxia.
Exacerbations must be quickly identified and treated. Nurses should teach patients about when and where to seek care. Patients should call their primary care or pulmonology provider to seek guidance when early symptoms occur. Mild exacerbations frequently can be managed as an outpatient with increased inhaled medications and oral corticosteroids. However, symptoms such as severe shortness of breath and difficulty breathing should be evaluated quickly. More severe symptoms may require hospitalization for stabilization.
Vital care
Nurses provide vital education and care coordination for patients with COPD to prevent costly and lifethreatening exacerbations. Patients and families need additional support and education as symptoms progress, and nurses can teach them about complicated medication regimens and comorbidities, help them navigate the healthcare system, and provide opportunities for end-of-life conversations that allow them to make the best care choices.
Erin Morgan is a clinical assistant professor at the University of Tennessee in Knoxville.
Selected references
Centers for Disease Control and Prevention. National Center for Health Statistics: Chronic obstructive pulmonary disease. May 3, 2017. cdc.gov/nchs/fastats/copd.htm
Centers for Disease Control and Prevention. National Center for Health Statistics: Leading causes of death. March 17, 2017. cdc.gov/nchs/fastats/leading-causes-of-death.htm
Centers for Disease Control and Prevention. Pneumococcal vaccine timing for adults. November 30, 2015. cdc.gov/vaccines/vpd/pneumo/downloads/pneumo-vaccinetiming.pdf
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2018. goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf
Patnode CD, Henderson JT, Thompson JH, Senger CA, Fortmann SP, Whitlock EP. Behavioral counseling and pharmacotherapy interventions for tobacoo cessation in adults, including pregnant women: A review of reviews for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;163(8):608-21.
Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: A clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179-91.
Rossi A, Butorac-Petanjek B, Chilosi M, et al. Chronic obstructive pulmonary disease with mild airflow limitation: Current knowledge and proposal for future research—A consensus document from six scientific societies. Int J Chron Obstruct Pulmon Dis. 2017;12: 2593-2610.
Russell REK, Ford PA, Barnes PJ, Russell S. Eds. Managing COPD. 3rd ed. London, England: Springer Healthcare Ltd; 2013.
World Health Organization. Projections of mortality and causes of death, 2016 to 2060. who.int/healthinfo/global_burden_disease/projections/en
















