
Simple nurse actions can ensure patients feel safe and empowered.
- Trauma-informed care is a core component of nursing practice.
- Nurses must implement universal strategies to prevent retraumatizing patients.
- Nursing school curricula should include education about trauma.
Childhood trauma (adverse childhood experiences [ACEs]) can result in severe mental and physical consequences that reverberate throughout a person’s life. Despite the widespread occurrence of ACEs, most nurses remain unaware of their long-term, negative effects. Many nursing tasks—touching a patient’s body, asking questions about past sexual history or abuse—can trigger retraumatization. If you routinely implement trauma-informed care (TIC), you can help reduce the risk of re-traumatizing patients. (See About trauma.)
Trauma screening
The prevalence of trauma requires screening of all patients in all healthcare settings. Universal trauma screening increases the chances of a patient reporting their trauma history. According to Palmieri and Valentine, 82% of sexual assault and intimate partner violence survivors would report a traumatic event with appropriate screening measures; whereas, only 24% would disclose their trauma history if not properly screened. Many patients may not disclose trauma information out of fear of retraumatization. Proper screening can help patients feel more comfortable and provide them with the support they need.
Helping patients who harm themselves
Long-term health outcomes of childhood sexual abuse
However, trauma screening doesn’t occur during most healthcare visits and a substantial amount of trauma history goes unnoticed. This lack of screening and education about the importance of TIC makes nurses’ bedside behavior critical to preventing patient retraumatization.
About trauma
The Substance Abuse Mental Health Services Administration (SAMHSA) defines trauma as “an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life-threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being.” Adverse childhood events (ACEs) occur between birth and age 18 and can include neglect, witnessing or experiencing emotional or physical abuse, sexual assault, and living in a household with challenges such as parental divorce or separation, household member incarceration, or a parent with serious mental illness or substance use disorder.
According to SAMHSA, more than two-thirds of children report at least one traumatic event by age 16. Although the actual trauma may subside by adolescence, emotional effects, psychological consequences, and health complications can follow the individual well into adulthood. The Centers for Disease Control and Prevention estimates that 61% of adults have experienced at least one type of ACE, and nearly one in six report having experienced four or more types.
Trauma and the brain
Trauma’s main effect on the brain involves the hippocampus (the memory center), the amygdala (the fear center), and the prefrontal cortex (the center that regulates emotions and controls functions). They work simultaneously to manage stress. When an individual thinks about a past traumatic event, the amygdala is activated while the prefrontal cortex is suppressed. This results in the body being overcome with fear but unable to control the feeling.
As the brain’s memory center, the hippocampus also is responsible for distinguishing between the present and the past. When having a traumatic thought, the hippocampus becomes less active, and the brain can’t distinguish between actual trauma and a memory. The brain perceives the memory as an actual threat, placing it in an elevated alert state, and making the person feel trapped in their own, never-ending emotions.
Trauma affects
The effects of ACEs can manifest throughout an individual’s life, from childhood through adolescence and into adulthood.
Childhood
Childhood trauma increases the risk of developing psychological distress, anxiety, and depression. These conditions can present as physical symptoms (stomachaches, headaches), disruptive behavior (including unexplained anger), lack of focus, obsessive worrying, irritability, sleep disturbances, and appetite changes. The effects of trauma make it hard for children to form and maintain relationships with peers and may prevent them from succeeding in school. Some children can move into adolescence without any effects from their past trauma, but most experience several challenges.
Adolescence
For adolescents, childhood trauma may remain a constant and disturbing memory that leads to depression and anxiety. They may find it hard to talk about their past trauma because they can’t trust others or they feel different from those who haven’t had similar experiences. Some adolescents suffer from post-traumatic stress disorder (PTSD), and most don’t receive the treatment they need.
Adolescents may use drugs or alcohol to repress traumatic memories. Substance use disorders among adolescents are linked to higher rates of school failure, a lack of social skills, low activity participation, memory-related issues, increased suicide rates, liver dysfunction, and death from alcohol poisoning.
In addition, traumatized adolescents may exhibit reckless behavior, such as driving carelessly, having unprotected sex with multiple partners, and participating in violent activity. All of these behaviors can result in life-changing outcomes, including sexually transmitted infection, pregnancy, incarceration, physical injury, or death. Campbell and colleagues state that female adolescents who are sexually victimized have substantially higher risks for sexual or physical abuse in adulthood. Although the percentage of sexual abuse remains higher in females, the risk for experiencing abuse in adulthood also increases when a male has been sexually abused as a child.
Adulthood
Adults who’ve experienced childhood trauma have higher risks for depression, anxiety, and PTSD. Adolescent risky behaviors may worsen, and substance use disorder may become more prevalent. Increased behaviors in adulthood amplify the risk for their detrimental consequences.
Some adults may not display the typical behavioral signs of distress; however, repressed trauma may manifest in conditions that require medical attention, including asthma, severe migraines, depression, pulmonary disease, obesity, cancer, and inflammatory diseases. Those with past trauma also are significantly more likely than those without to seek mental and physical healthcare later in life.
TIC approach
By taking a TIC approach, you assume that all patients have experienced past trauma and tailor your behavior to prevent retraumatization. TIC emphasizes physical, psychological, and emotional safety. It creates opportunities to rebuild a patient’s sense of control and empowerment by ensuring they feel safe and comfortable, respecting personal space, using nonthreatening body language, paying attention to patient cues, and communicating clearly. TIC promotes an environment of healing by reducing distress and providing emotional support and resources. (See 5 key ingredients of TIC.)
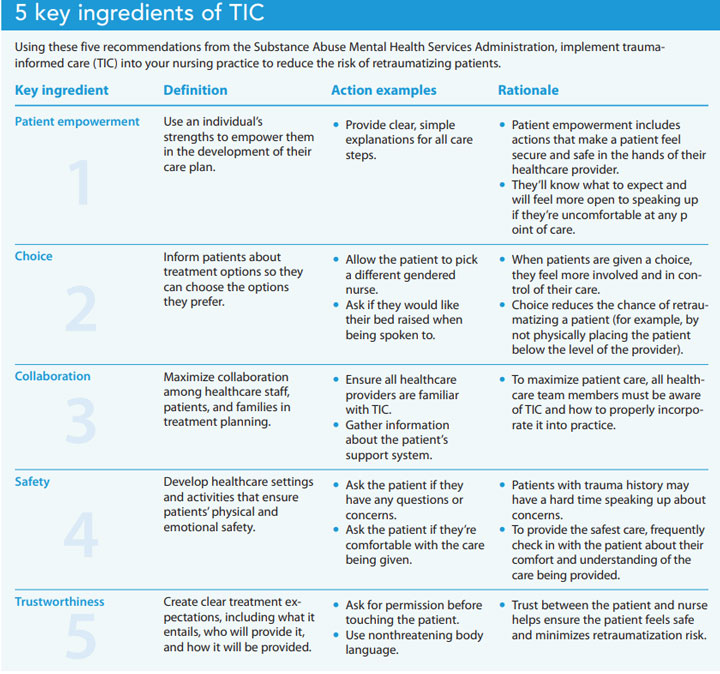
5 key ingredients of TIC
Using these five recommendations from the Substance Abuse Mental Health Services Administration, implement trauma-informed care (TIC) into your nursing practice to reduce the risk of retraumatizing patients.
Reducing the risk for retraumatization
Retraumatization occurs when an individual consciously or unconsciously re-experiences a previous trauma, which can be triggered by a similar environment, a smell, an image, a new relationship that mimics a previous one, or a healthcare visit. Everyday nursing actions can help reduce the risk for retraumatization. For every patient interaction, introduce yourself and explain your role, use open and nonthreatening body language, assure patients that you’ll protect their privacy, and describe care and assessments, especially before touching the patient. Always use clear, simple explanations for discharge and treatment instructions, as well as teach-back to confirm patients understand. (See Preventing retraumatization.)
Preventing retraumatization
These simple, yet effective, patient-centered steps can significantly reduce retraumatization.
- Provide trauma screening for all patients to identify those with a history of trauma.
- Recognize the signs of retraumatization, including sudden anxiousness, restlessness, fear, avoidance, social isolation, despair, fatigue, physical reactions (such as putting up their hands), and an inability to control emotions.
- Be mindful of secondary trauma, which can lead to chronic fatigue, disturbing thoughts, poor concentration, emotional detachment, avoidance, absenteeism, and physical illness. Nurses and other front-line staff experiencing these symptoms may struggle to provide high-quality care and experience burnout, leading to staff turnover.
- Learn about the importance of trauma-informed care (TIC), and advocate for changes in your organization to become trauma informed.
- Advocate for trauma and TIC education in nursing school curriculum and on-the-job training.
Enhance patient safety and comfort
Frequently, universal trauma screening isn’t implemented during patient encounters, making bedside TIC crucial to ensure patients who’ve experienced trauma feel safe. Consistent trauma screening for all patients, trauma and TIC education implemented in nursing education curriculum, and workplace retraining can help healthcare providers better understand the effects of ACEs and enhance patient comfort, safety, and sense of control during healthcare encounters.
Ally Buettel is an RN at NYU Langone Health in Mineola, New York. Marissa D. Abram is an assistant professor at Adelphi University College of Nursing and Public Health in Garden City, New York.
References
Agorastos A, Pervanidou P, Chrousos GP, Baker DG. Developmental trajectories of early life stress and trauma: A narrative review on neurobiological aspects beyond stress system dysregulation. Front Psychiatry. 2019;10:118. doi:10.3389/fpsyt.2019.00118
Bransford C, Cole M. Trauma-informed care in homelessness service settings: Challenges and opportunities. In: Larkin H, Aykanian A, Streeter CL eds. Homelessness Prevention and Intervention in Social Work. New York, NY: Springer Publishing; 2019; 255-77.
Butler LD, Maguin E, Carello J. Retraumatization mediates the effect of adverse childhood experiences on clinical training-related secondary traumatic stress symptoms. J Trauma Dissociation. 2018;19:25-38. doi:10.1080/15299732.2017.1304488
Campbell R, Greeson MR, Bybee D, Raja S. The co-occurrence of childhood sexual abuse, adult sexual assault, intimate partner violence, and sexual harassment: A mediational model of posttraumatic stress disorder and physical health outcomes. J Consult Clin Psychol. 2008;76(2):194-207. doi:10.1037/0022-006X.76.2.194
Centers for Disease Control and Prevention. Preventing adverse childhood experiences. April 6, 2022.
Cohen JR, Menon SV, Shorey RC, Le VD, Temple JR. The distal consequences of physical and emotional neglect in emerging adults: A Person-centered, multi-wave, longitudinal study. Child Abuse Negl. 2017;63:151-61. doi:10.1016/j.chiabu.2016.11.030
Dye H. The impact and long-term effects of childhood trauma. J Hum Behav Soc Environ. 2018;28(3):381-92. doi: 10.1080/10911359.2018.1435328
Fleishman J, Kamsky H, Sundborg S. Trauma-informed nursing practice. Online J Issues Nurs. 2019;24(2). doi:10.3912/OJIN.Vol24No02Man03
Li Y, Cannon LM, Coolidge EM, Darling-Fisher CS, Pardee M, Kuzma EK. Current state of trauma-informed education in the health sciences: Lessons for nursing. J Nurs Educ. 2019;58(2):93-101. doi:10.3928/01484834-20190122-06.
Palmieri J, Valentine JL. Using trauma-informed care to address sexual assault and intimate partner violence in primary care. J Nurse Pract. 2020;17(1):44-8. doi:10/1016/j.nurpa.2020.08.028
Saiyed S, Chozom T, Saiyed S, Bender A. Getting to know our patients through the lens of trauma informed care. J Am Med Dir Assoc. 2021;22(3):B12. doi:10.1016/j.jamda.2021.01.027
Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. July 2014.
Key words: trauma-informed care, adverse childhood experiences, trauma-informed nursing


















3 Comments. Leave new
thanks for info.
I agree this is such an important topic and I deeply wish TIC and easier and affordable access to counseling becomes a center practice in health care. My master’s project last year was on TIC with my PICO question being “In adults who have encountered adverse childhood experiences, does a trauma- informed care approach improve healthy lifestyle behavior changes as compared to motivational interviewing without being trauma informed?” All articles supported the implementation of trauma-informed care into primary care practices with the proposed outcomes of decreasing chronic disease and high-risk behaviors by addressing trauma early.
Many chronic health problems in adults are linked to adverse childhood experiences (ACE). In the mental health field, trauma-informed care as an intervention has proven positive mental health outcomes in clients, and a large amount of literature recommends screening for ACE’s early in primary care to improve health. However, there is limited information if trauma-informed care (TIC) effects behavior changes for positive health outcomes in the outpatient clinical primary care setting so more research is still needed. Because, in my research, “sixty-two articles within the last 15 years reviewed, only four implemented trauma informed care and two articles incorporated motivational interviewing in relation to adverse childhood experiences that met the 5-year criteria” for evidenced base practice (EBP), with only one article as level II research, and 5 articles as level III research.
I worked in a Psychiatric Hospital that was able to provide this training in a daylong inservice I was also to work with a trauma educated social worker who reinforced this teaching This needs to be a teaching for all healthcare workers I am a retired nurse after 50 years .unfortunately they do not provide this anymore due to time limitations and staff decreases