
A new medical unit establishes an engaged nursing workforce.
Takeaways:
- A culture grounded in teamwork, shared governance, and accountability is needed for staff engagement and owning patient outcomes.
- To develop this culture, nurse leaders must establish a unit practice council (UPC).
- Engaging staff using the UPC model and creating a supportive practice environment can enhance nurse-sensitive outcomes and patient and staff experiences.
Establishing a new medical unit in a large academic hospital presents opportunities and challenges. At Emory University Hospital in Atlanta, an unbudgeted new unit, led by experienced nurse leaders (unit director, clinical nurse specialist [CNS], and clinical nurse/charge nurse), surmounted its first challenge (staffing) by starting primarily with contract staff. However, in just over a year, they filled all positions, eliminating the need for contract nurses. From the beginning, unit leaders acknowledged an opportunity to create a culture grounded in teamwork, shared governance, and accountability for patient outcomes. The challenge then became: How to effectively establish this culture within a diverse team?
Building a professional governance culture
The unit’s nurse leaders understood Tuckman’s stages of team formation—forming, storming, norming, and performing. (See 4 stages of team formation.) During this process, several themes emerged, including teamwork, professional (shared) governance, accountability, and ownership of patient outcomes. Porter-O’Grady’s description of empowered work environments, where those accountable for outcomes make decisions about the work, resonated with the leaders. Professional governance empowers nurses to own the outcomes of their practice and advocate for the resources necessary to improve patient care and the work environment.
4 stages of team formation
Tuckman identified four stages of team formation.
Stage 1—Forming: The team comes together and gets acquainted. Relationships are formal, and leaders within the group are emerging.
Stage 2—Storming: This stage is characterized by conflict, pushing boundaries, and competition as individual personalities become more apparent. Staff performance may decrease as a result of energy spent on nonproductive activities, leaving leaders discouraged.
Stage 3—Norming: Conflicts are resolved, and agreement is reached on common goals.
Stage 4—Performing: The team works together without friction to achieve its goals.
To develop this culture and engage nurses in making practice decisions and advocating for resources to improve the environment and care outcomes, the nurse leaders established a unit practice council (UPC).
Creating a UPC
The unit leaders identified nurses and nurse technicians on both shifts who displayed enthusiasm and creativity to serve on the UPC. The clinical nurse leader, a bedside nurse with experience leading clinical initiatives, serves as the UPC chair. The CNS is a non-voting member who serves as an internal clinical expert, connects the UPC to other resources within the organization or the healthcare system, presents outcome data, collaborates with the council members to establish priorities, and mentors them to identify the best decision-making evidence. The unit director is an ad hoc member the UPC can turn to for help finding resources and setting the scope of the UPC’s work.
During a kick-off meeting, council members established initial goals and priorities and created a purpose outlined in the UPC charter. The charter (based on a model charter available from a system-supplied toolkit) includes the council’s mission, vision, and values as well as its operating procedures, including officer elections and meeting frequency. The UPC then brainstormed key issues related to patient care and safety, including teamwork, communication between the nurses and nurse technicians, unit involvement in strategic quality initiatives, and improving the existing bedside shift report structure.
After finalizing the charter, shared goals, and strategic initiatives, council members created a clear communication structure using ISBAR (Identification, Situation, Background, Assessment, Recommendation). This format allows nurses to identify an issue, describe the situation that caused the issue, provide background information, assess the issue, and make recommendations for improvement.
The UPC chair then developed communication tools and protocols, including an ISBAR form, bulletin board, and monthly meetings and committee reports. In addition, UPC members developed a committees accountability spreadsheet.
ISBAR form
When nurses want to communicate with the UPC about an issue, they complete an ISBAR form, which the council uses to analyze the concern, create an action plan, measure the impact of the solution, and follow up with staff. (View ISBAR form). To ensure individual nurse anonymity, ISBAR forms are submitted via a locked UPC box.
Bulletin board
The UPC uses a bulletin board to communicate with the unit about council members and initiatives, new ideas, and current projects. A section of the bulletin board titled “Your Voice—We Listened!” shares action plan follow-up and decisions that impact patient care.
Monthly meetings and committee reports
At each monthly UPC meeting, an agenda guides the items for discussion, although members may raise other items of high importance. Nurses and nurse technicians who participate in quality initiatives and committees submit a monthly committee report to update the UPC and other team members about what’s happening across the organization. (View a monthly committee report form.)
Accountability spreadsheet
The committee accountability spreadsheet is used to ensure that council members and other initiative champions submit reports outlining progress toward identified goals. It also serves as a visual reminder for the staff to attend meetings, so information is brought back to the UPC for dissemination. (See Staying accountable.)
Staying accountable
The accountability spreadsheet serves as a visual aid on the unit to ensure that committee members and other initiative champions submit reports outlining progress toward identified goals. The assigned unit champions enter the check marks after they’ve attended the monthly meeting; champions also submit a report to the unit practice council (UPC). After verifying attendance and receipt of the report, the UPC chair changes the check mark to a blue dot. A red dot indicates the unit champion didn’t attend the meeting; in this case the CNS follows up with the champion.

EOC = environment of care, MET = medical emergency team, PLAN = professional lattice for advancement in nursing
UPC projects
Examples of current UPC projects include tools in patient rooms for nurses and nurse technicians to communicate with patients and each other, a standard bedside shift report process used by nurses and nurse technicians, and a buddy system for staff breaks. The UPC also monitors quality outcomes on the unit, such as catheter-associated urinary tract infection (CAUTI) and hospital-acquired pressure injury (HAPI) prevention.
Outcomes
Engaging staff using the UPC model and creating a supportive practice environment has resulted in nurse-sensitive outcome and patient and staff experience measures that outperformed the benchmarks for most of the preceding six quarters (four before the UPC was implemented and two after). During the new unit’s first year, no CAUTIs were reported. Team members identified one HAPI during quarterly prevalence rounds. Eradicating HAPI on the unit became a strategic goal. The action plan included education, reviewing risk reduction strategies, and performing “it takes two” assessments (two sets of eyes to assess the skin when patients are admitted).
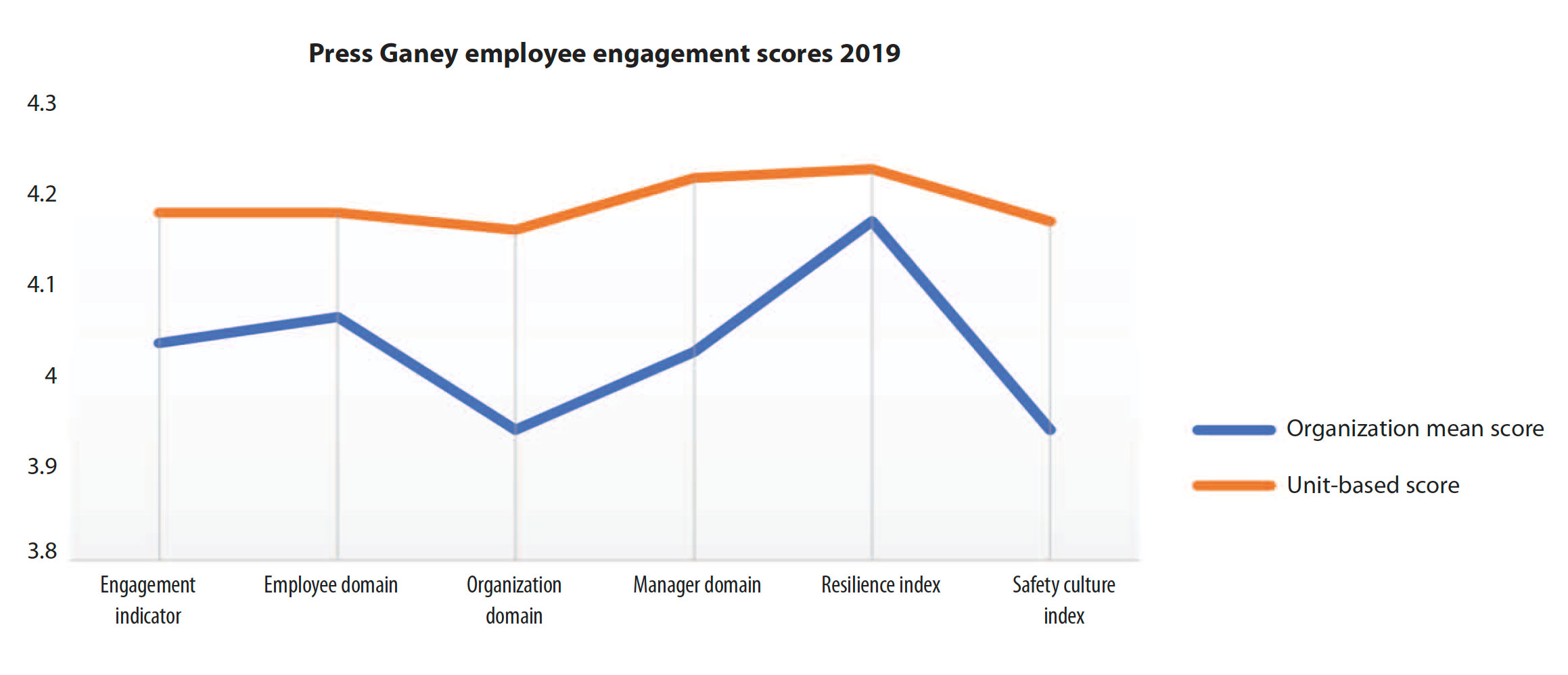
On organizational staff engagement surveys, this unit outperformed the mean—they’re engaged and less likely to express an intention to leave, and they perceive their work as high quality and that they have control over unit decisions. These high engagement scores illustrate that the unit has progressed from the storming to the norming phase of team formation. (See Engaged workforce.)
Engaged workforce
Based on results for six key areas (each ranked on a scale of 0 to 5), employee engagement scores indicate that the new unit operates above the organization mean.
Supported and trusted
High nurse and nurse technician engagement on this new unit facilitated top performance in the care transition domain of the Hospital Consumer Assessment of Healthcare Providers and Systems survey. Scores averaged in the 95th percentile within two quarters of opening the unit. Patient experience scores have ranked in the top 25th percentile for the past 6 out of 7 months and have ranked in the top 10th percentile for the past 4 out of 7 months.
Although the unit expanded from 14 beds to a maximum capacity of 23 beds within a year, the UPC developed an innovative model to engage newly hired staff members in creating a practice environment that supports quality outcomes and promotes a safer environment. Clinical nurses at the bedside drive improved practice, and the professional governance structure conveys a message that nurses are supported and trusted to make critical decisions that impact patient care. AN
The authors work at Emory University Hospital in Atlanta, Georgia. Teresa Costley is a clinical nurse specialist. Diaz Clark is a nurse scholar.
References
Clavelle JT, Porter O’Grady T, Weston MJ, Verran JA. Evolution of structural empowerment: Moving from shared to professional governance. J Nurs Adm. 2016;46(6):308-12.
Dempsey C, Reilly BA. Nurse engagement: What are the contributing factors for success? Online J Issues Nurs. 2016;21(1):2.
De Simone S, Planta A, Cicotto G. The role of job satisfaction, work engagement, self-efficacy and agentic capacities on nurses’ turnover intention and patient satisfaction. Appl Nurs Res. 2018;39:130-40.
Guanci G, Medeiros M. Shared Governance That Works. Minneapolis, MN: Creative Health Care Management; 2018.
Institute for Healthcare Improvement. ISBAR trip tick. ihi.org/resources/Pages/Tools/ISBARTripTick.aspx
Kutney-Lee A, Germack H, Hatfield L, et al. Nurse engagement in shared governance and patient and nurse outcomes. J Nurs Adm. 2016;46(11):605-12.
Porter-O’Grady T. Principles for sustaining shared/professional governance in nursing. Nurs Manage. 2019;50(1):36-41.
Porter-O’Grady T, Malloch K. Unit 3. In: Managing for Success in Healthcare. St. Louis, MO: Mosby; 2007; 253-55.
Tuckman BW. Developmental sequence in small groups. Psychol Bull. 1965;63(6):384-99.


















1 Comment.
Sounds easy but we all know its not right?