
For more than 40 years, nurses have had the highest jobrelated injury rates of all healthcare personnel. In a 2011 survey conducted by the American Nurses Association:
• 62% of nurses expressed concerns about experiencing a disabling musculoskeletal injury
• 56% reported musculoskeletal pain caused or exacerbated by their work
• 42% reported being injured at work at least once during a 12- month period
• 52% reported chronic back pain
• 38% said they’d had to take time off work due to occupation-related back pain
• 20% said they’d changed their unit, position, or employment setting due to lower back pain.
The costly and seemingly intractable problem of work-related injuries among nurses and other healthcare professionals prompted Sage Products to convene a June 2015 meeting with leading experts in safe patient handling and mobility (SPHM) to better define the problem, clarify risk factors, and identify risk-reduction strategies. Panel members reached a consensus that the term patient handling injury (PHI) is an accurate, well-recognized term for identifying nurses’ injuries stemming from direct patient care. This term promotes awareness and knowledge about specific causes of injuries, establishes a shared understanding of the problem’s magnitude, and helps identify solutions to enhance nurse and patient safety.
The overarching goal of SPHM programs is to support nurses’ efforts to provide the right care for the right patient at the right time. Nurses must be aware of PHI risk factors and participate fully in efforts to ensure their patients’ and their own safety through consistent use of SPHM practices. This article examines leading risk factors for PHIs and reviews strategies for designing and implementing effective SPHM programs at healthcare facilities.
Risk factors
The following factors contribute to PHIs in nurses:
• prolonged work hours
• longer shift duration
• longer duration of exposure during a shift
• more consecutive days worked
• preexisting health conditions
• excessive sleepiness
• social and familial disruptions
• psychological disorders
• an older nurse workforce
• greater use of complex technological innovations
• increasing numbers of critically ill patients.
Certain organizational factors also contribute to high PHI rates—inadequate staff education in SPHM, failure to commit resources to technology to support safety, and limitations of systems that promote and reinforce SPHM.
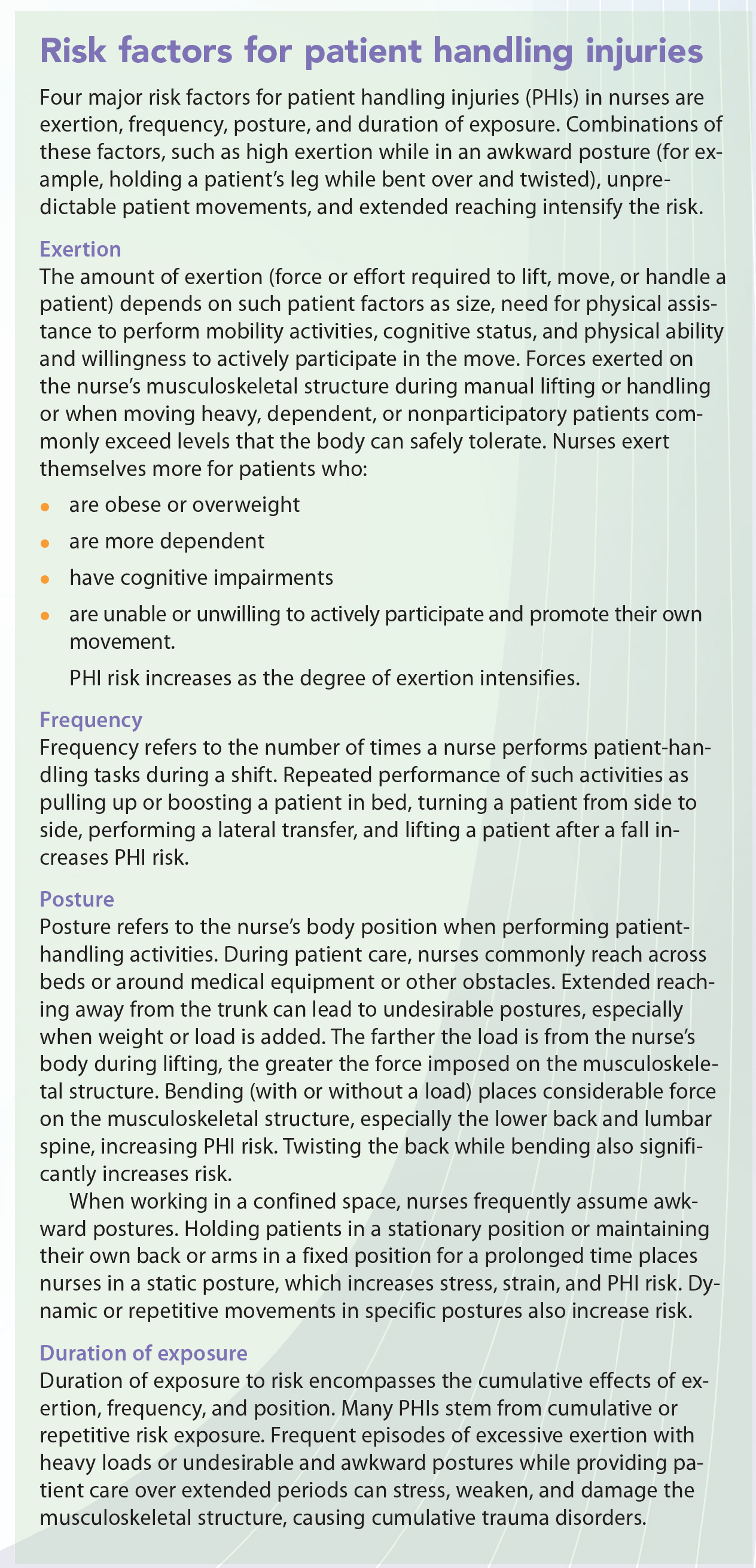
Based on a literature review and professional experience, Sage’s expert panel identified four major risk factors linked specifically to patient handling that increase nurses’ PHI risk. (See Risk factors for patient handling injuries.)
Multifaceted approach to injury prevention
Multifaceted SPHM programs are more effective than any single intervention in reducing or preventing PHIs; research shows such programs reduce PHI risk. A comprehensive effort to achieve sustained PHI reductions and improve patient safety hinges on multimodal strategies that take into account available human and equipment resources, as well as how these resources interact with work systems in diverse healthcare settings (such as perioperative, long-term care, and critical care and other acute-care environments). Successful SPHM programs must encompass appropriate technology along with worker education, a culture of safety, commitment from the top down, and routine periodic program evaluation.
Technology
Technological advances and assistive devices aid the critically important work of promoting patient movement and mobility while reducing or eliminating PHI risk factors. Proper use of assistive devices to lift, move, reposition, and transport patients is the foundation of a successful SPHM program. Assistive devices include mobile mechanical patient lifts, ceiling-mounted lifts, friction-reducing devices, lateral transfer aids, in-bed turning and repositioning devices, and height-adjustable electric beds. Ideally, this equipment should be located at or near the bedside of all patients.
All staff involved in patient handling activities must embrace and endorse integration of tools and technology into the care delivery process. Where nurses have easy access to appropriate equipment, evidence-based SPHM programs are crucial— but these alone are insufficient to guarantee program success (for instance, some nurses may choose not to use SPHM equipment). What’s more, SPHM programs may reduce injuries initially, but if nurses eventually revert to old, familiar patient-handling behaviors, injury reductions may not be sustained.
Also, assistive devices must match patients’ physical, cognitive, and clinical needs; nursing tasks to be performed; workplace design; and nurse characteristics. Furthermore, nurses must work within the structure of their organization to be effective agents of change for SPHM. An organizational investment in SPHM equipment and integration of this equipment into daily patient care is vital to a successful program.
Education
Competency-based employee education on use of SPHM devices and associated work practices is crucial. Both new hires and permanent staff involved in patient handling should receive education on an ongoing basis to promote, sustain, and increase their proficiency.
Culture
Successful design and implementation of SPHM programs requires meaningful, sustained changes in the workplace culture. Establishing a culture of safety at the individual, group, and organizational levels rests on understanding the complexity of healthcare delivery systems with tightly interwoven and constantly changing work processes. The organization’s current culture and SPHM program design must be evaluated from a systems perspective to ensure that the program has a sustained favorable impact on PHI rates.
In an organizational culture of safety:
• nurses feel a sense of responsibility and are willing to report adverse events, injuries, and near misses
• administrators respond to these reports consistently and effectively
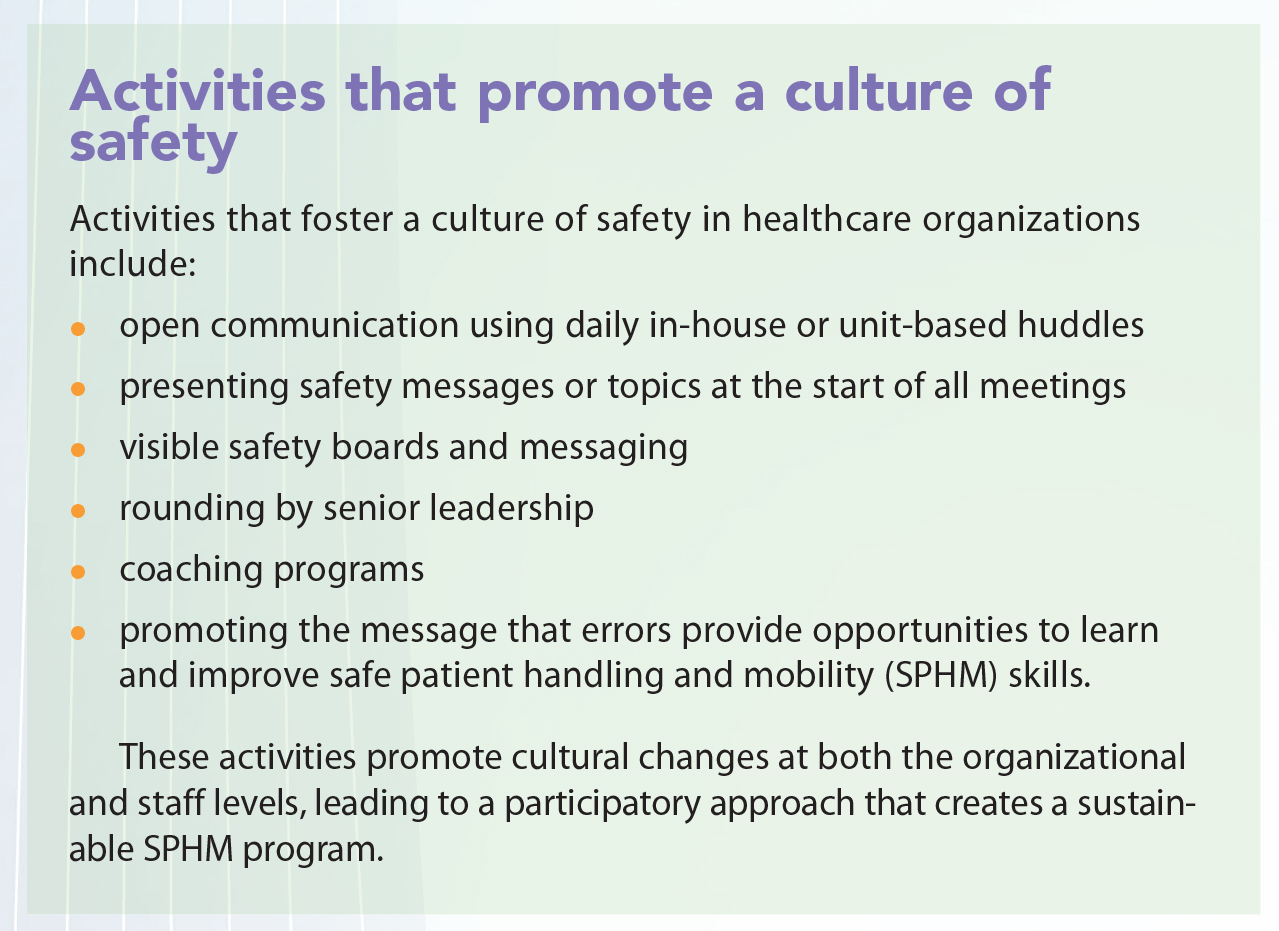
• everyone involved is treated fairly, with the cause of the event viewed from a systems perspective rather than assigning blame to individuals. (See Activities that promote a culture of safety.)
Commitment
To build and sustain a successful SPHM program, leaders, managers, and clinical staff must demonstrate a consistent commitment and nurse and patient safety must be integrated into clinical and business goals. Frontline nursing staff must be actively engaged and participate in planning, implementing, and evaluating the program. Visible active support of all program elements by senior leaders, mid – level managers, and engineering and construction staff can overcome barriers and promote changes in ways that frontline staff may be unable to achieve. Also, a well-designed and supported SPHM mentoring or coaching program at the unit or department level continuously reinforces SPHM principles and use of appropriate equipment, which are crucial to maintaining cultural changes.
Evaluation
SPHM program outcomes and processes must be evaluated objectively on a routine basis. Relevant outcome measures include decreased PHI rates, improved patient safety, reduced direct costs (including medical costs for injury treatment and rehabilitation, as well as compensation to injured workers), fewer days of lost work, increased employee satisfaction, and ongoing identification of opportunities for refining SPHM processes and policies. Outcome metrics at the system and unit levels can be disseminated through the facility’s intranet or “dashboards” that display safety data in real time. Employees should be encouraged to share stories of safety events with full transparency.
Thoughts, words, and actions
An industry-wide effort to prevent PHIs through SPHM programs requires partnerships and coalitions, staff education, increased access to and use of assistive devices, and ongoing education—all supported by federal and state SPHM initiatives in development. Numerous resources are available to assist organizations on their journey to SPHM.
Organizational change to support and promote SPHM occurs only when all organization members focus on three key questions: What are we are doing? Why are we doing it? What’s my role? Full engagement and cultural transformation can occur only when everyone responds effectively to these questions in thoughts, words, and actions.
Guy Fragala is a senior advisor for ergonomics at the Patient Safety Center of Inquiry in Tampa, Florida. Teresa Boynton, an occupational therapist, previously served as an ergonomics and injury prevention specialist and workers’ compensation consultant at Banner Health, Western Region, in Greeley, Colorado. Marlyn T. Conti is a patient safety initiatives manager at Intermountain Healthcare in Salt Lake City, Utah. Lee Cyr is director of insurance services with Synernet, Inc. in Portland, Maine. Lynda Enos is a certified professional ergonomist and ergonomics/human factors consultant with HumanFit, LLC, in Portland, Oregon. Devon Kelly is an injury prevention project manager in the safety department at OSF Saint Francis Medical Center in Peoria, Illinois. Nancy Mc- Gann is system manager of ergonomics and safe patient handling for SCL Health in Colorado, Kansas, and Montana. Kathleen Mullen is the safe patient handling coordinator for CoxHealth in Springfield, Missouri. Susan Salsbury is system lead for safe patient handling and mobility at OhioHealth and Associate Health and Wellness in Columbus, Ohio. Kathleen Vollman is a clinical nurse specialist/consultant for Advancing Nursing, LLC, in Northville, Michigan.
References
American Nurses Association. 2011 ANA Health & Safety Survey: Hazards of the RN Work Environment. 2011. goo.gl/b5sBd5
American Nurses Association. Handle with Care Fact Sheet. goo.gl/6gh30b
American Nurses Association. Safe Patient Handling and Mobility: Interprofessional National Standards. Silver Spring, MD. American Nurses Association; 2013.
Bassett RD, Vollman KM, Brandwene L, Murray T. Integrating a multidisciplinary mobility programme into intensive care practice (IMMPTP): a multicentre collaborative. Intensive Crit Care Nurs. 2012;28(2):88-97.
Gallagher S. Implementation Guide to the Safe Patient Handling and Mobility Interprofessional National Standards. American Nurses Association. Silver Spring, MD; 2013.
Joint Commission, The. Improving Patient and Worker Safety: Opportunities for Synergy, Collaboration and Innovation. November 2012. goo.gl/ZnzqTd
Mayeda-Letourneau J. Safe patient handling and movement: a literature review. Rehabil Nurs. 2014;39(3):123-9.
Mohammed S, Singh D, Johnson GT, et al. Evaluation of occupational risk factors for healthcare workers through analysis of the Florida Workers’ Compensation Claims Database. Occup Dis Environ Med. 2014;2(4):77-85.
Nelson AL, Motacki K, Menzel N. The Illustrated Guide to Safe Patient Handling and Movement. New York, NY: Springer Publishing Company, LLC; 2009.
Occupational Safety & Health Administration. Worker Safety in Hospitals. Caring for our Caregivers. osha.gov/dsg/hospitals/program_development.html
Powell-Cope G, Toyinbo P, Patel N, et al. Effects of a national safe patient handling program on nursing injury incidence rates. J Nurs Adm. 2014;44(10):525-34.
Schoenfisch AL, Lipscomb HJ, Pompeii LA, et al. Musculoskeletal injuries among hospital patient care staff before and after implementation of patient lift and transfer equipment. Scand J Work Environ Health. 2013;39(1):27-36.
Trinkoff AM, Geiger-Brown JM, Caruso CC, et al. Personal safety for nurses. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality; 2008; 2-473-2-508.


















{kind=link}
{kind=link}
1 Comment.
Dear Editor,
I am writing in response to the article “Patient handling injuries: Risk factors and risk-reduction strategies” by Fragala, G., Boynton, T., Conti, M.T., Cyr, L., Enos, L., Kelly, D., McGann, N., Mullen, K., Salsbury, S., & Vollman, K. published in Volume 11 No. 5 issue of the May 2016 edition of American Nurse Today. This was an interesting article in regards to the need for safe patient handling and mobility (SPHM) programs to be implemented in healthcare facilities in order to decrease patient handling injury (PHI) rates, lost work days, and direct costs. However, there was no evidence provided to show how beneficial the programs are for the healthcare facilities. I am writing in to provide some statistical data that supports the authors’ position within this article. This information is imperative for the reader to have in order to encourage such a necessary change in the healthcare industry.
After further research I came across an OSHA document that provided the necessary statistical data. Within this document “Safe patient handling programs: Effectiveness and cost savings” located at https://www.osha.gov/dsg/hospitals/documents/3.5_SPH_effectiveness_508.pdf
there were several studies done across the United States after introducing SPHM programs, all of which experienced positive outcomes. The following includes just some of the results the document mentioned:
• Franklin Square Hospital in Maryland experienced 70% reduction in PHI after 3 years
• Englewood Hospital in New Jersey experienced 57.1% reduction in PHI and 80.5% reduction in lost work days after 2 years
• University of Iowa Hospitals and Clinics experienced 85% reduction in workers’ compensation and 76% reduction in lost work days after 3 years
• Sacred Heart Medical Center in Oregon saved $305,000 in direct costs over 2 years
• Stanford University Medical Center saved $2.2 million in direct costs after 5 years
In conclusion, this statistical data provides the evidence needed to show how beneficial SPHM programs are to healthcare facilities. Based on the results from this study there was up to a 70% reduction in PHI rates, up to an 80.5% reduction in lost work days, and as much as $2.2 million saved in direct costs. In addition, these reductions all occurred in a time frame of 5 years or less. In the healthcare industry hands on patient care is necessary, therefore it is essential that healthcare facilities implement an SPHM program.
Sincerely,
Toni Erway, RN