A free clinic system’s quality-improvement project aims to improve care.
- Nurse practitioners frequently provide care in medically underserved areas of the United States, often in free clinics.
- Patients who access care at free clinics frequently meet the diagnostic criteria for posttraumatic stress disorder (PTSD) and as a result have difficulty with interpersonal interactions, mobility, self-care, and overall poorer health outcomes.
- Nurses can effectively lead quality improvement teams to increase identification of and care for patients diagnosed with PTSD.
Many nurse practitioners (NPs) provide care in medically underserved areas, some in one of the more than 1,400 free clinics throughout the United States. More patients who access care at free clinics meet the diagnostic criteria for posttraumatic stress disorder (PTSD) than those who receive care at fee-for-service clinics. Many of these patients face various challenges, including being immigrants or refugees, surviving human trafficking or domestic violence, and living unsheltered.
The lifetime prevalence rates of PTSD for survivors of traumatic events range from 9.1% for domestic violence, 31.46% for refugees, 32% for those living unsheltered, and 41% for survivors of human sex trafficking. However, providers working in free clinics don’t routinely screen or treat these patients for PTSD.
Implementing trauma-informed care
Children and post-traumatic stress disorder
Why it matters
PTSD, which develops after exposure to one or more traumatic events, includes various symptoms and chronic physical and mental health disorders associated with social, occupational, and physical disability. Many people living with PTSD have difficulty with interpersonal interactions and relationships, mobility, and self-care issues; they also have poorer health outcomes overall. In addition to the burden on personal health, a significant economic burden also exists. In 2018, the most recent year for which data are available, Davis and colleagues reported the total cost of PTSD in the United States at $232.2 billion or $19,630 per individual diagnosed with PTSD.
The challenge
Similar to those who seek care at other free clinics across the country, individuals using the free clinic system in southern California face a high risk for PTSD. Despite their increased risk for the disorder and related comorbidities, these patients didn’t receive routine screening for the condition. To meet this need, we formed a quality improvement (QI) project team to address the lack of screening for and treatment of PTSD in adults, 18 years of age and older, who access care in the free clinic system.
Comprising three free clinics in three cities in southern California, the QI project took place between December 9, 2022, and April 28, 2023. The project team included the NP project lead, the clinic executive director, the clinic manager, and two subject matter experts in QI project implementation. The team performed a literature review, selected a guiding framework, and identified the project’s goals.
Literature review
In our search of the literature from 2017 to 2022, we found available treatments for PTSD and associated comorbidities; however, identifying the condition requires providers to recognize its signs and symptoms. Once identified, providers can initiate treatment according to evidence-based research, expert opinion, and patient preference. Evidence-based clinical practice guidelines can effectively increase provider knowledge and improve screening and treatment.
Guiding framework
The project team selected Graham’s Knowledge-to-Action (KTA) framework to guide the project because several other projects had successfully used it to implement practice guidelines while ensuring they remained practical at the local level. The KTA framework includes two cycles: knowledge creation and action.
Consistent with the KTA framework action cycle, the project team reviewed five high-quality PTSD clinical practice guidelines. They chose the 2017 Veterans Affairs/Department of Defense Management of Posttraumatic Stress Disorder and Acute Stress Reaction (VA/DoD PTSD) guideline because of the recommendations’ quality and specificity and the availability of several free online resources for patients and providers at the National Center for PTSD (ptsd.va.gov).
Project goals
Before implementing the VA/DoD PTSD guideline, the project team developed three specific, measurable, achievable, relevant, and time-bound (SMART) goals to achieve within 4 months: 80% of all adult patients, 18 years and older, who accessed care at the free clinic would receive PTSD screening using the 5-item Primary Care PTSD Checklist for the DSM-5 (PC-PTSD-5); 80% of those who tested positive would receive a referral for treatment; and 80% of those would receive treatment.
What we did
We used a multiple time series design to determine whether implementing the VA/DoD PTSD guidelines achieved our increased screening, referral, and treatment goals. To evaluate the effect of the intervention, we monitored data weekly and collected it retrospectively from the electronic health record (EHR).
We started the QI project at the free clinic sites after receiving clinic leadership and Institutional Review Board approval. Project participants included the NP project lead, the clinic manager, office manager, 5 front office staff, 15 volunteer healthcare providers (NPs, physicians, physician assistants [PAs]), 2 RNs, 38 RN students, 33 family NP (FNP) students, and 15 PA students.
A formal orientation for volunteers, staff, and students introduced them to the project and the VA/DoD PTSD guideline. They also completed a free web-based training video series (PTSD 101), which incorporates evidence-based guidance for the screening, referral, and treatment of PTSD.
Guided by the KTA framework, specific project activities included adaptation of the VA/DoD PTSD guideline to local contexts, which resulted in the development of the SoCalCC PTSD Treatment and Referral Protocol. We developed this two-page protocol to remind staff, students, and volunteers of all the necessary steps in the free clinic screening, referral, and treatment process.
Additional project activities included adding the PC-PTSD-5 to the clinics’ patient check-in protocol; placing PTSD pocket cards in charting areas and emailing electronic copies to all clinic providers; using the PTSD Checklist for DSM-5 (PCL-5) to monitor patients diagnosed with PTSD; and providing weekly coaching, on-site or remotely, for staff, students, and volunteers.
Using weekly chart audits, we tracked clinic staff, volunteers, and student participation. The audits helped us determine whether screening, treatment, and/or referrals for PTSD were being conducted according to the SoCalCC PTSD Treatment and Referral Protocol and the VA/DoD PTSD guideline. If the audit revealed any inappropriate screening, referral, or treatment, we contacted the individuals involved for additional coaching.
Screening and monitoring instruments
We used the five-item PC-PTSD-5 to screen patients for PTSD and the 20-item PCL-5 to monitor the progress of patients diagnosed with and treated for PTSD. We selected these instruments based on their reported reliability and validity. In a 2003 study conducted to develop the PC-PTSD-5 and in follow-on studies conducted in 2016 and 2021 to evaluate the instrument’s psychometrics, Prins and colleagues and Cheng and colleagues reported good test-retest reliability (r = .83), an internal consistency alpha of .83, and predictive validity against the clinician-administered PTSD Scale 0 (r = 0.83). In several studies conducted between 2010 and 2022 to evaluate the psychometric properties of the PCL-5, McDonald, Wilkins, Blevins, and Forkus, along with their colleagues, reported test-retest reliability ranging from .66 to .90, an internal consistency alpha ranging from .83 to .98, and indications for convergent and discriminant validity.
Data collection and analysis
We collected data from the free clinic system’s EHR, which included the number of adults screened using the PC-PTSD-5, monitored for treatment effectiveness using the PCL-5 and patient record review, and summed the total number of patients treated or referred for PTSD over the course of the project. We entered the data into a Microsoft Excel Workbook.
We performed data analysis using the Excel Data Analysis Tool Pack and the add-in software XLSTAT. We calculated percentages monthly for 4 months post-intervention. Next, we generated run charts to illustrate the changes in screening rates that occurred after implementation of the VA/DoD PTSD guideline. The Chi-square test and the Cochran–Mantel–Haenszel (CMH) test, an extension of the Chi-square test, helped us determine whether time in the intervention and/or clinic site where care occurred affected the percentage of adults screened, treated, or referred. We set statistical significance at alpha .05 for all statistical tests.
What we learned
For 4 months before the intervention, a total of 481 unique patients accessed care at the three free clinics; during that time, two patients received a diagnosis of and treatment for PTSD. At the end of the 4-month intervention, 630 patient encounters occurred (representing 476 unique patients). Of those 476 patients, 81% (n = 386) received PTSD screening and 45 individuals screened positive for PTSD (a 4-month prevalence rate of 9.5%). Of those 45 positive screens, 14 patients received a diagnosis of PTSD and received treatment in the free clinic system. This represented a statistically significant increase in patients treated for PTSD.
Characteristics of patient encounters
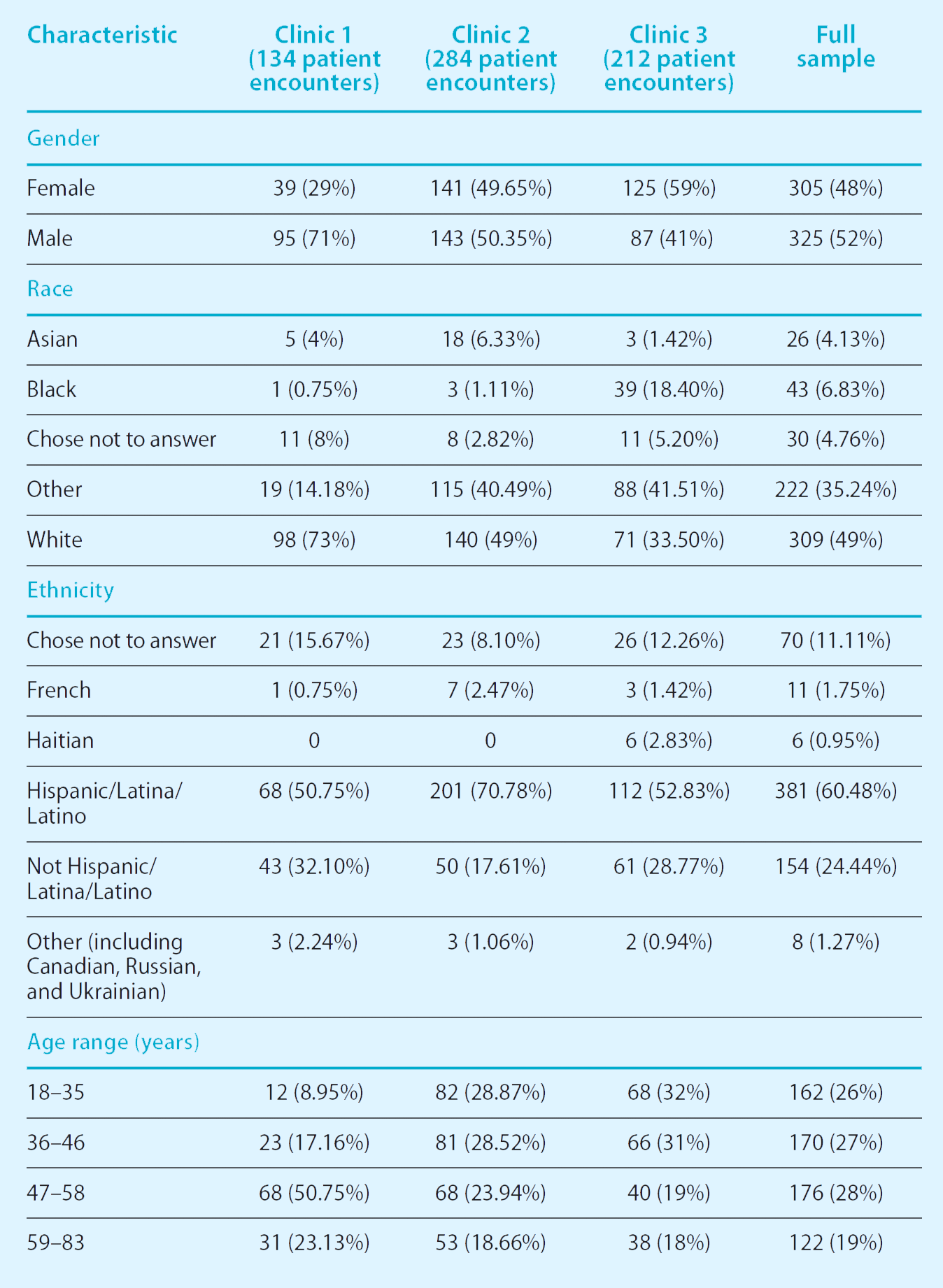
We evaluated the demographic characteristics of all 630 patient encounters that occurred during the QI project. At Clinic 1, the mean age was 54.43 years (SD = 11.44 years) with most patients (71%) identifying as male and White (73%). At Clinic 2, the mean age was 42 years (SD = 13.93 years) with gender evenly split between males and females; most (71%) patients at Clinic 2 identified as Hispanic/Latina/Latino. At Clinic 3, the mean age was 44 years (SD = 14.73) with slightly more females (59%) than males (41%); 53% of patients identified as Hispanic/Latina/Latino. (See Patient demographics.)
Patient demographics
Patient demographics vary by clinic location (476 unique patients, 630 patient encounters between January 10, 2022, and April 30, 2023). We found a statistically significant difference by clinic in age [F(2, 627) = 3.01, p < .001], gender [χ2 (2, n = 630) = 29.62, p <.001], and self-reported race [χ2 (8, n = 630) = 123.33, p <.001] and ethnicity [χ2 (10, n = 630) = 39.22, p <.001].
Project goals
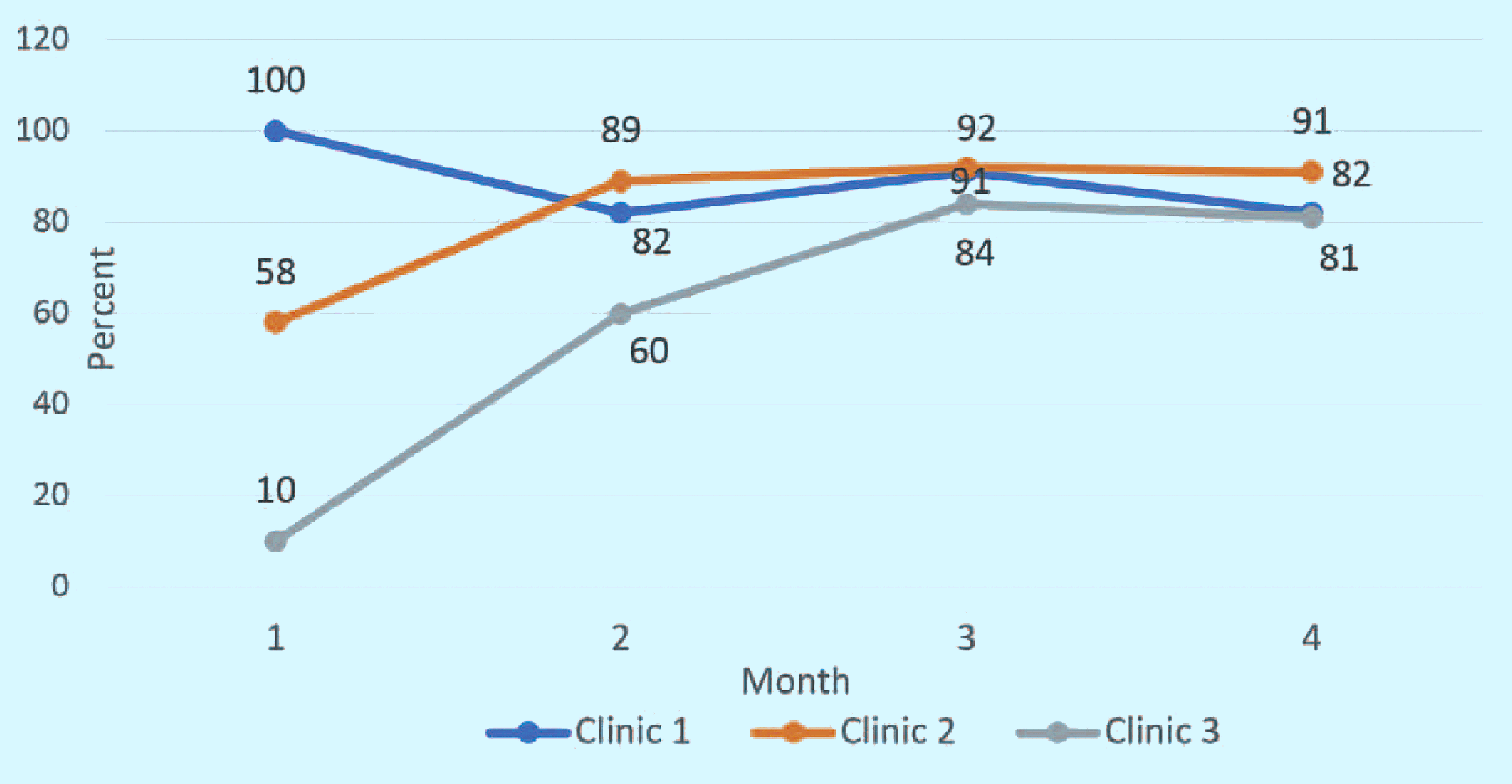
We met the first project goal. Four months after implementing the VA/DoD PTSD guideline, more than 80% of all adult patients, age 18 years and older, who accessed care in the free clinic system received screening for PTSD using the 5-item PC-PTSD-5. When we evaluated each clinic separately for rates of screening, referral, and treatment, we found a noticeable difference in the percentage of patients screened for PTSD. We performed additional analyses to determine if time in the intervention or clinic where patients received care affected screening rates. (See Goal 1: Screening outcomes.)
Goal 1: Screening outcomes
We achieved our first goal (80% of all adult patients, 18 years and older, will receive post-traumatic stress disorder [PTSD] screening by the end of the 4-month intervention using the 5-item Primary Care PTSD Checklist for the DSM-5). Note that the clinic location had a statistically significant effect on the percentage of patients screened [M2 = (1, n = 630) = 93.291, p <.001].
We partially met the second project goal—referral. Of the patients who received a positive screen for PTSD (n = 45), providers referred 75% (n = 34) for further evaluation during the 4-month intervention. This metric varied by clinic; Clinics 1 and 2 reached 100% in month two but dropped to 50% in month three. Clinic 3 made no referrals for patients who screened positive.
We met the third project goal—treatment. Of the 14 patients who received a diagnosis of PTSD, 13 elected to obtain care (according to the VA/DoD PTSD guideline) at the free clinics.
Additional findings
Two additional findings related to documentation and return on investment resulted from this intervention.
Inadequate documentation. During the intervention, we conducted weekly spot checks of patient records to ensure coaching could take place around screening, referral, or treatment practices that didn’t follow recommendations of the VA/DoD PTSD guidelines. We found that as many as 66% of screenings and referrals for further evaluation and treatment, although performed, weren’t being documented in the EHR.
Return on investment. To determine the cost effectiveness and sustainability of the project, we evaluated the potential return on investment. The total non-personnel cost of the 4-month project was $20,600; personnel expenses were donated. We then developed a projected profit-and-loss statement for the next fiscal year.
The indicators used to cost out the project included the free clinic system 4-month prevalence rate range for a positive PTSD screen of 9.5% to 17% (between 200 and 300 patients), projected expenses (including non-personnel and personnel), and projected net revenue (including donations, grants, and MediCal reimbursement). We calculated the projected profit–loss statement for the QI project for fiscal year 2024 by subtracting total projected expenses from projected net revenue with an anticipated profit range of $146,200 to $219,300.
What the results tell us
Screening for PTSD in free clinics is feasible and increases identification rates and referral and treatment for PTSD. By month four of the intervention, between 81% and 91% of patients were being screened for PTSD depending on the clinic at which the patient accessed care. The majority (75%) of those who screened positive were referred for further evaluation, and most (93%) of the patients diagnosed with PTSD who received care for the disorder at the free clinics were treated according to the VA/DoD PTSD guideline.
We calculated the 4-month prevalence rate for a positive PTSD screen at 9.5%. This percentage was lower than expected based on previous observational studies that put prevalence rates for at-risk populations who access care at free clinics between 30% and 48%. This rate is more consistent with PTSD prevalence rates at fee-for-service primary care clinics (between 2% and 11%).
We may have set the cut-off point for a positive PC-PTSD-5 screen too high at a score of 3. Recent psychometric evaluations of the PC-PTSD-5 in younger, non-White, non-English-speaking populations support this possibility. In our project, 36 patients scored a 2 on the PC-PTSD-5. If we had used that lower cut-off point, 81 patients would have screened positive for PTSD (prevalence rate of 17%).
Multiple factors can affect screening, referral, and treatment rates in free clinic settings. In this QI project, Clinic 3 had the lowest screening, referral, and treatment rates. Our investigation found that delays in scanning the screening instrument into the EHR, appointment type (immigration physicals), and an insufficient number of interpreters to screen patients who spoke languages other than Spanish and English may have contributed to these low rates.
The United States has a shortage of medical interpreters, and limitations exist in the number of languages offered by translation services. Communication barriers can lead to poor outcomes for patients, whereas access to professional medical interpreters can improve patient–provider communication and patient outcomes. To meet this identified need, the clinic system hired an additional interpreter who speaks Haitian Creole, Spanish, and English for Clinic 3.
The type of medical appointment may affect the ability to screen for a particular disorder. For example, immigration physicals may not include any additional information such as screening results for PTSD. In addition, patients who receive an immigration physical may move to another part of the state shortly afterward. In accordance with the revised SoCalCC PTSD Treatment and Referral Protocol, the clinic system’s current practice includes PTSD screening when individuals return for follow-up appointments after completing immigration physicals.
Weaknesses and limitations</h3 > The inability to add the PC-PTSD-5 to the EHR during the project contributed to the low documentation rates of positive PTSD screens and referrals for further evaluation and treatment. The project depended on outcome data from the EHR. Other studies have noted the challenge of using EHRs to assess outcomes, which can result in missing data and failure to include relevant measures (such as questionnaires), both of which presented issues for this project.
Strengths
The strengths of this project included the guiding framework, stakeholder buy-in, design, sample size, and sustainability. Using the KTA framework encouraged modification of the VA/DoD PTSD guideline for local context, which enhanced sustainability. The multiple time series design allowed for data collection over 4 months and strengthened our ability to attribute findings to the intervention. After completing the project, we conducted a post hoc power analysis using the Chi-square test statistic with a sample size of 476, an alpha of .002, one degree of freedom, and an effect size of 0.40. The sample sizes (630 encounters with 476 unique patients) provided a power of greater than .90.
Nursing implications
Findings from this QI project included inadequate documentation of patient screening and referrals. As described by the American Nurses Association, communication of patient needs to the healthcare team and successful evidence-based nursing practice require accurate documentation. RNs and APRNs must work to ensure clear, accurate, and accessible documentation across healthcare organizations.
The addition of necessary screening tools to the EHR can improve documentation processes and evaluation of patient outcomes; however, not all screening tools may be valid across all patient populations. We recommend additional research with the PC-PTSD-5 to evaluate its reliability, validity, and utility across diverse patient populations.
Since the implementation of this project, an updated VA/DoD PTSD clinical practice guideline has been published. You can learn more about PTSD, including the updated clinical practice guideline, at the National Center for PTSD (ptsd.va.gov).
Linnea M. Axman is the associate dean for graduate programs in the College of Nursing at University of Phoenix in Phoenix, Arizona. Richard Prior is senior associate dean for academic affairs in the College of Nursing at University of Cincinnati in Cincinnati, Ohio. Jason Saude is a clinical nurse manager at University of California San Diego Health in La Jolla. Mary L. Baker is director of quality and systems integration at Lestonnac Free Clinic in Orange, California.
American Nurse Journal. 2025; 20(4). Doi: 10.51256/ANJ042553
References
American Nurses Association. ANA’s principles for nursing documentation: Guidance for registered nurses. 2010. nursingworld.org/globalassets/docs/ana/ethics/principles-of-nursing-documentation.pdf
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR). Washington, DC: American Psychiatric Association; 2022.
Blackmore R, Boyle JA, Fazel M, et al. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLoS Med. 2020;17(9):e1003337. doi:10.1371/journal.pmed.1003337
Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J Trauma Stress. 2015;28(6):489-98. doi:10.1002/jts.22059
Cheng P, Jasinski N, Zheng W, et al. Psychometric properties of the primary care PTSD screen for DSM-5: Findings from family members of Chinese healthcare workers during the outbreak of COVID-19. Front Psychiatry. 2021;12:695678. doi:10.3389/fpsyt.2021.695678
Courtois CA, Sonis J, Brown LS, et al; Guideline Development Panel for the Treatment of Posttraumatic Stress Disorder (PTSD) in Adults. Clinical Practice Guideline for The treatment of Posttraumatic Stress Disorder (PTSD) in Adults. American Psychological Association. 2017. apa.org/ptsd-guideline/ptsd.pdf
Davis LL, Schein J, Cloutier M, et al. The economic burden of posttraumatic stress disorder in the United States from a societal perspective. J Clin Psychiatry. 2022;83(3):21m14116. doi:10.4088/jcp.21m14116
Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder. 2017. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal.pdf
Field B, Booth A, Ilott I, Gerrish K. Using the Knowledge to Action Framework in practice: A citation analysis and systematic review. Implement Sci. 2014;9:172. doi:10.1186/s13012-014-0172-2
Forkus SR, Raudales AM, Rafiuddin HS, Weiss NH, Messman BA, Contractor AA. The posttraumatic stress disorder (PTSD) checklist for DSM-5: A systematic review of existing psychometric evidence. Clin Psychol. 2023;30(1):110-21. doi:10.1037/cps0000111
Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: Time for a map? J Contin Educ Health Prof. 2006;26(1):13-24. doi:10.1002/chp.47
Prins A, Bovin MJ, Smolenski DJ, et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and evaluation within a veteran primary care sample. J Gen Intern Med. 2016;31(10):1206-11. doi:10.1007/s11606-016-3703-5
Prins A, Ouimette P, Kimerling R, et al. The primary care PTSD screen (PC-PTSD): development and operating characteristics. Primary Care Psychiatry. 2003;9(1):9-14. doi:10.1185/135525703125002360
McDonald SD, Calhoun PS. The diagnostic accuracy of the PTSD checklist: a critical review. Clin Psychol Rev. 2010;30(8):976-87. doi:10.1016/j.cpr.2010.06.012
Saude J, Baker ML, Axman LM, Swider SM. Applying the chronic care model to improve patient activation at a nurse-managed student-run free clinic for medically underserved people. SAGE Open Nurs. 2020;6:2377960820902612. doi:10.1177/2377960820902612
Tsai J, Schick V, Hernandez B, Pietrzak RH. Is homelessness a traumatic event? Results from the 2019-2020 National Health and Resilience in Veterans Study. Depress Anxiety. 2020;37(11):1137-45. doi:10.1002/da.23098
Vogt D, Mangan E. Research on women, trauma, and PTSD. U.S. Department of Veterans Affairs. ptsd.va.gov/professional/treat/specific/ptsd_research_women.asp
Weathers FW, Litz, BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP. PTSD Checklist for DSM-5 (PCL-5). National Center for PTSD. 2023. ptsd.va.gov/professional/assessment/documents/PCL5_Standard_form.PDF
Wilkins KC, Lang AJ, Norman SB. Synthesis of the psychometric properties of the PTSD checklist (PCL) military, civilian, and specific versions. Depress Anxiety. 2011;28(7):596-606. doi:10.1002/da.20837
Key words: Posttraumatic stress disorder, clinical practice guideline, quality improvement, free clinics


















