
A nurse’s guide to intervention
- Occasional premature ventricular complexes (PVCs) are commonly seen on cardiac monitoring and frequently increase with age.
- Each time a patient has a PVC, they’re experiencing a nonperfusing heartbeat, which may be detected as a skipped wave when assessing a pulse, or a wide ventricular early wave followed by a pause on a 6-second ECG strip.
- Considering factors such as frequency, symptoms, causes, R-on-T phenomenon, and the presence of heart disease can help you make decisions about care wherever you encounter the patient.
Learning Objectives
- Recognize key characteristics of premature ventricular complexes (PVCs) on cardiac monitoring.
- Apply critical thinking to assess and respond to patients experiencing PVCs.
- Demonstrate knowledge of contributing factors and medication considerations related to PVC management.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 6/1/28
You admit Sara Martin* to the medical-surgical floor from the emergency department with a diagnosis of heart failure exacerbation, hypertension, type 2 diabetes, peripheral vascular disease, chronic renal failure, and depression. Her initial vital signs are blood pressure 100/62 mmHg when lying down, heart rate 75 beats per minute and irregular, respiratory rate 22 breaths per minute, temperature 98.2° F (36.3° C), oxygen saturation 90% on 2 L of oxygen via nasal cannula, mean arterial pressure (MAP) 74 mmHg. Ms. Martin’s lab values include B-type natriuretic peptide 1,000 pg/mL, potassium 2.8 meq/dL, magnesium 1.2 mg/dL, blood urea nitrogen (BUN) 12 mg/dL, and creatinine 1.8 mg/dL.
Atrial fibrillation: Recognition and management to improve quality of life
Myocardial infarction: Nursing assessment and care
Ms. Martin says that she feels lightheaded and anxious. She also describes her heart as “fluttering” at times.
The patient has an order for telemetry monitoring. After placing leads and electrodes on her chest, you note a sinus rhythm with continuous bigeminy premature ventricular complexes (PVCs) on the monitor. You print a 6-second ECG strip to place in the patient’s chart. Should you intervene?
What are PVCs?
Occasional PVCs are commonly seen on cardiac monitoring and frequently increase with age. They result from increased irritability of ventricular cells, which leads the beat to arise from the bundle of His pathways rather than the atrioventricular node. PVCs, easily identified on a cardiac strip, appear as an early, wide (>0.12 second) ventricular complex followed by a pause in the cardiac rhythm.
PVCs can be unifocal (same shape) or multifocal (different shapes). This variance occurs due to the foci (origin) of the irregular beat. PVCs can come as one (occasional), two (couplet), or three or more (non-sustained ventricular tachycardia [VT]). The patient may have rhythmic PVCs at every other beat (bigeminy) or every third beat (trigeminy). PVCs also can be intermittent or sustained. A PVC can originate during, rather than after, a T wave in the cardiac cycle and can cause VT as a result of the R-on-T phenomenon. Note each of these characteristics when planning an intervention.
Each time a patient has a PVC, they’re experiencing a nonperfusing heartbeat, which may be detected as a skipped wave when assessing a pulse, or a wide ventricular early wave followed by a pause on a 6-second ECG strip. When examining a 6-second ECG strip, don’t count the PVC in calculating the heart rate. (See ECG strips.)
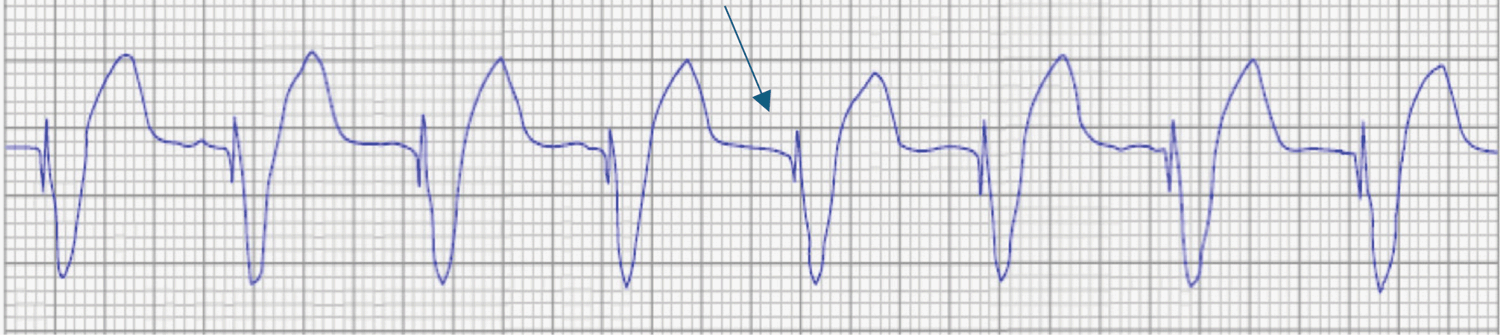
ECG strips
The following ECG strips illustrate various types of premature ventricular complexes (PVCs).
Occasional PVC

Bigeminy PVC

Non-sustained ventricular tachycardia
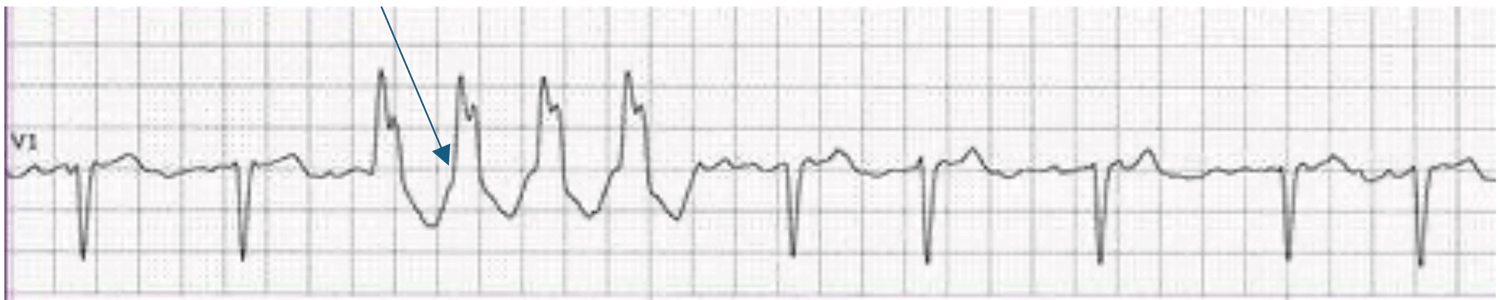
Ventricular paced beat with a spike (no PVC)
Patients sometimes feel these abnormal heartbeats as a skipped beat or palpitations, which they may describe as “fluttering.” The more frequently the patient has PVCs and the closer they come to each other, the more often their heart isn’t perfusing blood to the rest of the body.
According to Suba and colleagues, nurses frequently silence or change the alarms on cardiac monitoring systems designed to detect PVCs because of their common occurrence and alarm fatigue. In addition, ventricular paced beats in patients with a pacemaker can be mistaken for PVCs if the nurse doesn’t program the monitor to look for a pacing spike. The most sensitive PVC alarms should remain on for new patients until you know more about their history and heart rhythm.
What causes PVCs?
Exogenous causes of PVCs include caffeine, sleeplessness, anesthesia, stress, nicotine, medications, methamphetamine, and alcohol. Endogenous causes include infection, myocardial ischemia, myocardial infarction, chronic heart failure, anemia, hyperthyroidism, hypomagnesemia, hypokalemia, and hypercalcemia. Consider all causes when a patient experiences frequent PVCs. If no underlying heart disease exists, primary care providers (PCPs) don’t typically treat occasional PVCs; however, nurses should continue to closely monitor the patient. (See Medications and PVCs.)
Medications and PVCs
The following types of medications can lead to premature ventricular complexes (PVCs).
How do you know whether the PVCs on Ms. Martin’s second ECG strip require intervention? Consider that the patient has predisposing factors for PVCs, including heart failure, hypomagnesemia, and hypokalemia. The patient also reports symptoms, including “fluttering” and anxiety, and presents with hypoxemia and hypotension. Your course of action depends on a symptomatic vs asymptomatic presentation along with PVC frequency and the location of foci in the cardiac cycle. According to Mastenbjork and Meloni, frequent PVCs warrant different interventions than do asymptomatic or occasional PVCs.
Symptomatic vs. asymptomatic PVCs
Because PVCs are non-perfusing heartbeats, you would expect to see symptoms (dizziness, lightheadedness, anxiety, shortness of breath, palpitations, chest discomfort, dyspnea, and hypotension) related to a lack of perfusion in symptomatic patients. According to Suba and colleagues, what begins as a couplet or an intermittent run of bigeminy PVCs, for example, can become a run of nonsustained VT 3 or more consecutive PVCs. In a patient with frequent PVCs, immediately assess for changes in their status.
Begin by taking a complete set of vital signs along with level of consciousness (LOC) and compare them to the patient’s previous or baseline values. Look for hypotension, a decreased heart rate, and hypoxemia. Next, ask the patient how they’re feeling. Look for lightheadedness, dizziness, dyspnea, anxiety, and changes in LOC. If you note changes compared to baseline, inform the patient and their family of the arrhythmia, call the PCP, and stay with the patient.
According to the American Heart Association, if the patient has a sustained run of PVCs (VT), assess for a carotid or a femoral pulse (rather than a peripheral pulse due to shunting of blood to the patient’s core) and evaluate the patient’s LOC. If the patient has a pulse and is awake and alert, call the rapid response team (RRT) and attempt vagal maneuvers, which prompt the vagus nerve to act on the heart’s natural pacemaker and slow electrical impulses. These maneuvers include having the patient cough, bear down, or drink through a straw. In addition, the PCP can provide a carotid massage of one side of the patient’s neck. If vagal maneuvers convert the patient back to a normal sinus rhythm, work with the RRT or PCP to identify causes of the arrhythmia. Treatment might include a beta blocker, an antiarrhythmic, or a calcium channel blocker to decrease ventricular cell irritability.
If vagal maneuvers don’t convert the patient to normal sinus rhythm and the patient still has a pulse and remains awake and alert, consider recommending cardioversion to the PCP. Stable VT (with a pulse) will become unstable VT (no pulse) if allowed to continue. To convert fast or irregular rhythms, the PCP performs cardioversion with low-voltage joules using a defibrillator. Advocate for your patient to receive an I.V. sedative before cardioversion.
Asymptomatic PVCs
In a patient who experiences occasional PVCs that don’t originate from the T wave and reports no symptoms, consider whether the abnormal rhythm is sustained or intermittent. Manolis defines sustained abnormal rhythms as those that continue for 30 seconds or more; intermittent abnormal beats come and go. For example, for asymptomatic intermittent bigeminy, trigeminy, or PVC couplets, nursing interventions include assessment, continued monitoring, and consideration of the cause.
For a patient with asymptomatic runs of VT, obtain a set of vital signs to compare with baseline. According to Ignatavicius, if the vital signs are lower than the previous set (either a decrease of 20 mm/Hg systolic or 10 mm/Hg diastolic), the patient is deemed symptomatic, and you should call RRT and consider oxygen therapy.
In addition, assess for the presence of a carotid or a femoral pulse. If the patient has a pulse, then assess their LOC, take a set of vital signs to compare to pre-arrhythmia, attempt vagal maneuvers, consider oxygen therapy, and call the RRT. Someone should always stay with the patient as they can experience a rapid change in status. (See Nursing interventions.)
Nursing interventions
Nursing interventions depend on the type of premature ventricular complex (asymptomatic vs symptomatic) and frequency.
- Assess
- Continue to monitor
- Assess
- Continue to monitor
- Assess
- Continue to monitor
- Consider causes
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Consider causes
- Assess
- Continue to monitor
- Consider causes
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Consider causes
- Assess
- Continue to monitor
- Consider causes
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Consider causes
Without VT
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Consider causes/medications
With VT
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Follow VT guidelines
- Consider causes/medications
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- O2 therapy
- Consider causes/medications
- Assess
- Obtain vital signs and LOC
- Call RRT/PCP
- Pull crash cart near room
- O2 therapy
- Consider causes/medications
With Pulse
- Call RRT/PCP
- O2 therapy
- Try vagal maneuvers
- Consider asking the PCP for cardioversion
- Pull crash cart near room
- Stay with patient
- Consider causes/medications
Pulseless
- Call Code Blue
- Begin CPR
- Use closed-loop communication with healthcare team
- Send for code cart
- Begin Advanced Cardiac Life Support algorithm for pulseless VT
LOC = level of consciousness, PCP = primary care provider, RRT = rapid response team, VT = ventricle tachycardia
R-on-T phenomenon
When measuring ECG waves and intervals, determine whether the PVC originates within the T wave. According to Manolis, a PVC that originates during the relaxation period of the cardiac cycle (T wave) can result in increased ventricular irritability, which leads to VT. VT can occur if the patient experiences a prolonged QT interval ( >44 seconds) or if the electrical wave travels across damaged heart muscle to arrive at healthy heart muscle (ischemia). If you note this type of PVC and it doesn’t result in sustained VT, immediately assess the patient, look for causes, and call the PCP. If the R-on-T PVC does lead to VT, follow the protocol for VT with or without a pulse. If the R-on-T phenomenon accompanies no pulse, address it with the PCP after the patient is stable.
Other interventions
Anticipate interventions to address probable causes and prevent patient status deterioration. Ensure the patient has an I.V. for immediate medication administration. Evaluate the patient’s lab values and look for electrolyte imbalances, particularly potassium, magnesium, and calcium. If not already prescribed, recommend interventions to replace these electrolytes. (See Common I.V. push medications.)
Common I.V. push medications
Primary care providers frequently prescribe administration of the following medications
- Indicated for pulseless VT
- Assess for difficulty breathing
- Monitor BP frequently
- Administer IVP undiluted over 10 min
- Check BP and pulse before administering and periodically
- Administer IVP undiluted over 2 min
- Monitor ECG continuously
- Monitor BP and respiratory status frequently during administration
- Administer IVP as fast as possible for initial dose
- Check BP and pulse before administration and then periodically
- Administer IVP undiluted over 1 min
- Check BP and pulse before administration and then periodically
- Administer IVP undiluted at 0.5 mg/min (don’t exceed 1 mg/min)
- Check BP and pulse before administration and then periodically
- Administer IVP undiluted over 2 min
- Patients >65 years administer over 3 min
BP = blood pressure, IVP = I.V. push, VT = ventricular tachycardia
When taking vital signs, look for decreases in pulse rate, oxygen saturation, and blood pressure during arrhythmias. Recommend a 12-lead ECG to further evaluate and document PVCs. Review the patient’s history for diseases, medications, and substance use that could cause ventricular cell irritability. Anticipate recommending medications to inhibit ventricular arrhythmias such as lidocaine, metoprolol, and amiodarone.
In addition, review vagal maneuvers and how to teach the patient to perform them. Assess electrode and lead placement on the patient to evaluate heart rhythm correctly, and consider oxygen therapy.
Know when to intervene
Ms. Martin’s symptoms (lightheadedness, fluttering heart), lab results (high BNP, low magnesium and potassium), low blood pressure and oxygen saturation, and 6-second ECG strip (PVCs occurring after the T wave) indicate that she has sustained bigeminy PVCs with a diagnosis of heart failure exacerbation. She requires immediate intervention. You call the PCP and recommend treatments to reverse the low magnesium and potassium levels.
Although most occasional PVCs are benign, instances exist in which the patient has more frequent PVCs and you must intervene. Considering factors such as frequency, symptoms, causes, R-on-T phenomenon, and the presence of heart disease can help you make decisions about care wherever you encounter the patient. Knowing when to be concerned and intervene for a patient with PVCs can prove challenging, but with the correct knowledge, you can make the clinical judgment needed to ensure the best possible outcomes.
Christie Cavallo is an assistant professor in the division of nursing at Baptist Health Sciences University in Memphis, Tennessee.
American Nurse Journal. 2025; 20(6). Doi: 10.51256/ANJ062506
References
American Heart Association. Algorithms. cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/algorithms
Ignatavicius DD, Workman L, Rebar CR, Heimgartner NM. Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care. 10th ed. Philadelphia, PA: Elsevier; 2020.
Manolis MS. Premature ventricular complexes. Treatment and prognosis. UpToDate. December 4, 2024. uptodate.com/contents/premature-ventricular-complexes-treatment-and-prognosis
Mastenbjörk M, Meloni S. EKG/ECG Interpretation. 2nd ed. Las Vegas, NV: Medical Creations; 2021
Mladěnka P, Applová L, Patočka J, et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med Res Rev. 2018;38(4):1332-1403. doi:10.1002/med.21476
Suba S, Hoffmann TJ, Fleischmann KE, et al. Premature ventricular complexes during continuous electrocardiographic monitoring in the intensive care unit: Occurrence rates and associated patient characteristics. J Clin Nurs. 2023;32(13-14):3469-81. doi:10.1111/jocn.16408
Suba S, Hoffmann TJ, Fleischmann KE, et al. Evaluation of premature ventricular complexes during in-hospital ECG monitoring as a predictor of ventricular tachycardia in an intensive care unit cohort. Res Nurs Health. 2023;46(4):425-35. doi:10.1002/nur.22314
Key words: premature ventricular complexes, PVCs, ventricular tachycardia

















4 Comments. Leave new
Letter to the Editor:
In what was otherwise a good educational article explaining PVCs, I disagree with the author who stated that a vagal maneuver includes having a patient “drink through a straw”. The purpose of these maneuvers is to increase intrathoracic pressure which drinking would directly oppose (Niehues & Klovenski, 2023). Furthermore, in a setting where these maneuvers are taking place there is a high possibility the patient may require cardioversion or resuscitation and drinking fluids in an attempt to trigger a vagal response would potentially complicate intubation or sedating for cardioversion due to aspiration. I urge the author to reconsider her position in this educational piece, as I think the maneuver she describes could potentially be putting patients at risk.
With Regards,
XXXXX
Reference:
Niehues, L.J. & Klovenski, V. (2023) Vagal maneuver. StatPearls. Retrieved June 16, 2025, from https://www.ncbi.nlm.nih.gov/book
Thank you so much for your letter to the editor. I agree that drinking from a straw was not the appropriate wording. My article should have said “blowing through a pinched straw” to try a vagal maneuver if this fast VT with a pulse is SVT. ACLS (n.d.) recommends an alternative way to perform a Valsalva Maneuver other than having the patient bear down is to tell the patient to blow through a pinched straw or barrel of a 10 ml syringe for 15-20 seconds. I appreciate your effort to point this out.
ACLS (n.d) Vagal maneuvers with supraventricular tachycardia. https://acls.com/articles/vagal-maneuvers/#
Letter to the Editor:
Dear Editor,
On p. 8 of the June 2025 issue of American Nurse, Dr. Cavallo offers vagal maneuvers as treatment of sustained ventricular tachycardia (VT). Review of literature reveals this may be contraindicated in VT for several reasons. Vagal maneuvers affect the atrioventricular (AV) node to slow impulses by causing release of acetylcholine to stimulate M2 muscarinic receptor agonism, slowing Phase 0 of the action potential in the AV node. Elevated heart rate related to atrial impulses moving along re-entry pathways through the AV node are slowed by this cholinergic stimulus. Ventricular tachycardia originates from ectopic foci in the ventricles generating electrical impulses independently of the normal cardiac pacemaker circuit, which includes the sinus node and AV node, thus vagal maneuvers may have little effect. However in rare cases, vagal maneuvers applied during VT or sinus rhythm have caused sudden onset of ventricular fibrillation. Thus, most references recommend vagal maneuvers be used primarily for narrow-complex paroxysmal supraventricular tachycardia as a first line treatment to terminate the tachyarrhythmia by stopping the re-entry pathway. My thanks to Dr. Cavallo for an informative and interesting article.
Thank you for pointing this out, and I concur. My inclusion of that information was because nurses, as well as healthcare providers, often struggle with differentiating VT with a pulse at rates of 150 or above from SVT (Briggs, 2024). Also, Niehues and Klovenski (2023) states that Vagal maneuvers are often utilized first to abort episodes of stable supraventricular tachycardia (SVT) or differentiate SVT from ventricular tachycardias (VT). I agree with you and Briggs (2024) that we should assume it is ventricular tachycardia until proven otherwise, especially with a patient with cardiovascular disease. Trying vagal maneuvers with VT with a pulse used to be a part of the ACLS algorithm before 2016 due to the problem with differentiation.
Reference:
Briggs, B. (2024). A debate that need not happen: VT vs. SVT. Emergency Medicine News, 46(5), 1, 21. https://doi.org/10.1097/01.EEM.0000961402.31228.1e
Niehues, L.J. & Klovenski, V. (2023) Vagal maneuver. StatPearls. Retrieved June 16, 2025, from https://www.ncbi.nlm.nih.gov/book