
Save time, increase intervention efficiency and effectiveness, and enhance patient safety.
Takeaways:
- Care managers spend hours cross referencing multiple sources to gather as much information as possible about a patient.
- Risk scores help predict future costs and events, but the algorithm and outreach score developed by this team of nurses looks at various factors in the patient’s current health status to determine who will benefit most from care coordination services right now.
Using early identification of at-risk or vulnerable patients and ensuring they receive the right care at the right time, accountable care organizations (ACOs) decrease unnecessary medical costs via a patient-centered care coordination (CC) approach. Care managers (CMs), usually RNs, coordinate the health and wellness of ACO patients via interventions based on individualized health plans that assess various factors, including chronic disease management, social determinants of health, and behavior modification. As appropriate, other healthcare professionals participate in this process. However, various risk-based stratification methodologies can complicate the identification of populations that would most benefit from CC services.
For example, risk scores determine a patient’s expected medical cost compared to the average. Insurance companies, population health applications, and ACOs create their own risk scores, with no single gold standard. The basic components include clinical information, costs, and patient demography. CMs find this information useful when the goal is to reduce the risk of future unfavorable events. However, this leaves patients with various noncomparable scores that don’t provide a holistic representation of their health, which complicates prioritizing patients for outreach. Prusinski also notes that risk scores don’t consider factors outside of diagnosed medical conditions and don’t always lower costs. The focus on cost detracts from, and frequently completely eclipses, behavioral health factors, patient adherence, and other environmental influences.
One ACO developed an outreach score using an alternative to the standard risk stratification. It helps stratify all attributed patients for CC outreach. Rather than predicting the likelihood of future events, the outreach score (based on immediate individual patient clinical need) creates clinical prioritization. Typically, CMs leverage multiple sources to identify patients eligible for outreach, and yet another to gather clinical data. Creating an outreach score prevalidates all data sources and marries the clinical criteria, which removes CM administrative burden and allows them to manage their time more efficiently.
How we did it
The team (nurses with experience in public health, data and analytics, and care coordination) that developed the outreach score didn’t require institutional review board approval because patients had already consented to providing the organization with claims data and information from the regional health information exchange.
Because of patient complexity and volume, we first applied the outreach score algorithm to the ACO’s government-sponsored Medicare population. A unique component included in this algorithm, and not in risk score equations, is socio-economic status (SES). Using the U.S. News & World Report Healthiest Communities tool, we obtained county-level SES data. We used these data rather than zip codes because 2010 and 2020 census data weren’t publicly available. The tool ranked 10 areas of health and health-related categories on a scale from 1 to 100 (100 being the best score possible). The calculated average score yielded the overall county score. We performed the calculation to generate our own SES score: SES score = 100 / sum of the 10 individual categories.
We devised the SES calculation to provide an inverse measure, so that patients with the highest outreach scores are those deemed the most in need of CM services. As an inverse measure, counties performing poorly yield higher SES scores. We assumed that counties with higher SES scores would be in poorer health than those with lower scores. We later included this as part of the equation to determine a patient’s final outreach score. Several studies have looked at how the SES of an individual’s neighborhood (for example, lack of healthy food options, little space to exercise, and high crime levels) can significantly affect health.
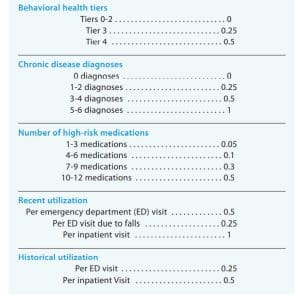
The algorithm incorporates five additional areas: historical healthcare utilization, recent healthcare utilization, chronic disease diagnosis, pharmacy data, and patient demographics. The analytics department and CC directors collaborated to assign weights to variables within each area, summed, multiplied by the SES score, then divided by 10 for the final score. (See Weighing variables.)

Historical and recent healthcare utilization
Historical utilization, derived from paid claims data, included the date of the last Medicare annual wellness visit, the number of emergency department (ED) visits, and the number of inpatient admissions in the previous 12 months. We collected recent utilization data from the health information exchange, which circumvents the 90-day claims lag and allows for real-time interventions. Recent utilization data included the number of ED visits, ED visits with falls, and inpatient admissions in the previous 45 days. Recent utilization carried a double weight compared to historical utilization due to the likelihood for increased risk of readmission.
Chronic diseases
Chronic diseases included in the outreach score included asthma, coronary artery disease, heart failure, chronic obstructive pulmonary disease, diabetes, and hypertension. We assigned points based on the number of chronic diseases. We excluded end-stage renal disease (ESRD) because these patients typically are managed by a specialized care team and wouldn’t benefit more from CM interventions. We also excluded patients who received hospice during the previous 12 months.
Pharmacy data
We used claims to obtain patient medication lists for the previous 12 months. Medications were grouped into one of 12 classes previously identified as high-risk per the ACO’s pharmacy program. We discarded medications that didn’t fall into one of these classes and segmented the number of high-risk medications (1–3, 4–6, 7-9, 10–12). We then assigned weights based on the numbers of high-risk medications the patients is taking. Patients prescribed more high-risk medications receive more points in their outreach score calculation.
Patient demographics
Patient demographics included in the algorithm included age, dual-eligibility status (patients eligible for both Medicare and Medicaid), frailty status, and behavioral health tiering. We devised age bands with 10-year cut-points, with more weight allocated to younger patients because most people under 60 don’t qualify for Medicare unless they have a severe health condition. We assigned points only to dual-eligible patients (those who weren’t dual eligible received no points). Frailty encompasses 12 indicators (abnormal gait, muscle weakness, walking difficulty, falls, durable medical equipment use, debility, cachexia, protein–calorie malnutrition, pressure injury, muscle wasting/disuse atrophy, adult failure to thrive, and senility without psychosis), the tally of which determined the number of points assigned.
Race alone doesn’t indicate health, so we excluded it. In the ACO’s service area, more Blacks and Hispanics, compared to Whites, live in lower-income urban neighborhoods that lack access to high-quality employment and educational opportunities, space for physical activity, healthy and safe housing conditions, and healthy food options. All of these factors contribute to an individual’s health, but applying points based solely on race would be inequitable because multiple races can and do live in the same community and they’re all affected by the same environmental factors.
Behavioral health
We categorized behavioral health into four tiers based on the number and type of mental health diagnoses, psychiatrist visits, and behavioral health hospitalizations. Higher tiers (which received more points) contain more severe diagnoses and utilization. Including this variable in the algorithm uncovered frequently overlooked behavioral health issues, prompting CMs to include wraparound services as appropriate.
Many studies have considered the correlation between SES and behavioral health, but only recently has society started to acknowledge the importance of mental health as much as physical health. An inability to manage one’s mental and behavioral health disorders can lead to struggles at work that result in unemployment, failure to care for oneself, increased healthcare utilization and costs, poverty, and suicide.
What we discovered
Our data review revealed an average patient age of 73 years, with 23% over 80, and only 7% younger than 60. Two counties contain 63% of the ACO’s population. Most (76%) of patients weren’t dual eligible, and about 84% had no frailty indicators. Over three-quarters of the patients were prescribed at least one high-risk medication.
The Centers for Medicare and Medicaid Services calculates the Medicare risk score (provided to ACOs enrolled in Medicare value-based programs) based on patient gender, age, conditions and hierarchical condition category, and disability status. The risk score solely focuses on a patient’s likelihood of future spend derived from previous clinical markers, which excludes their current clinical needs, updated status, and external environment. We calculated the total medical costs for each score category based on each patient’s medical costs for the previous 12 months. Two recognized approaches exist for determining patient outreach: medical cost or risk score. When using total medical cost based on risk score, the lower-risk score categories require the most attention due to their high spend. However, with the outreach score, total medical costs indicate that CMs should prioritize rising-risk patients who may become high risk if their conditions aren’t managed properly. These patients can be costly, but not costly enough to be carved out of the total medical costs at the end of the calendar year.
We adjusted for the volume of patients in each score category as we calculated average medical cost. As expected, when segmented by outreach score, average medical costs steadily increased with increasing score category.
When segmenting the scores by low-risk (0.0 – 2.99), rising-risk (3.0 – 5.99), and high-risk (6.0+), 37.4% of patients fall into the low-risk category when using the outreach score vs. 95.3% when using the Medicare risk score. This means that less than 5% of the population is considered rising- or high-risk, which doesn’t create a large enough caseload for the CM, resulting in picking and choosing from thousands of low-risk patients. The outreach score resulted in 50.9% of patients falling into the rising-risk segment. More patients included in the CMs’ caseloads can influence the bottom line.
From 2020 (no outreach score) to 2021 (first year outreach score was available), we saw a 55% increase in wrap-around service referrals. Of the 17 programs with referrals in 2020 and 2021, the largest increase was to specialists (800.0% increase), followed by food programs and nutrition counseling (400.0%). Other notable increases were to hospice (80.0%), services to support aging (77.8%), durable medical equipment (71.4%), and home health (60.9%).
An additional 12 programs received referrals in 2021 that hadn’t received any referrals the year before. Of these, 74.1% were to social and behavioral health services. Other noteworthy referrals included transportation, fall prevention, and caregiver services. CMs referred a total of 27 programs during 2021.
How we applied what we learned
The primary purpose of the outreach score was to answer the question, “Who should I reach out to first?” Rather than trying to predict future events, we aimed to implement a real-time holistic approach for identifying patients whose quality of life might be most improved with individualized clinical support and wrap-around services. The results include streamlined workflows, appropriate interventions and wrap-around service referrals, enhanced patient safety, and increased mental and behavioral health recommendations.
Efficiency
The outreach score presents pre-validated patient data in one document, which improves CM workflow efficiency by eliminating the need to consult multiple sources for information. This has been especially critical during the COVID-19 pandemic when healthcare utilization radically decreased and the health information exchange was one of the main sources of self-assignment.
Interventions and referrals
CMs receive patient lists organized in descending order of outreach score. They then call patients to offer clinical services and interventions they deem appropriate. For example, they offer disease management and education assistance and they teach patients how to access healthcare in various settings and explain appropriate use. When medication issues arise, including adherence barriers, CMs make case referrals to the ACO pharmacist. To address healthcare inequalities (lack of or limited access to care, availability of services based on income, underinsured, limited healthcare knowledge, language barriers, literacy), CMs refer patients to wrap-around services such as social work, behavioral/mental health, and community programs as appropriate. To ensure interventions align with the overall care plan, CMs communicate patient-centered assessments to primary care providers. As needed, care plan adjustments are updated in the electronic health record.
Patient safety
During the pandemic, our ACO has emphasized patient education for the appropriate site and the importance of proper medication administration. The outreach score has helped reduce patient exposure through telemedicine visits with primary care providers and avoid unnecessary ED visits resulting from improper medication administration side effects.
Mental and behavioral health referrals
The previous risk score method for determining patient outreach focused on patient utilization and comorbid conditions. Because mental and behavioral health issues typically aren’t highlighted as comorbid conditions, they fade into the background or are overlooked. Inclusion of county and heavier weighting for behavioral health (which is just as important as chronic disease status and historical healthcare utilization) has helped move these patients up the list so they don’t go unnoticed.
Before the pandemic, an article by the Association of American Medical Colleges reported that ED visits for mental health and substance use disorders increased more than 44% from 2006 to 2014. According to a study by Holland and colleagues, the mean ED visit rate per 100,000 visits through the first 7 months of the pandemic for mental health conditions shows an increased rate from the same week a year prior even though overall ED visits decreased. This may indicate increased prevalence of mental and behavioral health conditions.
Benefits for patients receiving appropriate long-term care (outside of the ED) for their mental and behavioral health reach beyond the patient’s immediate mental state. They can include maintaining employment, adhering to medication recommendations, and positively affecting personal relationships.

Get a fuller picture
Risk scores can help predict anticipated expenses, but they don’t provide a holistic view of a patient’s health. The outreach score—which offers a fuller picture of an individual’s health, living conditions, and healthcare use—helps CMs identify patients with the greatest need for outreach. This approach saves time, increases intervention efficiency and effectiveness, and enhances patient safety.
Avery M. Day is an ACO senior quality analyst at Trinity Health Mid-Atlantic in Newtown Square, Pennsylvania. Mark E. Lewis is regional director of data and analytics at Trinity Health Mid-Atlantic. Rhonda S. Meredith is director of care management at Delaware Care Collaboration in Wilmington. Allison M. Patzek is director of ambulatory care management – north region at Quality Health Alliance in Langhorne, Pennsylvania. Tanya M. Vogel is director of acute and ambulatory care integration at Mercy Accountable Care in Darby, Pennsylvania.
References:
American Psychiatric Association. Stigma, prejudice and discrimination against people with mental illness. August 2020.
Bresnick J. Using risk scores, stratification for population health management. Health IT Analytics. December 16, 2016.
Center for Medicare and Medicaid Services. Risk Score Calculation. November 28, 2018.
Figueroa JF, Phelan J, Orav EJ, Patel V, Jha AK. Association of mental health disorders with health care spending in the Medicare population. JAMA Netw Open. 2020;3(3): 1210. doi:10.1001/jamanetworkopen.2020.1210
Holland KM, Jones C, Vivolo-Kantor AM, et al. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COIVD-19 pandemic. JAMA Psychiatry. 2021;78(4):372-9. doi:10.1001/jamapsychiatry.2020.4402
Joynt KE, Figueroa JF, Beaulieu N, Wild RC, Orav EJ, Jha AK. Segmenting high-cost Medicare patients into potentially actionable cohorts. Healthc. 2017;5(1-2):62-7. doi:10.1016/j.hjdsi.2016.11.002
Kalter L. Treating mental illness in the ED. Associate for American Medical Colleges. September 3, 2019.
National Equity Atlas. Neighborhood poverty. 2019.
Prusinski S. Beyond risk scores. The Actuary. February/March 2017.
Social Security Administration. Medicare. 2022.
Thornton RLJ, Glover CM, Cené CW, Gilk DC, Henderson JA, Williams DR. Evaluating strategies for reducing health disparities by addressing the social determinants of health. Health Aff. 2016;35(8):1416-23. doi:10.1377/hlthaff.2015.1357
U.S. News & World Report. Data explorer. bit.ly/3KxqbbC
U.S. News World Report. Healthiest communities: How they were ranked. September 22, 2021. usnews.com/news/healthiest-communities/articles/methodology
Wang J, Geng L. Effects of socioeconomic status on physical and psychological health: Lifestyle as a mediator. Int J Environ Res Public Health. 2019;16(2):281. doi:10.3390/ijerph16020281
Whittal K, Caldwell A. Rising risk: Maximizing the odds for care management. Milliman. March 2018.


















1 Comment.
This is where PMH Clinical Nurse Specialists-especially those in Psych Consultation Liaison Nurse roles, were very effective, and are still needed. The CNS not only does direct care with patients and families; they teach and model for other RNs and multidisciplinary teams; design improved healthcare delivery systems. Develop innovations in care and treatment.