A collaborative, patient-centered approach that considers a variety of factors will be most effective.
Takeaways:
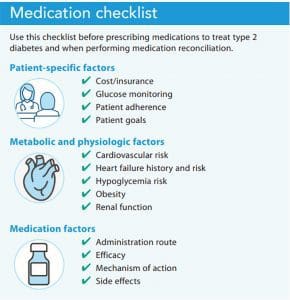
- Before selecting medications for type 2 diabetes and to promote optimal outcomes, three factors should be evaluated: patient-specific, metabolic/physiologic-specific, and medication-specific.
- Type 2 diabetes medication selection should be individualized with a focus on cardiovascular risk reduction and avoidance of hypoglycemia.
- Nurses are essential in educating patients about type 2 diabetes management, including medication options and medication-taking behavior.
Despite ongoing advancements in pharmacologic options to treat type 2 diabetes, recent data from Kazemian and colleagues suggest that only 64% of adults with the condition meet individualized glycated hemoglobin (HbA1c) treatment targets. To ensure better outcomes, patients and their care teams should work together, using a shared decision-making approach, to implement diet and physical activity interventions, followed by medication as needed.
Several resources can help nurses and providers assess medication options, including guidelines from the American Diabetes Association (ADA), the Endocrine Society, and the American Association of Clinical Endocrinologists for initiating and intensifying medications. Guidelines change frequently based on updated evidence and should be consulted in reference to individual patient situations and preferences. This article aggregates some of the most important patient, metabolic, physiologic, and medication factors that nurses and nurse practitioners should consider when implementing patient-centered medication selection for treating type 2 diabetes. (See Medication checklist.)
Patient factors
When counseling patients about medication options for treating type 2 diabetes, include individual goals, glucose monitoring, patient adherence, and cost and insurance.
Patient goals
ADA guidelines suggest that HbA1c levels should be targeted to <7% for most patients with diabetes (average blood glucose 154 mg/dL) and up to 8% for older patients, those with a limited life expectancy, and those who have other comorbidities or social influencers of health that impact outcomes (such as those who are undergoing chemotherapy or those who are under- or uninsured). More stringent HbA1c goals (<6.5%) can be targeted for patients with a low risk of hypoglycemia or with a recent diagnosis of diabetes, but only if it can be achieved without hypoglycemia or excess treatment burden.
Share evidence-based recommendations with patients and assess their interest and motivation in achieving these glucose levels. Use motivational interviewing to encourage patients to work toward achieving recommended targets, but note their personal goals and any real or perceived barriers. For example, a patient with low socioeconomic status may not be able to adjust their diet, ultimately impairing their ability to achieve glucose targets. Similarly, a patient with a history of frequent or severe hypoglycemia may be afraid to target lower glucose levels for fear of precipitating an episode. Acknowledge individual patient preferences and offer ongoing patient education and support. The ADA’s Standards of Medical Care in Diabetes, updated annually, promotes patient-centered, individualized outcomes.
Glucose monitoring
Some diabetes medications require patients to monitor their blood glucose frequently. For example, patients who are prescribed basal-bolus insulin typically inject the medication four times per day or more and should monitor their glucose levels before each injection. If a patient can’t or won’t perform this monitoring, safety is a consideration. Help patients explore continuous glucose monitors as an alternative to self-monitoring.
Patient adherence
Evaluate patient adherence to current medications before initiating any new medication. Kirkman and colleagues estimated that over 30% of patients with diabetes don’t take their medications as prescribed, and other studies have shown that anywhere from 38% to 93% of patients don’t adhere to medication regimens. You can establish rapport and trust with patients by taking time to explore barriers and opportunities for improvement. Optimizing the current medication regimen is an excellent first step to achieving glucose control.
Cost and insurance
Cost is a primary barrier to medication nonadherence. Diabetes medication costs are rising in the United States as a result of issues such as lack of pricing transparency, insurance negotiations, and medication patent rights. When possible, work with the care team, including pharmacists, to ensure that the medications selected are preferred and covered by the patient’s insurance. Several pharmaceutical companies offer programs to assist patients who are under- or uninsured.
Metabolic and physiologic factors
When determining which medication to implement, consider metabolic and physiologic factors, such as obesity, renal function, cardiovascular risk, hypoglycemia risk, and heart failure history and risk.
Obesity
Several classes of medications for treating type 2 diabetes—including biguanides (metformin), glucagon-like peptide-1 receptor agonists (GLP-1RA), sodium glucose cotransporter-2 (SGLT-2) inhibitors, and the lesser-known alpha-glucosidase inhibitors—can lead to weight loss. Metformin, for example, may contribute to up to a 3 kg weight loss, and semaglutide may result in up to a 6.1 kg weight loss. When possible, select medications with a favorable weight profile for patients who are overweight to avoid precipitating further weight increases. The Food and Drug Administration approved liraglutide (a GLP-1RA) specifically for weight loss, and it’s used as an antihyperglycemic agent at lower doses.
Dipeptidyl peptidase-4 (DPP-IV) inhibitors are weight neutral. Sulfonylureas, thiazolidinediones, and insulin can lead to weight gain or difficulty losing weight. When these medications are required, attempts at weight loss or weight neutrality should focus on diet and physical activity.
Renal function
Chronic kidney disease (CKD) is common in patients with diabetes. Several diabetes medications require dose adjustments for renal insufficiency and may be contraindicated for low glomerular filtration rates (GFRs). Medication classes that require dose-adjustment for renal insufficiency include biguanides, SGLT-2 inhibitors, and select DPP-IV inhibitors and GLP-1RAs. However, not all medications in each class need to be dose-adjusted. For example, the only DPP-IV inhibitor that doesn’t require renal dose adjustment is linagliptin. The GLP-1RA exenatide should be discontinued if the GFR is <30 mL/min, and other GLP-1RAs (such as semaglutide) don’t require any renal dose adjustments. Keep in mind that CKD can lead to a longer medication half-life, precipitating hypoglycemia when patients are taking sulfonylureas or insulin.
Recent data have suggested that SGLT-2 inhibitors may slow renal function decline through renal oxygenation and lowered inflammation in patients with CKD. The ADA recommends SGLT-2 inhibitors for patients with chronic kidney disease. Clinical research related to SGLT-2 inhibitors and preservation of renal function is ongoing.
Cardiovascular risk
All patients with diabetes have a heightened risk for cardiovascular disease. Several medications in the GLP-1RA and SGLT-2 class have demonstrated cardiovascular risk reduction and should be selected, when possible, for appropriate patients. The GLP-1RAs available in the United States that have demonstrated cardiovascular benefit include liraglutide, semaglutide, and dulaglutide. The SGLT-2 inhibitors with demonstrated cardiovascular benefit include empagliflozin, canagliflozin, and dapagliflozin. In contrast, some sulfonylureas and insulin are associated with an increased risk of cardiovascular disease, but a causal relationship hasn’t been determined.
Hypoglycemia risk
For patients at higher risk of hypoglycemia (patients who are older, who have CKD, who take sulfonylureas and insulin, who participate in heavy exercise, or who have an erratic diet), carefully select medication to avoid hypoglycemia. SGLT-2 inhibitors, GLP-1RAs, metformin, and DPP-IV inhibitors are excellent options when seeking to avoid hypoglycemia. However, hypoglycemia may still occur in patients taking these medications when combined with sulfonylureas or insulin.
Heart failure
Studies of SGLT-2 inhibitors consistently demonstrate that patients who take them have a reduced risk of hospitalization for heart failure. This benefit is likely due to the diuretic effect of SGLT-2s. The most recent ADA guidelines suggest choosing this medication class for patients with diabetes and current heart failure or who are at high risk for heart failure.
Medication factors
When implementing a new therapy for type 2 diabetes, consider the medication’s mechanism of action, efficacy, side effects, and administration route.
Mechanism of action
Ensuring the most appropriate diabetes medication requires understanding how different classes of diabetes medications achieve glucose lowering. For example, GLP-1RAs specifically target post-prandial glucose by increasing insulin secretion related to food intake. If fasting blood glucose lowering is needed, these medications aren’t the best choice. In contrast, basal insulin will lower glucose throughout the day, particularly overnight and fasting glucose, but it doesn’t address post-meal hyperglycemia. Sulfonylureas will increase endogenous insulin secretion all day, irrespective of food intake, and will lead to hypoglycemia if patients don’t eat regular meals. Asking patients to increase glucose monitoring (or placing a diagnostic continuous glucose monitor) can help determine hyperglycemia patterns and which medications (in addition to diet and lifestyle changes) will target glucose elevations effectively.
Efficacy
Diabetes medications have different levels of efficacy (glucose-lowering potential). Before selecting an agent, compare the patient’s current HbA1c level with the goal. A recent systematic review and meta-analysis by Tsapas and colleagues suggested that the most effective diabetes medication for drug-naïve patients with type 2 diabetes is subcutaneous semaglutide (lowers HbA1c by 1.48%) and the lowest efficacy is DPP-IV inhibitors (0.60% decrease). The same study showed that HbA1c lowering for patients receiving metformin therapy was the highest for subcutaneous semaglutide (1.33% decrease) and the lowest for lixisenatide (0.43% decrease). Teach patients about the effectiveness of the different medication classes and discuss expected HbA1c lowering by drug class or individual medication.
Administration route
Most medications for type 2 diabetes are available in oral form. GLP-1RAs and insulin are the two medication classes that require injection. The newer GLP-1RAs are available as a once-weekly injection, which reduces patient burden. Semaglutide is available in oral form, making it an effective alternative for patients who prefer not to perform injections but would benefit from a GLP-1RA. Inhaled insulin, first approved in 2006, also is available, but acceptance by prescribers has historically been poor because of concerns about the long-term impact on pulmonary function. You can help educate patients about medication injections and explore their willingness and competency to perform a self-injection.
Side effects
Consider potential side effects when selecting a medication class and discuss them with patients. For example, if a patient has a pre-existing diagnosis of chronic urinary tract infections (UTIs), an SGLT-2 inhibitor may not be the best option as this class can lead to an increase in UTIs. If a patient has uncontrolled GI conditions, such as irritable or inflammatory bowel syndromes, a GLP-1RA or metformin would not be ideal because they can cause GI side effects such as diarrhea, constipation, and bloating and may exacerbate underlying symptoms.
Individualized care
A one-size-fits-all medical management approach for type 2 diabetes doesn’t exist. Nurses, in collaboration with the rest of the patient’s care team, should consider individual factors when selecting medications. When possible, encourage patient choice and input and choose medications proven to reduce cardiovascular risk. Clinical trials have suggested that when shared decision making is applied to clinic visits, patients increase their knowledge, experience improved communication with healthcare providers, have more realistic expectations about treatment outcomes, and feel a sense of increased autonomy.
Kathryn Evans Kreider is an associate clinical professor at Duke University School of Nursing in Durham, North Carolina.
References
American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes—2021. Diabetes Care. 2021;44(suppl 1):S111-24. doi: 10.2337/dc21-S009
Azoulay L, Suissa S. Sulfonylureas and the risks of cardiovascular events and death: A methodological meta-regression analysis of the observational studies. Diabetes Care. 2017;40(5):706-14. doi: 10.2337/dc16-1943
Dekkers CCJ, Gansevoort RT, Heerspink HJL. New diabetes therapies and diabetic kidney disease progression: The role of SGLT-2 inhibitors. Curr Diab Rep. 2018;18(5):27. doi:10.1007/s11892-018-0992-6
Herman ME, O’Keefe JH, Bell DSH, Schwartz SS. Insulin therapy increases cardiovascular risk in type 2 diabetes. Prog Cardiovasc Dis. 2017;60(3):422-34. doi: 10.1016/j.pcad.2017.09.001
Johnson‐Rabbett B, Seaquist ER. Hypoglycemia in diabetes: The dark side of diabetes treatment. A patient‐centered review. J Diabetes. 2019;11(9):711-8. doi: 10.1111/1753-0407.12933
Kazemian P, Shebl FM, McCann N, Walensky RP, Wexler DJ. Evaluation of the cascade of diabetes care in the United States, 2005-2016. JAMA Intern Med. 2019;179(10):1376-85. doi: 10.1001/jamainternmed.2019.2396
Kirkman MS, Rowan-Martin MT, Levin R, et al. Determinants of adherence to diabetes medications: Findings from a large pharmacy claims database. Diabetes Care. 2015;38(4):604-9. doi: 10.2337/dc14-2098
Madsbad S, Holst JJ. Glycaemic control and weight loss with semaglutide in type 2 diabetes. Lancet Diabetes Endocrinol. 2017;5(5):315-7. doi: 10.1016/S2213-8587(17)30094-3
McEwen LN, Casagrande SS, Kuo S, Herman WH. Why are diabetes medications so expensive and what can be done to control their cost? Curr Diab Rep. 2017;17(9):71. doi: 10.1007/s11892-017-0893-0
Stahnke AM, Isaacs D, Capoccia KL, Cox M, Johnson T, Shealy KM. Comprehensive diabetes medication resource. ADCES in Practice. 2020;8(2):27-34. doi: 10.1177/2633559X20896414
Schwartz DD, Stewart SD, Aikens JE, Bussell JK, Osborn CY, Safford MM. Seeing the person, not the illness: Promoting diabetes medication adherence through patient-centered collaboration. Clin Diabetes. 2017;35(1):35-42. doi: 10.2337/cd16-0007
Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: A systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278-86. doi: 10.7326/M20-0864