
With collaboration and creativity, we can shift the culture.
- Nurses across the profession have experienced increased stress and distress, which has only intensified during the global pandemic
- Despite efforts, limited accessible options exist for nurses to participate in psychologically informed and specifically tailored interventions to decrease distress and burnout and increase resiliency
- Proactive approaches focused on prevention rather than reaction can aid mitigation of nursing stress and burnout.
The COVID-19 pandemic has been the ultimate stress test for our taxed healthcare system, and despite nurses’ immense fortitude, the effects of this stress have landed unfairly on their shoulders. Although central to every aspect of healthcare operations and patient care, nurses haven’t received much-needed psychosocial support, which has resulted in unbearably high levels of psychological and moral distress, work-related stress, and occupational burnout. As a result, more nurses are leaving the profession and hospitals face challenges with staff recruitment and retention. Although these issues have existed for quite some time, the pandemic has made them impossible to ignore.
Healthy schedules, healthy nurses
Learn about the five constructs of the healthy nurse.
ANA launches Healthy Nurse program
Burnout (physical, mental, and emotional exhaustion as a result of stress) and resilience (an ability to cope effectively and adapt to significant life stressors) have received much attention in nursing recently. However, specific programming implementation has been slow. Notably, nurses plead with their organizations for programs to help them cope proactively with stress and distress and to provide them with support and resources to continue doing their jobs effectively. Interventions exist to address burnout and increase resilience for healthcare workers broadly and specifically for nurses (for example, the Community Resiliency Model®, Mindfulness Based Stress Reduction, and cognitive behavioral and mindfulness-based programming). However, their availability varies across healthcare institutions, and many nurses have difficulty participating because of job-related responsibilities. To effect meaningful and lasting change for nurses, organizations must formally prioritize developing and integrating these programs.
As a hospital psychologist at Massachusetts General Hospital (MGH) in Boston, I’ve spent time with nurses on and off the unit trying to better understand their needs and next steps. In an effort to improve the physical, mental, emotional, and social well-being of nurse colleagues, I created several nurse support programs following four distinct developmental phases (including resolving a few notable issues) that can be applied across various settings.
Phase 1: Addressing nurses needs
Before the COVID-19 pandemic, I worked in my hospital’s Neuro-ICU as a clinical psychologist on a federally funded clinical trial for patient and informal caregivers. When rounding the unit to check on patients and families, I also checked in with nurses and learned about their universal stress, work demands, interpersonal challenges of working with others under stress, as well as how they managed stress personally and professionally. From these conversations, I began conceptualizing a support group for nurses that included teaching psychosocial skills aimed at addressing issues of emotional distress and burnout.
Support groups, as opposed to other forms of treatment (individual therapy, coaching), allow nurses to share with and encourage each other and to enhance social learning by acquiring coping skills from one another through conversation and modeling. Conversations with nurses, the nurse director, and unit nurse leaders helped to inform the original nurse support program and identified gaps in support and psychosocial skills training. From these discussions, I developed an informal psychologically informed nurse support group to reduce emotional distress (depression, anxiety, and secondary post-traumatic stress disorder [PTSD]) before it becomes chronic and to improve coping skills.
Several core skills for these group sessions mirrored the program delivered to patients and caregivers in our ICU. In addition, the initial programming used evidence-based, third-wave behavioral psychotherapy approaches, which included skills such as mindfulness, dialectics, cognitive defusion, acceptance, and relaxation. The sessions also offered opportunities to strengthen general coping, interpersonal bonds, values, and social support. I collaborated with the unit social worker when delivering these groups—meeting in person with nursing staff once a week before the pandemic (March 2019 to March 2020), and then every 2 weeks virtually during the pandemic (April 2020 to July 2020) for 60-minute sessions. Attendance varied week to week, with two to eight nurses in regular attendance.
Although I provided initial structure to the support group with psychoeducation, we kept conversations organic and related to common nursing challenges, such as patient and family issues, critical incidents on the unit (codes, poor outcomes), and interpersonal challenges (issues among colleagues, residents, fellows, attendings, specialty services, administrators). The social worker and I prioritized group support over specific skill delivery, as well as experiential learning (as opposed to didactic) to enhance social engagement. Because the group’s primary intention was as a clinical service, we didn’t collect any data.
Although many nurse participants provided positive feedback on the program, no formal infrastructure existed for the program to continue after my time on the federally funded clinical trial ended. In addition, lack of funding and waning attendance during the pandemic led the group to end prematurely in late summer of 2020. However, I formed early impressions from these initial groups, including the need to remove barriers for nurse attendance—such as financial (protected time to attend sessions) and logistical (scheduling, shift covering)—and to promote the relevance and value of such programming as a proactive vs. reactive response to nurse stress and burnout.
Phase 2: Piloting a formal nurse support program
After the informal nurse support program in the Neuro-ICU, I began making connections with colleagues at other hospitals to offer the program to help promote their staff’s resiliency as well as to help me develop and pilot the program. In 2020, I secured funding to pilot a 6-month nurse support program (six 60-minute sessions) for six early career (<2 years) nurses working at another Neuro-ICU in New England. I based the formal program curriculum on the original informal support program and collected quality improvement (QI) data to help shape future delivery. (See Phase 2 curriculum)
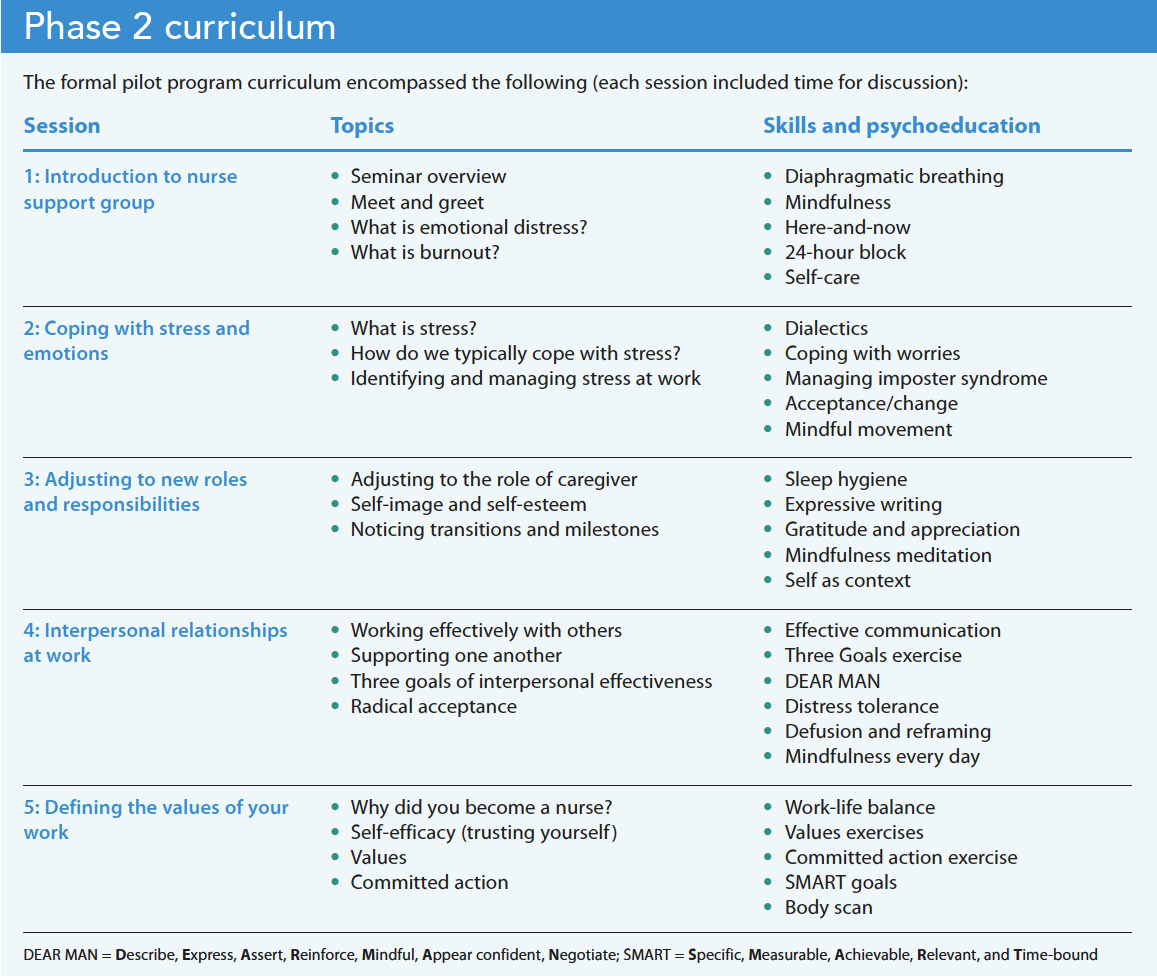
QI data and anecdotal accounts from these groups suggested the program was well-received and helped address on-the-job nursing stressors. Nurses described the program as helpful in building a stronger sense of community. This initial version of the nurse support and resiliency program led to piloting the program in a structured way and thinking about future development and delivery. Meeting once a month presented challenges in terms of continuity, but program consistency (first Wednesday of every month) aided attendance. However, even with the predictability of the schedule, these nurses had limited time to participate in groups. I considered how to deliver stress-reduction, resilience, and community-building skills in less time.
Phase 3: Creating two workshops
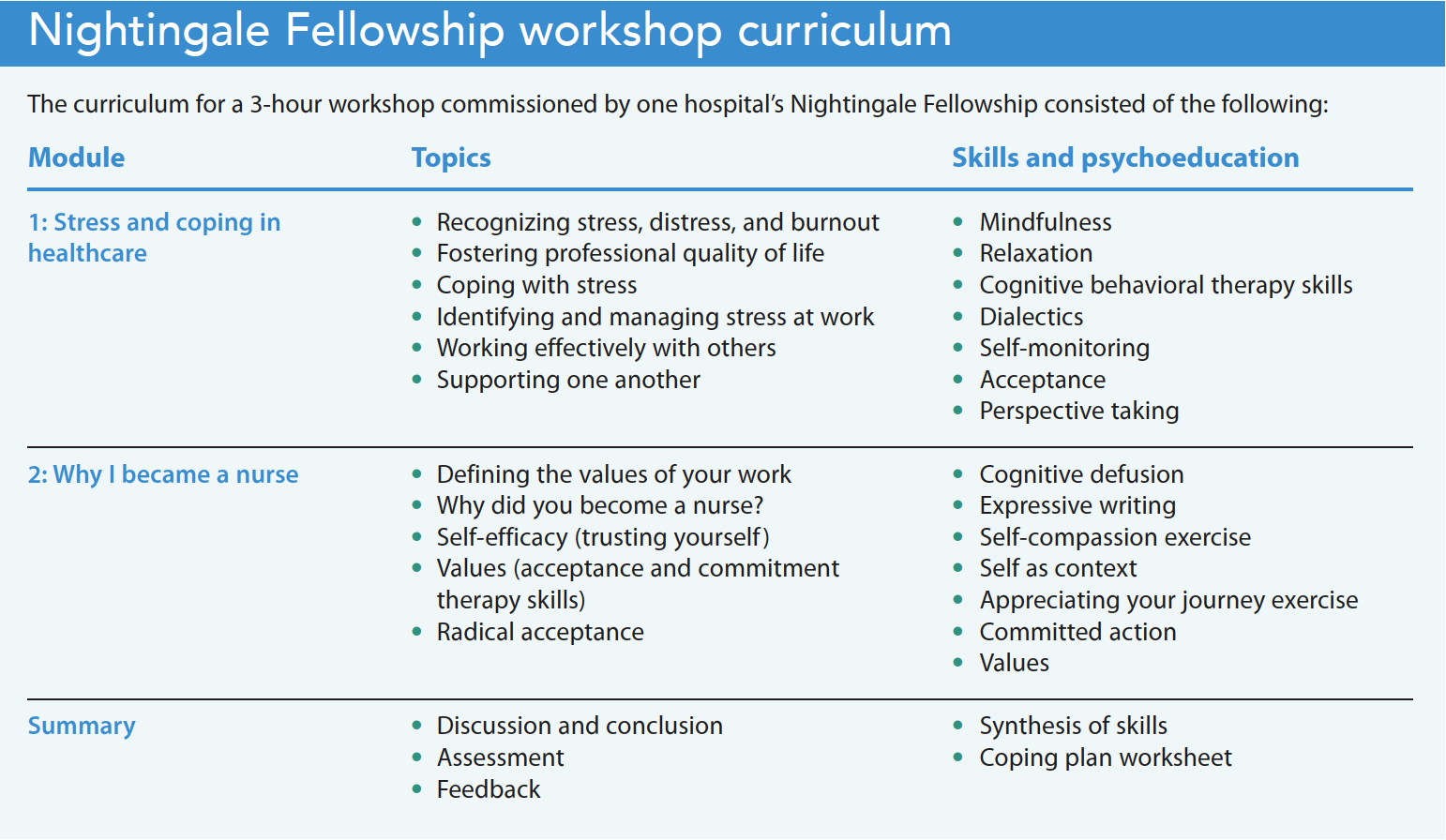
The need for nurse support increased during the pandemic as topics of moral distress (an inconsistency between beliefs and actions), moral residue (the result of moral distress when one feels that their integrity has been compromised), and delayed PTSD (when onset of PTSD occurs after 6+ months) became more common among nurse leaders at my hospitals. In the winter of 2021, the Nightingale Fellowship (a 2-year fellowship program that emphasizes professional development through education, assigned mentorship, and individualized learning experiences in nurses) at one of the hospitals invited me to design and pilot a 3-hour workshop version of the program for nurse fellows on leadership paths.
Before designing this workshop, I analyzed feedback from the 6-month nurse pilot program and informally interviewed two nurse colleagues at my organization to help adapt it for a rehabilitation nurse audience (needs-based adaptation) and to reconstruct core content (mindfulness, coping, social support, self-efficacy, and values) into two modules, each lasting 1.5 hours. (See Nightingale Fellowship workshop curriculum)
Although I didn’t collect data from this workshop, the general feedback I received proved valuable. Fellows noted the relevance of skills (mindfulness, fostering psychological flexibility, values, self-reflection, social support, and self-efficacy) to the nursing profession. They also shared that these exercises provided opportunities to reflect on their coping strategies as well as to reconnect with the value of their work as nurses. The fellowship director provided feedback via email, stating, “[The workshop] was a highlight in our two-year journey as fellows,” and that conversations about how to integrate these skills into their units radiated across fellows for days after the presentation. She mentioned that the fellows expressed the desire to be “ambassadors” of these psychosocial skills and that they planned to carry this knowledge back to their respective teams. The director said it best: “…it is within our reach to create this needed change, and perhaps our duty, to implement strategies and build relationships that bring satisfaction and dare I say, joy, to our work.”
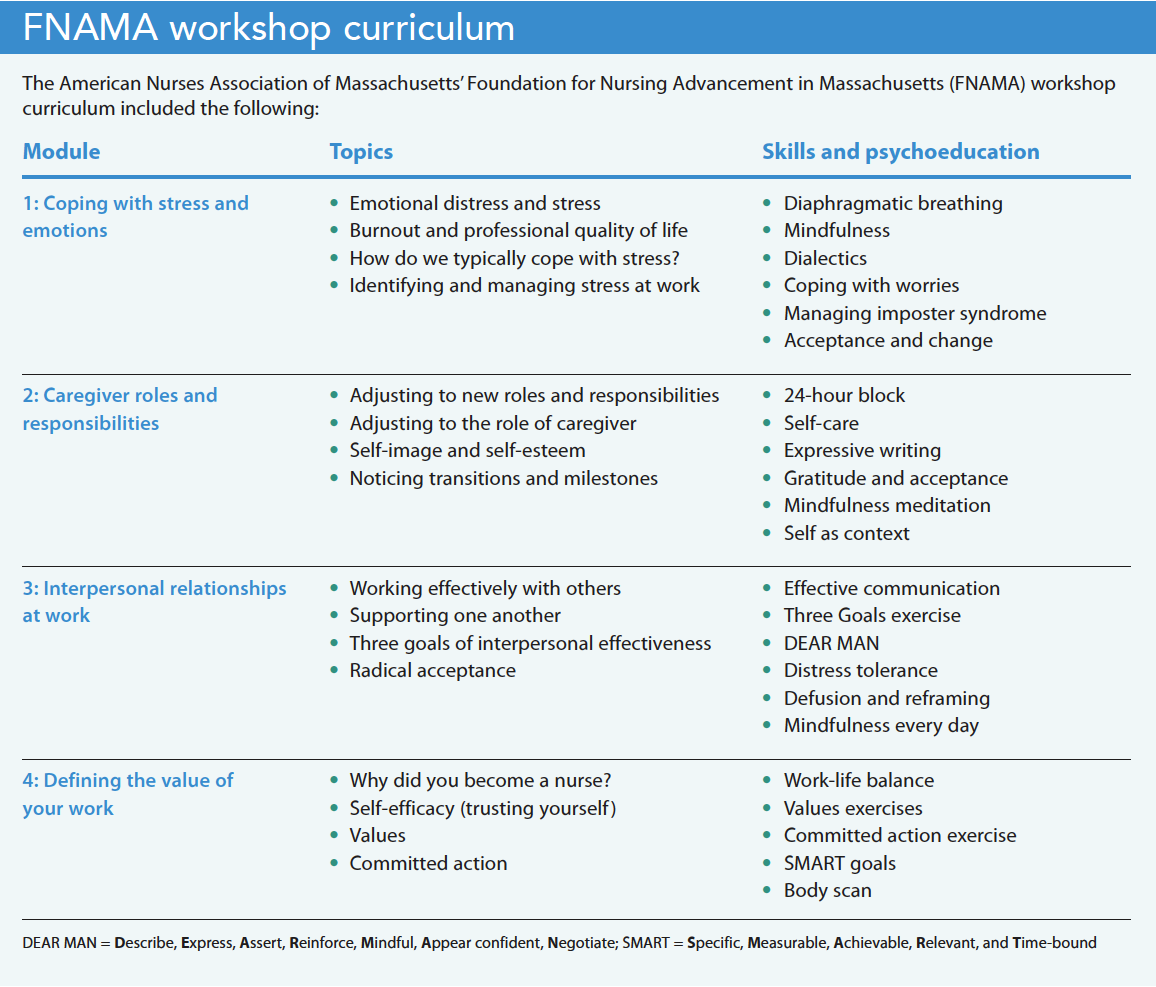
In early 2022, the nurse director at the MGH Neuro-ICU connected me with the American Nurses Association of Massachusetts’ Foundation for Nursing Advancement in Massachusetts (FNAMA), which was interested in holding their first in-person nursing forum to help connect nurses with one another in their organization. They wanted to hire a facilitator to present psychosocial skills for managing stress, increasing resiliency, and creating professional networks with nurses across the state. With several months to plan, I designed a 6-hour workshop (with breaks), titled “Moving from surviving to thriving: Resetting, recentering, restoring ourselves,” which included four core modules (Coping with Stress and Emotions, Caregiver Roles and Responsibilities, Interpersonal Relationships at Work, and Defining the Value of Your Work).
Similar to the original program, this workshop prioritized experiential learning and social connection among the attendees. The FNAMA submitted the curriculum for approval and offered 4 continuing education units (CEUs) for participation. The organization rented conference space; provided breakfast, coffee, and lunch; and offered the workshop for free to all RNs in Massachusetts. (See FNAMA curriculum.)
We collected data on this workshop, including demographic information and satisfaction (Client Satisfaction Questionnaire; CSQ) and qualitative feedback from participants. Most attendees (N = 75) were women (>95%), middle-aged (median age = 48; standard deviation [SD] = 11.9), and had served >20 years (SD = 12.4) in the profession. At the end of the workshop, nurses (N = 72) who completed the survey endorsed high satisfaction with the program (CSQ median score = 30 [out of a total possible 32]; SD = 2.8) and provided positive feedback on the workshop’s effects on their well-being and coping. Anecdotally, several nurses commented on the importance and relevance of the content. One nurse noted that she had recently started her first sabbatical after 24 years as a nurse because of the stress, burnout, and vicarious trauma she experienced during the pandemic. She remarked that the workshop provided “a breath of fresh air” and encouraged her to continue seeking mental health support and resources during her time off.
Phase 4: Developing two abbreviated nurse support modules
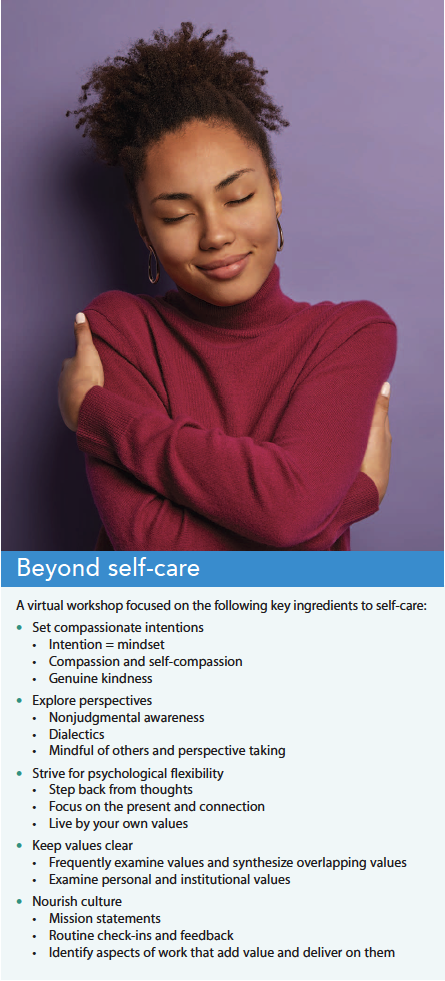 In the most recent development of the nurse support program, a local hospital in the greater Boston area asked for two specific talks (mini-workshops) as part of a day-long, hospital-sponsored summit for National Nurses Month in 2022. Both hour-long talks offered CEU opportunities for attending nurses. The first, a webinar, titled “Beyond self-care: Simple strategies for increasing wellness and resiliency at work,” allowed nurses to log-in live and at their convenience. The webinar addressed typical (and frequently unhelpful) conversations about self-care and burnout and highlighted key ingredients for creating more nurturing work environments for nurses. (See Beyond self-care.)
In the most recent development of the nurse support program, a local hospital in the greater Boston area asked for two specific talks (mini-workshops) as part of a day-long, hospital-sponsored summit for National Nurses Month in 2022. Both hour-long talks offered CEU opportunities for attending nurses. The first, a webinar, titled “Beyond self-care: Simple strategies for increasing wellness and resiliency at work,” allowed nurses to log-in live and at their convenience. The webinar addressed typical (and frequently unhelpful) conversations about self-care and burnout and highlighted key ingredients for creating more nurturing work environments for nurses. (See Beyond self-care.)
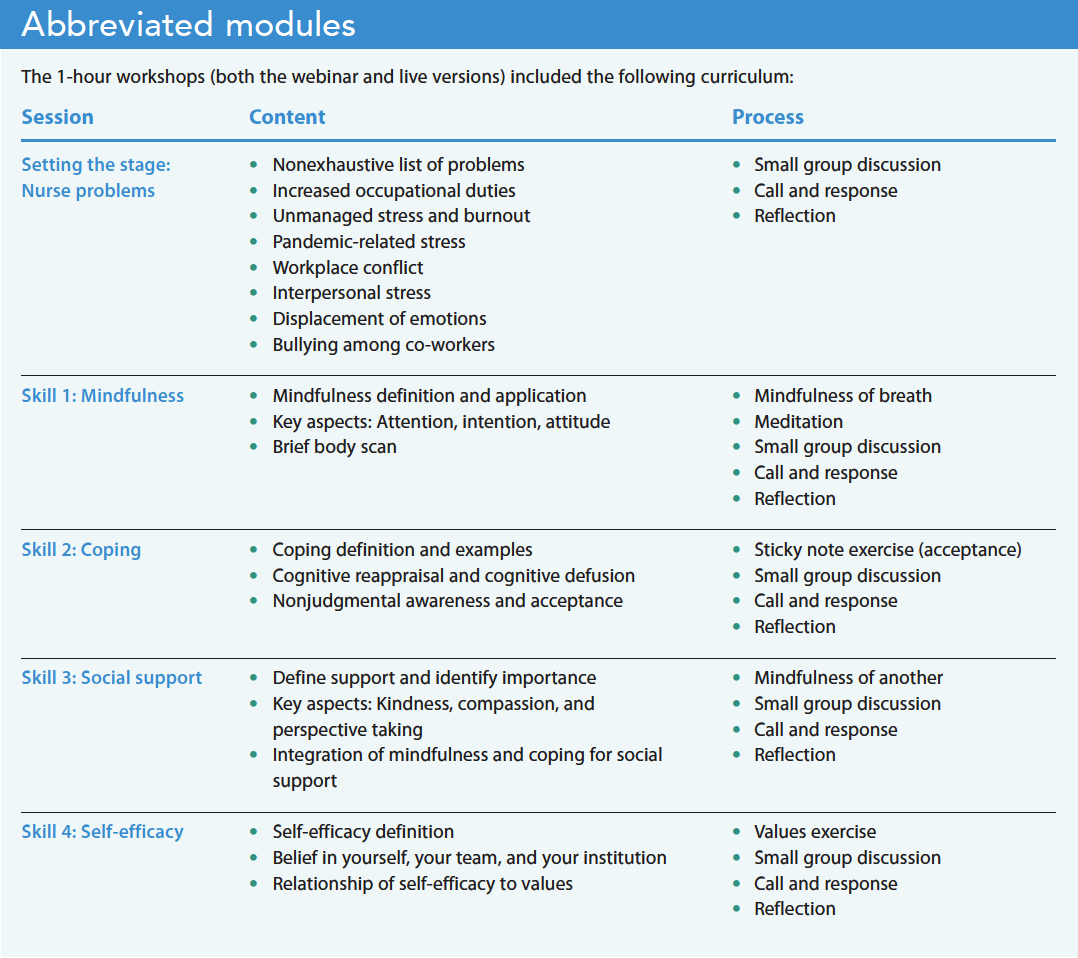
For the second talk, a live 1-hour presentation titled “Workplace well-being: Caring for yourself and your team,” the organization paid nurses for their time and provided breakfast, lunch, and refreshments. Challenges in designing this talk included rendering the most essential content from longer workshops and facilitating audience engagement within an hour. The presentation included “pair and share” (turning to a fellow nurse at your table), small group discussion, “call and response” (asking the audience, “Who has…”), and personal reflection (sitting silently, writing exercises) to enhance audience engagement and experiential learning. Similar to the other programs, the presentation prioritized community building via socializing and small group activities. (See Abbreviated modules.)
Next steps
The pandemic highlighted the rising rates of PTSD, anxiety, depression, and emotional exhaustion among nurses, as well as their association with negative aspects of the work environment (organizational support, safety, workplace relations). Nursing needs solutions to address these issues, and I argue that nurse support initiatives benefit from being psychologically informed and tailored to nurses’ specific needs.
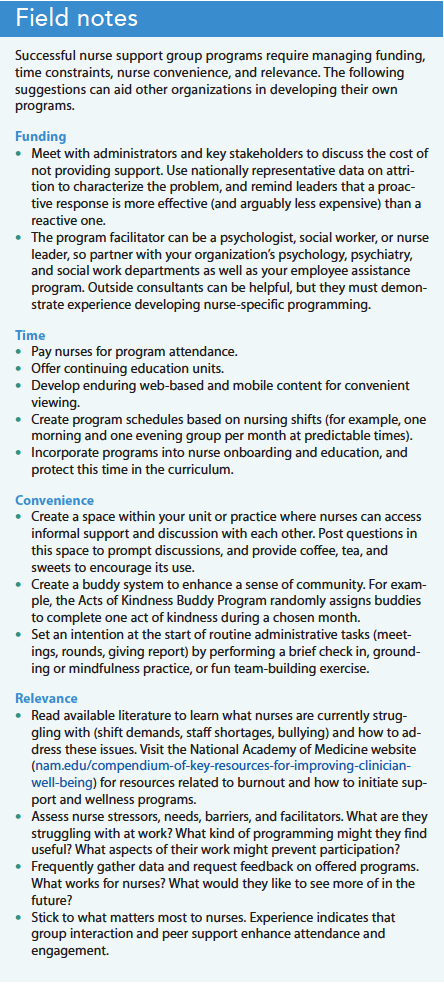
Development and delivery of these programs were not linear or simple. I faced several temporal, financial, and institutional challenges, and I also experienced my own burnout. But from these experiences, I also gathered useful field notes about what works, from which other organizations can benefit. (See Field notes.)
Nurse support and resiliency programs may not be especially innovative, but when we work collaboratively (nurses, doctors, psychologists, administrators) and creatively, we can shift the culture from reaction to prevention of these familiar problems.
Ethan G. Lester is a clinical psychologist at Massachusetts General Hospital, Mass Eye and Ear, and Spaulding Rehabilitation Hospital. He’s also an assistant professor at Harvard Medical School in Boston.
Disclosure: The author received payment from the Foundation for Nursing Advancement in Massachusetts, Yale New Haven Hospital, Newton Wellesley Hospital, and Spaulding Rehabilitation Hospital for the workshops described in this article.
References:
Arnetz JE, Goetz CM, Arnetz BB, Arble E. Nurse reports of stressful situations during the COVID-19 pandemic: Qualitative analysis of survey responses. Int J Environ Res Pub Health. 2020;17(21):8126. doi:10.3390/ijerph17218126
Attkisson CC, Greenfield TK. Client Satisfaction Questionnaire-8 and Service Satisfaction Scale-30. In: Maruish ME, ed. The Use of Psychological Testing for Treatment Planning and Outcome Assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1994.
Brown S, Whichello R, Price S. The impact of resiliency on nurse burnout: An integrative literature review. Medsurg Nurs. 2018;27(6):349-78.
Cleary M, Kornhaber R, Thapa DK, West S, Visentin D. The effectiveness of interventions to improve resilience among health professionals: A systematic review. Nurse Educ Today. 2018;71:247-63. doi:10.1016/j.nedt.2018.10.002
Da Rosa P, Brown R, Pravecek B, et al. Factors associated with nurses emotional distress during the COVID-19 pandemic. Appl Nurs Res. 2021;62:151502. doi:10.1016/j.apnr.2021.151502
Dall’Ora C, Ball J, Reinius M, Griffiths P. Burnout in nursing: A theoretical review. Hum Resour Health. 2020;18(1):41. doi:10.1186/s12960-020-00469-9
al Falasi B, al Mazrouei M, al Ali M, et al. Prevalence and determinants of immediate and long-term PTSD consequences of coronavirus-related (CoV-1 and CoV-2) pandemics among healthcare professionals: A systematic review and meta-analysis. Int J Environ Res Pub Health. 2021;18(4):2182. doi:10.3390/ijerph18042182
Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J Adv Nurs. 2021;77(8):3286-3302. doi:10.1111/jan.14839
Ghawadra SF, Abdullah KL, Choo WY, Phang CK. Mindfulness‐based stress reduction for psychological distress among nurses: A systematic review. J Clin Nurs. 2019;28(21-22):3747-58. doi:10.1111/jocn.14987
Grabbe L, Higgins MK, Baird M, Craven PA, San Fratello S. The Community Resiliency Model® to promote nurse well-being. Nurs Outlook. 2020;68(3):324-36. doi:10.1016/j.outlook.2019.11.002
Hardingham LB. Integrity and moral residue: Nurses as participants in a moral community. Nurs Philos. 2004;5(2):127-34. doi:10.1111/j.1466-769X.2004.00160.x
Havaei F, Ma A, Staempfli S, MacPhee M. Nurses’ workplace conditions impacting their mental health during COVID-19: A cross-sectional survey study. Healthcare (Basel). 2021;9(1):84. doi:10.3390/healthcare9010084
Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change. 2nd ed. New York, NY: Guilford Press; 2016.
Henshall C, Davey Z, Jackson D. Nursing resilience interventions—A way forward in challenging healthcare territories. J Clin Nurs. 2020;29(19-20):3597-9. doi:10.1111/jocn.15276
Kakemam E, Raeissi P, Raoofi S, et al. Occupational stress and associated risk factors among nurses: A cross-sectional study. Contemp Nurse. 2019;55(2-3):237-49. doi:10.1080/10376178.2019.1647791
Labrague LJ. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. J Nurs Manag. 2021;29(7):1893-1905. doi:10.1111/jonm.13336
Lee KA, Friese CR. Deaths by suicide among registered nurses: A rapid response call. J Psychosoc Nurs Ment Health Serv. 2021;59(8):3-4. doi:10.3928/02793695-20210625-01
Leng M, Wei L, Shi X, et al. Mental distress and influencing factors in nurses caring for patients with COVID‐19. Nurs Crit Care. 2021;26(2):94-101. doi:10.1111/nicc.12528
Li ZS, Hasson F. Resilience, stress, and psychological well-being in nursing students: A systematic review. Nurse Educ Today. 2020;90:104440. doi:10.1016/j.nedt.2020.104440
Linehan MM. DBT Skills Training Manual. 2nd ed. New York, NY: Guilford Publications; 2014.
Lorente L, Vera M, Peiró T. Nurses’ stressors and psychological distress during the COVID‐19 pandemic: The mediating role of coping and resilience. J Adv Nurs. 2021;77(3):1335-44. doi:10.1111/jan.14695
Pollock A, Campbell P, Cheyne J, et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst Rev. 2020;11(11):CD013779. doi:10.1002/14651858.CD013779
Ralph J, Freeman LA, Ménard AD, Soucie K. Practical strategies and the need for psychological support: Recommendations from nurses working in hospitals during the COVID-19 pandemic. J Health Organ Manag. 2021;36(2):240-55. doi:10.1108/JHOM-02-2021-0051
Slatyer S, Craigie M, Heritage B, Davis S, Rees C. Evaluating the Effectiveness of a brief mindful self-care and resiliency (MSCR) intervention for nurses: A controlled trial. Mindfulness. 2018;9(2):534-46. doi:10.1007/s12671-017-0795-x
Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;5:1-14. doi:10.3402/ejpt.v5.25338
Vranceanu AM, Bannon S, Mace R, et al. Feasibility and efficacy of a resiliency intervention for the prevention of chronic emotional distress among survivor–caregiver dyads admitted to the neuroscience intensive care unit: A randomized clinical trial. JAMA Netw Open. 2020;3(10):e2020807. doi:10.1001/jamanetworkopen.2020.20807
Yu F, Raphael D, Mackay L, Smith M, King A. Personal and work-related factors associated with nurse resilience: A systematic review. Int J Nurs Stud. 2019;93:129-40. doi:10.1016/j.ijnurstu.2019.02.014
Zhang X, Jiang X, Ni P, et al. Association between resilience and burnout of front‐line nurses at the peak of the COVID‐19 pandemic: Positive and negative affect as mediators in Wuhan. Int J Ment Health Nurs. 2021;30(4):939-54. doi:10.1111/inm.12847
Key words: nurse support, psychosocial support, resiliency, burnout, pandemic


















{kind=link}
1 Comment. Leave new
Acknowledgements:
Many heartfelt thanks to the participants and attendees of the various nurse support programs mentioned in this paper – this work is for you.
Personnel Support: Ana-Maria Vranceanu, Victoria Grunberg, Olivia Higgins, David Hwang, Nona Timario, Tara Tehan, Roger “Gino” Chisari, Christopher Carter, Lauren Williams, Maureen Banks, Martha Rafferty, Suzanne Murdok, Kimberly Foisy, Deborah Wilson, Christina Cassidy, & Celia Kampner
Programmatic Support: The Center for Health Outcomes and Interdisciplinary Research, Massachusetts General Hospital Neuro-ICU, Yale New Haven Hospital Neuro ICU, Spaulding Rehabilitation Hospital, the Foundation for Nursing Advancement in Massachusetts, Newton Wellesley Hospital, Mass General Brigham