
Assessment, diagnosis, and treatment.
Takeaways:
- Any child exposed to a traumatic event can experience symptoms of post-traumatic stress disorder (PTSD).
- Children’s symptoms can be very different from those of adults.
- Early symptom recognition and treatment provides the most positive outcomes.
- The first line of treatment is cognitive behavioral therapy (CBT), particularly trauma-focused CBT.
Many children and adolescents around the world have been victims of at least one traumatic event—child abuse and neglect, war, school shootings, natural disasters, accidents and injuries, and more. According to Alisic and colleagues, an estimated 16% of them have developed post-traumatic stress disorder (PTSD).
PTSD is debilitating and can lead to chronic mental health disorders and even suicide. Many children and adolescents who suffer with PTSD have difficulty performing daily tasks and may experience alterations in their social relationships. Research indicates that they also may develop PTSD-related comorbidities, such as cardiovascular disease, later in life.
Identifying PTSD risk factors and providing effective treatment to prevent further trauma is the key to improving outcomes.
 Risk factors
Risk factors
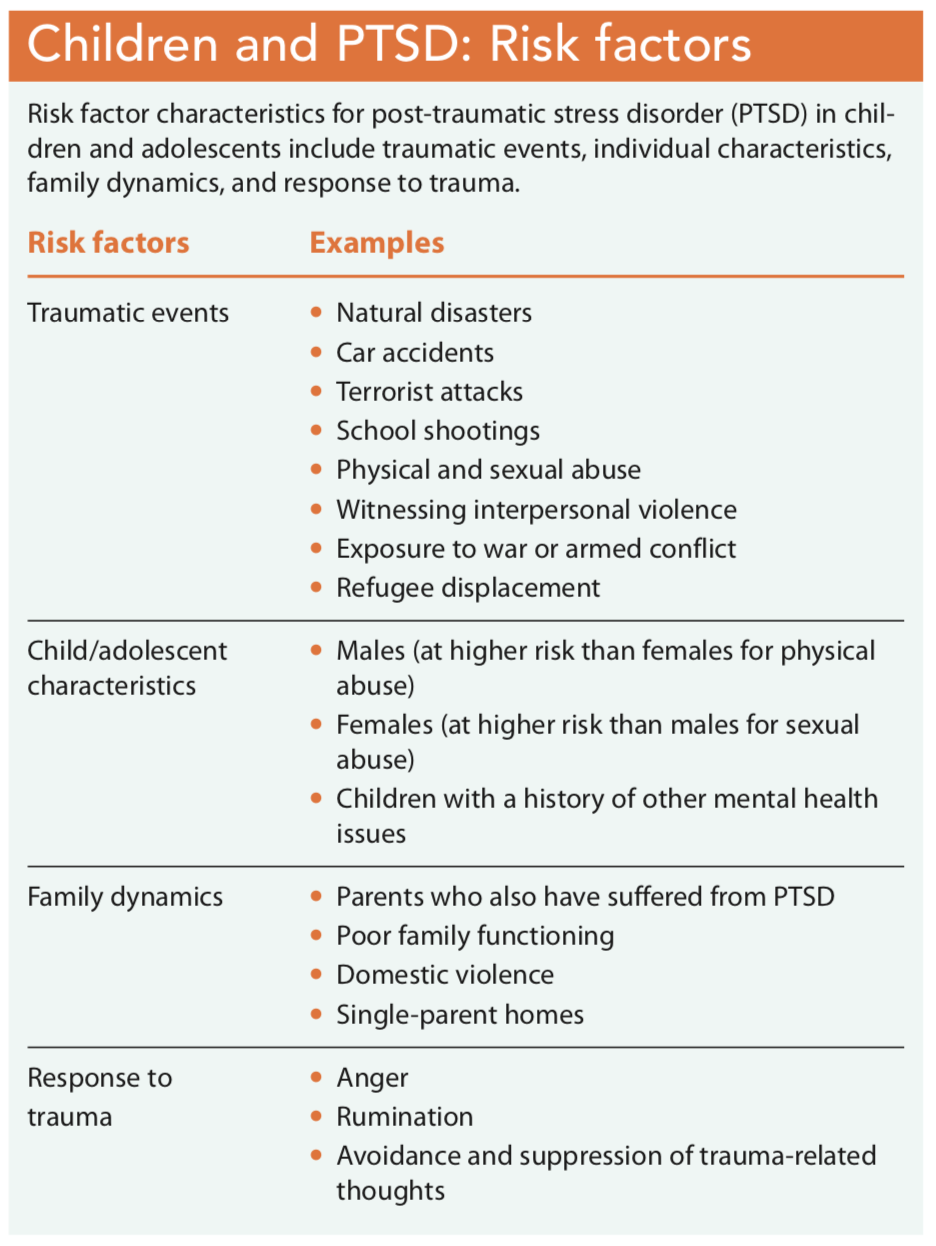
Risk for trauma exposure has many characteristics, including gender and age for all children. For example, according to McLaughlin and colleagues, males are at higher risk for exposure to physical violence than females. Females, however, are at higher risk for exposure to sexual violence. Infants and very young children are at risk for caregiver physical abuse, witnessing abuse, and kidnapping. Most children who’ve been exposed to a traumatic event have been 8 years or younger, but adolescents are at higher risk than younger children for rape and sexual assault, physical assault, automobile accident injury, and a family member’s death. Other risk factors include living in a single-parent home, low economic status, and residing in U.S. cities. Children who live in regions of the world with humanitarian emergencies such as war and armed conflict may become displaced with their families as refugees. These children may personally experience or witness brutal violence (including kidnapping, torture, and rape) and death. (See Children and PTSD: Risk factors.)
Assessment and diagnosis
PTSD assessment and diagnosis begins by determining whether the patient’s symptoms are the result of trauma or another underlying mental health disorder. Questions that can help make this determination include: Has the child directly experienced actual or threatened death, serious injury, or sexual violence; witnessed an event as it occurred to others; or learned that a close family member or friend experienced trauma? According to the Diagnostic and Statistical Manual for Mental Disorders, 5th edition (DSM-5), children (who are divided into two age categories: 6 years and older and younger than 6 years) have a lower threshold than adults for PTSD symptoms. Children with PTSD may experience signs and symptoms that fall into four categories: intrusion, avoidance, negative alterations in cognition and mood, and hyperarousal. (See PTSD signs and symptoms categories.)
Assessing the impact of trauma on a child’s ability to function in various domains—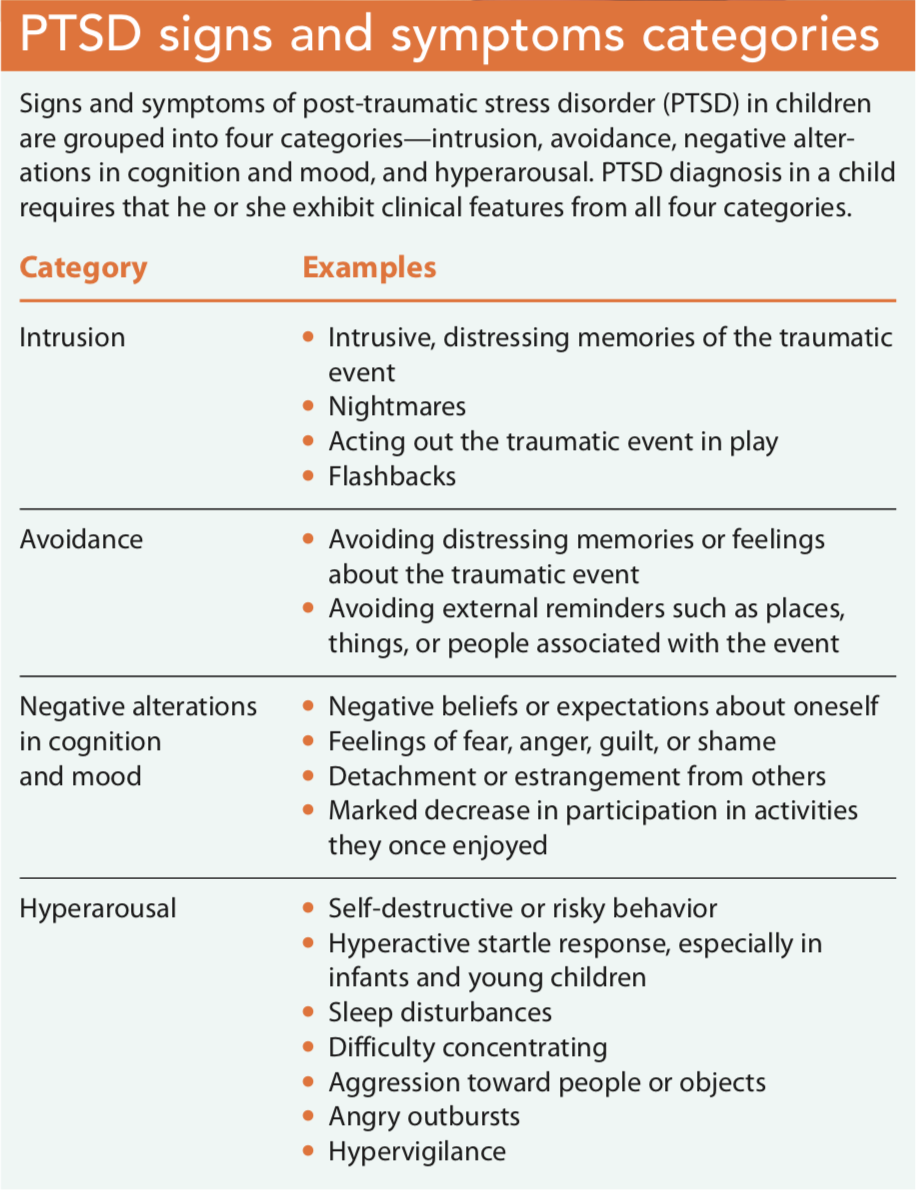 cognition, interpersonal relationships, mood and affect, family function, and trauma coping (avoidance, hypervigilance, and hyperarousal or aggression)—is important. Signs and symptoms will appear as behaviors that have a direct negative physical and cognitive impact on the child’s activities of daily function. Some children exhibit these clinical features for months or years after the traumatic event.
cognition, interpersonal relationships, mood and affect, family function, and trauma coping (avoidance, hypervigilance, and hyperarousal or aggression)—is important. Signs and symptoms will appear as behaviors that have a direct negative physical and cognitive impact on the child’s activities of daily function. Some children exhibit these clinical features for months or years after the traumatic event.
Assessing for comorbidities such as alcohol or drug dependency, generalized anxiety disorder, depression, separation disorder, and panic disorder also is important.
Assessment tools
Several assessment tools—including the University of California, Los Angeles (UCLA) PTSD Reaction Index for Children and Adolescents (PTSD-RI), and the Clinician-Administered PTSD Scale for Children and Adolescents (CAPS-CA-5)—are available to assist with diagnosing. Clinicians also should administer a suicide risk assessment to determine if an urgent need exists for inpatient assessment and treatment.
Treatment
The gold standard of treatment for children and adolescents with PTSD is trauma-focused cognitive behavioral therapy (TF-CBT). Pharmacotherapy for anxiety or depression related to PTSD may be included in conjunction with TF-CBT.
Psychosocial interventions
TF-CBT is an evidence-based treatment that should be implemented by a healthcare provider (such as a psychologist, licensed clinical social worker, or pediatric mental health nurse practitioner) who is trained in its use. The treatment involves having the child slowly reflect back on the traumatic event, allowing him or her to openly discuss it, and providing anxiety management techniques to help reduce symptoms. Several sessions may be needed before the child can comfortably think about the event and successfully use the management techniques. Parents participate in TF-CBT so they can learn to cope with their child’s PTSD symptoms.
TF-CBT also can be administered in group or community settings, such as when students experience a school shooting or in a community after a natural disaster. The treatment is especially effective and recommended as first-line treatment in children who have PTSD related to sexual abuse and display significant sexual behavioral issues (such as inappropriate touching of another child). Contraindications to TF-CBT include acute states of suicidality, psychosis, mania, drug intoxication, or severe developmental or cognitive impairment.
Play therapy can be used with younger children who can’t effectively express their thoughts about a traumatic event. The therapy uses games, drawing, and other forms of play to allow children to demonstrate their feelings and alleviate any anxiety related to the trauma.
In children with significant cognitive or developmental delays, child-parent psychotherapy is recommended because it doesn’t require intensive cognitive-based interventions. This method also is recommended for children experiencing severe attachment-related symptoms.
Pharmacotherapy
Typically, pharmacotherapy is used in conjunction with psychosocial therapy. Currently, no medications have been approved to treat PTSD in children, but studies have shown that medications such as selective serotonin reuptake inhibitors may be helpful in treating anxiety associated with PTSD. Antiadrenergic medications such as clonidine, guanfacine, and prazosin have been used to help manage nighttime symptoms, including nightmares and other sleep disturbances. Prazosin is the most widely recommended medication for sleep disturbances; guanfacine is more frequently used during the day to decrease symptoms of hyperarousal. Some children may experience nightmares when taking clonidine, in which case it should be discontinued.
If medications are part of the treatment plan, frequent monitoring for adverse effects is recommended. In addition, parents and caregivers will require education about adverse effects, expected outcomes, dosages, lab work, and follow-up visit frequency.
An interprofessional approach
PTSD symptoms and their severity in children and adolescents vary, and the nature of the trauma, the child’s age, how he or she reacts to the event, his or her developmental and cognitive ability, and the timing of diagnosis impact therapeutic outcomes. The course of PTSD symptoms also varies; research by Chowdhury and Pancha shows that approximately two-thirds of children diagnosed with PTSD recover and one-third experience long-term symptoms and chronic mental health concerns such as substance abuse, depression, anxiety, and ineffective social coping.
The key to effective treatment outcomes is early risk assessment and accurate diagnosis, which includes eliminating underlying mental health disorders with similar symptoms. Nurses and providers should remember that environmental factors (such as disruption in the family structure, displacement of the child/family, placement in foster care, parent incarceration, or a parent’s death) can influence treatment. PTSD may be overlooked in these children and in those who are afraid to share information about the trauma or of being exposed to additional trauma, so clinicians need to be well versed about the condition. Care management typically is overseen by a mental health specialist, but an interprofessional approach is essential to promote continuity of care, particularly when a child has been treated for other mental health concerns.
Visit these organizations’ websites to learn more about post-traumatic stress disorder (PTSD) in children and trauma-focused cognitive behavioral therapy (TF-CBT).
- Centers for Disease Control and Prevention: Children’s mental health: Post-traumatic stress disorder in children. Learn about PTSD symptoms, treatment options, and prevention techniques.
- Children Welfare Information Gateway: Trauma-Focused Cognitive Behavioral Therapy: A Primer for Child Welfare Professionals. This downloadable fact sheet about TF-CBT includes information about target populations, key components, benefits, and additional resources.
- Medical University of South Carolina TF-CBT Web 2.0: A course for trauma-focused cognitive behavioral therapy. This web-based training course gives providers who diagnose and treat PTSD an opportunity to learn new skills they can incorporate into their practice.
- Trauma-Focused Cognitive Behavioral Therapy: National Therapist Certification Program. This site offers training and certification for mental health professionals. Visitors also can search for certified therapists by name or region.
- U.S. Department of Veterans Affairs: PTSD: National Center for PTSD. This article provides insights into children’s PTSD risk factors, effects other than PTSD in children who experience trauma, and treatment options.
Kelly J. Betts is an assistant professor at the University of Nebraska Medical Center College of Nursing in Scottsbluff.
References
American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5). Arlington, VA: APA; 2013.
Alisic E, Zalta AK, van Wesel F, et al. Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: Meta-analysis. Br J Psychiatry. 2014;204:335-40.
Chowdhury U, Pancha A. Post-traumatic stress disorder in children and adolescents. Community Pract. 2011;84(12):33-5.
Jensen TK, Holt T, Ormhaug SM. A follow-up study from a multisite, randomized controlled trial for traumatized children receiving TF-CBT. J Abnorm Child Psychol. 2017;45(8):1587-97.
McLaughlin KA, Koenen KC, Hill ED, et al. Trauma exposure and posttraumatic stress disorder in a national sample of adolescents. J Am Acad Child Adolesc Psychiatry. 2013;52(8):815-30.
Tsujii H, Tachibana Y, Okuyama M, Igarashi T. Intervention for post-traumatic stress disorder in children after disaster: A literature review. Int J Child Adolesc Health. 2017;10(1):7-15.


















1 Comment.
Hello! Unfortunately, statistics confirm that many children cannot cope with such things as post-traumatic disorder alone. The main thing in this situation is to recognize in time that the child has problems. We must be attentive to our children and be able to notice changes in their behavior and their fears. PTSD treatment takes a lot of time and effort, but treatment is indispensable. Thanks for great article!