
Improve outcomes with supportive care.
- Chemotherapy-induced nausea and vomiting (CINV) is a common side effect of pediatric cancer treatment.
- Chronic nausea and vomiting can result in electrolyte imbalances and malnutrition.
- Supportive care as part of the chemotherapy protocol helps prevent some of the anticipated complications before therapy starts.
Anabelle*, a 6-year-old girl, has a history of medulloblastoma with leptomeningeal disease. After a total resection of the primary tumor, she experienced hydrocephalus, which required a shunt placement. Anabelle has completed 30 cycles of radiation therapy (RT) via protons.
Four weeks after RT, Anabelle arrives at the pediatric oncology unit for her first cycle of chemotherapy, which consists of cisplatin, high-dose cyclophosphamide, and vincristine administered via a central venous catheter. The chemotherapy protocol includes ondansetron to prevent nausea and vomiting. At treatment onset, Anabelle develops continuous nausea and begins ondansetron every 8 hours, which the provider later advances to daily granisetron. The provider also prescribes aprepitant and dexamethasone for the first 3 days of treatment. Anabelle’s weight on admission for chemotherapy shows a loss of 2 kg since the end of RT, so the provider prescribes enteral feeding.
Throughout the course of chemotherapy, the patient’s vital signs remain stable, and her complete blood count and differential are normal except for neutropenia with an absolute neutrophil count of zero. Metabolic abnormalities include potassium 3.2 mEq/L (normal: 3.4–4.7 mEq/L), phosphorus 4.0 mg/dL (normal: 4.1–5.9 mg/dL), and magnesium 1.7 mg/dL (normal: 2–2.8 mg/dL). The provider orders I.V. lorazepam every 6 hours as needed for intractable nausea and vomiting. The nurse notes that Anabelle guards her abdomen, which is soft, flat, and nontender in all four quadrants.
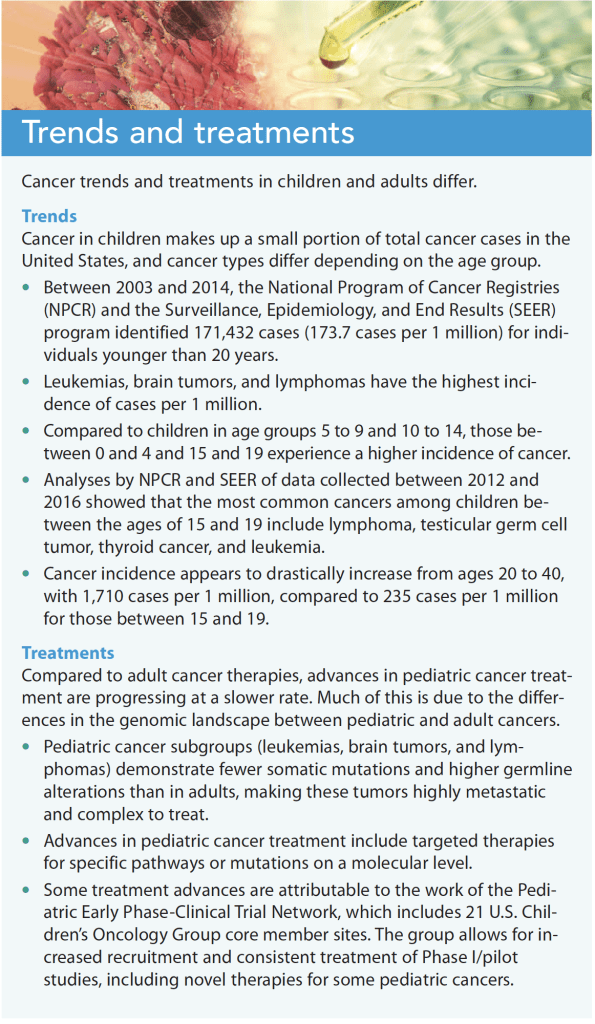
Chemotherapy prevents cancer cells from dividing and forces them into apoptosis. However, it doesn’t differentiate between normal cells and tumor cells, which can result in several common side effects, including those that disrupt systems involving rapidly dividing cells, such as the skin and mucus membrane (alopecia, mucositis, stomatitis), the GI tract (nausea, vomiting, diarrhea), and bone marrow suppression (pancytopenia). Supportive care as part of the chemotherapy protocol helps prevent some of these anticipated complications before therapy starts. (See Trends and treatments.)
Chemotherapy-induced nausea and vomiting (CINV) is a common side effect of pediatric cancer treatment. Understanding the pathophysiology, effects, and treatment options for CINV can help nurses identify and manage complications.
Pathophysiology
The vomiting center (VC) of the brain is located in the medulla oblongata. It integrates both a peripheral and central pathway to the brain, allowing multiple avenues for triggering a vomiting response. The peripheral pathway originates from the GI tract and contains multiple receptors along the duodenal and gastric tract, such as serotonin (5-HT3), neurokinin 1 (NK-1), and cholecystokinin-1. Once activated, the signal terminates at the nucleus tractus solitarius (NTS) to relay signaling to the VC. The central pathway allows the VC to receive direct signaling by cholinergic and histamine responses caused by pain, vestibular excitation (head movement), or strong emotions (anxiety, fear).
The central pathway also includes input from the chemoreceptor trigger zone (CTZ)—located on the fourth ventricle—in response to chemical stimuli such as chemotherapy and other medications. The CTZ doesn’t have a blood–brain barrier, so any drugs normally blocked by the central nervous system (CNS) can enter. In addition, 5-HT3 and NK-1 receptors located along the NTS, CTZ, and dorsal motor nucleus of the medulla oblongata can trigger a central response to the VC.
Nausea is less understood and can be described as a subjective feeling or sensation. No evidence exists to determine if the exact same neurotransmitters that target the VC also target nausea. However, dopaminergic, histaminergic, and muscarinic receptors may be involved since medications that control vomiting also work for nausea.
In addition to chemotherapy stimulation of the CTZ, several factors that contribute to Anabelle’s nausea and vomiting include recent proton RT and a significant history of anxiety and behavioral stress. The nurses and other clinicians performing physical assessments determine that her abdominal guarding is a sign of fear.
Chemotherapy can trigger receptors from the peripheral pathway or directly affect the VC by eliciting a response from the CTZ. About 24 hours after chemotherapy begins, free radicals produced by the treatment cause the enterochromaffin cells in the GI tract to release serotonin. Increased serotonin can elicit a response by the receptors to the VC to initiate emesis.
The peripheral pathway is associated with acute CINV. Chemotherapy also can stimulate the release of substance P (a neurotransmitter that activates NK-1 receptors) in the CNS. The central pathway is associated with delayed CINV.
Before Anabelle starts her first cycle of chemotherapy, the provider has already ordered ondansetron, aprepitant, and dexamethasone as part of the standard of care based on current evidence-based guidelines. Ondansetron and granisetron are 5-HT3 receptor antagonists and aprepitant is an NK-1 receptor antagonist. Aprepitant, dexamethasone, and ondansetron ease Anabelle’s nausea and vomiting during the first 3 days of treatment.
CINV effects
Serious CINV impacts a patient’s quality of life. Chronic nausea and vomiting can result in electrolyte imbalances and malnutrition.
Electrolyte imbalances
Common electrolyte imbalances include potassium, magnesium, and phosphorus loss. Providers typically order a daily basic metabolic panel with magnesium and phosphorus during treatment and for a few days post-treatment. Electrolytes usually are replenished via I.V. fluids, oral supplements, parenteral nutrition, or a combination. In severe cases, providers may order I.V. electrolytes.
Malnutrition
Malnutrition, the most common CINV complication, can lead to higher disease burden and prolonged hospital stay. Patients, especially children, lose their appetite with chemotherapy as a result of nausea or fear of vomiting. To increase nutrition, nurses should consult a registered dietician to formulate an individualized plan for maintaining the patients’ nutritional status. The most common first-line treatments to address appetite loss include prescribing an appetite stimulant such as cyproheptadine or administering enteral feeding.
For patients who can’t tolerate food, have difficulty eating, or are experiencing a severe loss of appetite, the provider may order a nasogastric (NG) tube. For children with severe CINV or those receiving highly emetogenic chemotherapies (such as high doses of cisplatin or cyclophosphamide) and can’t tolerate an NG tube, the provider may order a gastrostomy tube. The goal is to increase the patient’s total calorie intake and provide adequate nutrition. If enteral feedings aren’t well-tolerated, the provider may order total parenteral nutrition (TPN) until CINV is adequately controlled. In pediatric patients who can’t tolerate the full daily recommended caloric intake through enteral feeds, TPN can be given simultaneously to meet caloric goals and improve overall outcomes.
After 1 week of chemotherapy, Anabelle can’t tolerate NG feedings. She begins vomiting and loses another 2 kg in 1 month. The provider changes ondansetron to granisetron, a drug in the same class with a longer half-life and evidence of working better than ondansetron. Granisetron seems to help control Anabelle’s nausea, but she vomits after medications and feeds are given through the NG tube. Her lab reports show hypokalemia, hypomagnesemia, and hypophosphatemia. A surgical consult leads to the placement of a gastrostomy tube. The provider wants to control her nausea and vomiting before restarting enteral feedings.
Nursing implications
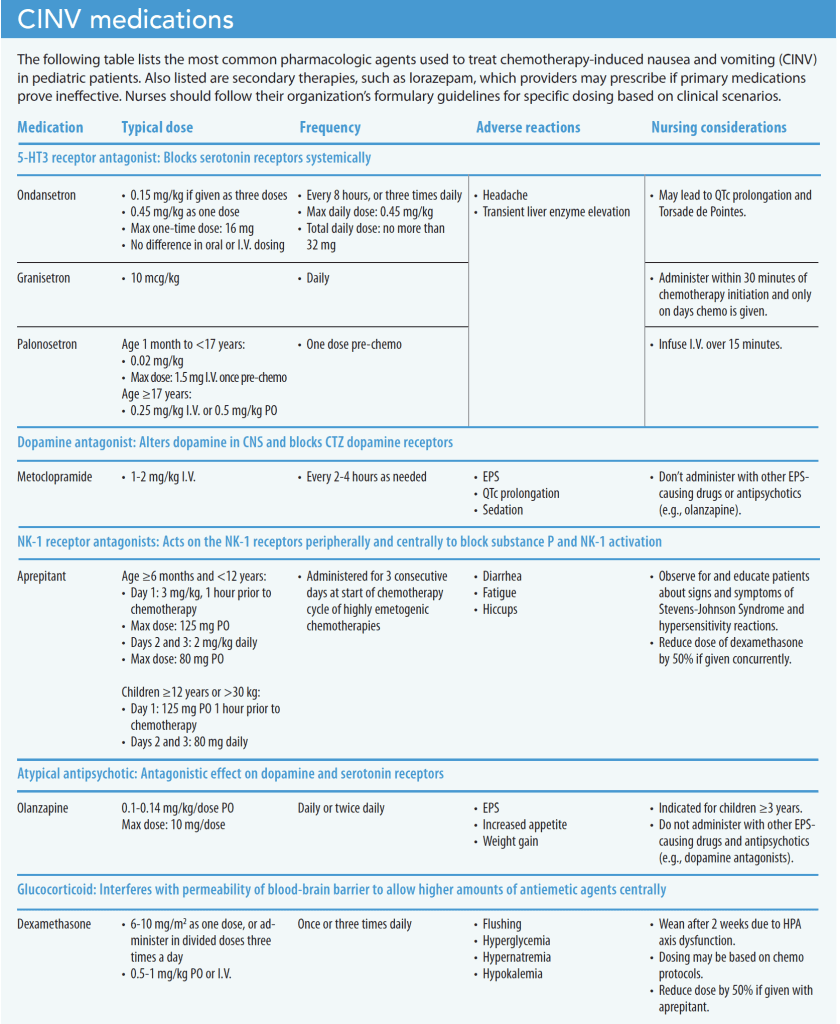
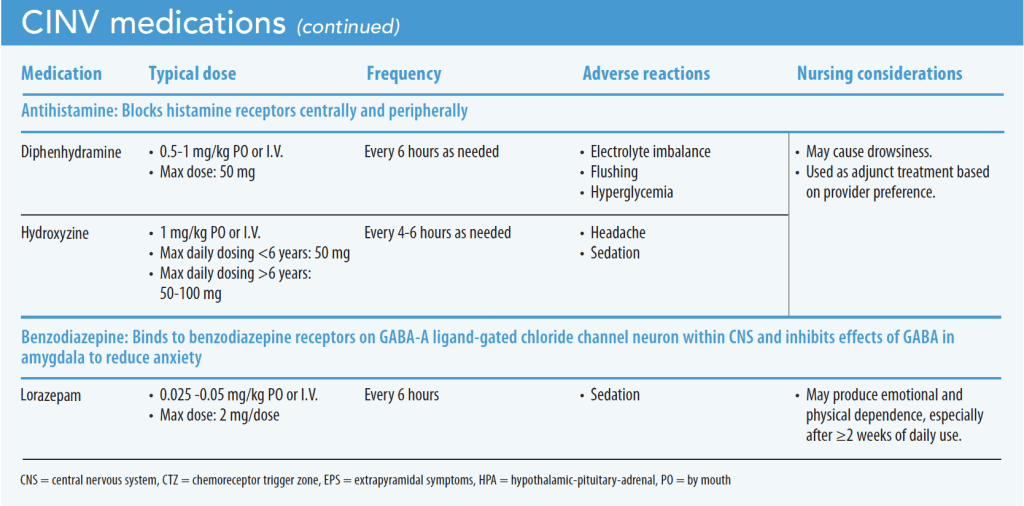
When nurses understand the risk of prescribed chemotherapies that cause nausea and vomiting, they can anticipate appropriate evidence-based pharmacologic and nonpharmacologic treatment. If evidence-based primary pharmacologic treatments aren’t effective, providers may prescribe secondary therapies (such as lorazepam) and other as-needed medications (such as hydroxyzine). (See CINV medications.)
Nonpharmacologic treatment
Before initiating secondary pharmacologic treatment, clinical practice guidelines endorsed by the Children’s Oncology Group suggest using nonpharmacologic modalities. The expertise of a child-life specialist (if available) and the participation of the child’s parent or guardian can aid CINV management. If a child-life specialist isn’t available, a behavioral therapist or psychologist can assess the patient for any behavioral components to vomiting. Building a rapport with the patient builds trust and may reduce anxiety, which can cause vomiting.
Dietary interventions to prevent CINV include reducing foods with strong smells and avoiding spicy, fatty, and salty foods. Taking antiemetics before meals also may help. If the patient has an NG tube or gastrostomy tube, nurses should push medications slowly to avoid a rush of fluids through the tube, which may trigger emesis. If the patient is actively vomiting, feedings should be held for an hour.
Other nonpharmacologic management techniques include acupuncture, acupressure, guided imagery, music therapy, progressive muscle relaxation, and psycho-educational support and information. After an episode of vomiting, judicious oral care can help maintain comfort and dental health.
Antiemetic adverse reactions and interactions
Antiemetics may produce adverse reactions and drug interactions. For example, metoclopramide and 5-HT3 antagonists can cause QTc prolongation. Olanzapine and metoclopramide can increase the risk of extrapyramidal side effects, including dystonia, akathisia, and Parkinsonism.
Olanzapine, an atypical antipsychotic drug indicated for schizophrenia, has shown a clinically significant increase in the numbers of patients who reported no vomiting or severe nausea that required rescue antiemetic therapy during and after chemotherapy. The stronger the 5-HT3 antagonist, the more time required between administrating doses. Nausea and vomiting that respond to lorazepam indicates that something else (such as anxiety) may be the cause.
Improve outcomes
Anabelle receives I.V. lorazepam 0.025 mg/kg every 6 hours as a standing order. The nurse realizes that Anabelle’s anxiety about medical interventions may play a factor in frequent emesis. Before performing any medical intervention, the nurse pages the certified child-life specialist to help Anabelle with her anxiety. To build rapport, the nurse encourages Anabelle to participate in care, allowing her to push her own medications and flushes via the gastrostomy tube. The provider changes Anabelle’s lorazepam to olanzapine 0.14 mg/kg via her gastrostomy tube. She stops vomiting, the nurse initiate feeds, and eventually Anabelle is weaned off TPN.
CINV negatively impacts patient quality of life. If left unmanaged, persistent vomiting can cause devastating complications that lead to severe malnutrition and electrolyte imbalances. Because CINV results from multiple factors, an interprofessional approach that includes pharmacologic and nonpharmacologic therapy, as well as consultation with dieticians and mental health professions, can improve outcomes, especially for pediatric patients.
Nick Deuz is a per diem staff nurse at Children’s Hospital at Montefiore and NewYork-Presbyterian Morgan Stanley Children’s Hospital, in New York City, and a certified pediatric nurse practitioner. Fidelindo Lim is a clinical associate professor at New York University Rory Meyers College of Nursing, in New York City.
References
Alhammad AM, Alkhudair N, Alzaidi R, Almosabhi LS, Aljawadi MH. Assessing the impact of chemotherapy-induced nausea and vomiting on patients’ quality of life: An Arabic version of the Functional Living Index–Emesis. J Oncol Pharm Pract. 2022;28(3):535-41. doi:10.1177/1078155221998447
Children’s Oncology Group. Phase 1 Consortium. https://childrensoncologygroup.org/index.php/66-phase-1-consortium/phase-1-consortium
Flank J, Robinson PD, Holdsworth M, et al. Guideline for the treatment of breakthrough and the prevention of refractory chemotherapy-induced nausea and vomiting in children with cancer. Pediatr Blood Cancer 2016;63(7):1144-51. doi:10.1002/pbc.25955
Flank J, Schechter T, Gibson P, et al. Olanzapine for prevention of chemotherapy-induced nausea and vomiting in children and adolescents: A multi-center, feasibility study. Support Care Cancer. 2018;26(2):549-55. doi:10.1007/s00520-017-3864-8
Friend AJ, Phillips B. Olanzapine was an effective additional antiemetic for children and young people undergoing highly emetogenic chemotherapy. Arch Dis Child Educ Pract Ed. 2021;107(4):312. doi:10.1136/edpract-2021-321775
Ghiasi N, Bhansali RK, Marwaha R. Lorazepam. StatPearls. February 7, 2022. ncbi.nlm.nih.gov/books/NBK532890
Griddine A, Bush JS. Ondansetron. StatPearls. September 29, 2021. ncbi.nlm.nih.gov/books/NBK499839/#:~:text=Standard%20oral%20dosing%20includes%208,prevent%20postoperative%20nausea%20and%20vomiting.
Gupta K, Walton R, Kataria SP. Chemotherapy-induced nausea and vomiting: Pathogenesis, recommendations, and new trends. Cancer Treat Res Commun. 2021;26:100278. doi:10.1016/j.ctarc.2020.100278
McDaniel L. Blood chemistry and body fluids. In: Kleinman K, McDaniel L, Molloy M, eds. The Harriet Lane Handbook. 22nd ed. Philadelphia, PA: Elsevier; 2020; 646-7.
McGrath KH, Evans V, Yap J. Indications and patterns of use for parenteral nutrition in pediatric oncology. J Parenter Enteral Nutr. 2020;44(4):632-8. doi:10.1002/jpen.1685
Miller KD, Fiddler-Benaoudia M, Keegan TH, Hipp HS, Jemal A, Siegel RL. Cancer statistics for adolescents and young adults, 2020. CA Cancer J Clin. 2020;70(6):443-59. doi:10.3322/caac.21637
O’Hanlon Curry J, Nixon C. Nausea and vomiting. In: Kline NE, ed. Essentials of Pediatric Hematology/Oncology Nursing. 4th ed. Chicago, IL: Association of Pediatric Hematology Oncology Nurses; 2014; 227-8.
Patel P, Robinson PD, Devine KA, et al. Prevention and treatment of anticipatory chemotherapy-induced nausea and vomiting in pediatric cancer patients and hematopoietic stem cell recipients: Clinical practice guideline update. Pediatr Blood Cancer. 2021;68(5):e28947. doi:10.1002/pbc.28947
Patel P, Robinson PD, Thackray J, et al. Guideline for the prevention of acute chemotherapy-induced nausea and vomiting in pediatric cancer patients: A focused update. Pediatr Blood Cancer. 2017;64(10):e26542. doi:10.1002/pbc.26542
Paw Cho Sing E, Robinson PD, Flank J, et al. Classification of the acute emetogenicity of chemotherapy in pediatric patients: A clinical practice guideline. Pediatr Blood Cancer 2019;66(5):e27646. doi:10.1002/pbc.27646
Sicari V, Zabbo CP. Diphenhydramine. StatPearls. July 11, 2022. ncbi.nlm.nih.gov/books/NBK526010
Siegel DA, Li J, Henley SJ, et al. Geographic variations in pediatric cancer incidence – United States, 2003-2014. Morb Mortal Wkly Rep. 2018;67(25):707-13. doi:10.15585/mmwr.mm6725a2
Sweet-Cordero EA, Biegel JA. The genomic landscape of pediatric cancers: Implications for diagnosis and treatment. Science. 2019;363(6432):1170-5. doi:10.1126/science.aaw3535
Thomas K, Saadabadi A. Olanzapine. StatPearls. May 2, 2022. ncbi.nlm.nih.gov/books/NBK532903
Key words: chemotherapy, pediatric cancer, nausea and vomiting

















