
Interprofessional team takes action to improve care of patients with diabetes.
Takeaways:
- The revision of a hospital’s critical blood glucose value reduces both severe and critical hypoglycemia episodes promoting patient safety.
- Interprofessional team collaboration promotes implementation of evidence based practice for hospitalized patients to improve quality care.
In January 2017, at a 253-bed, semirural hospital, a critical blood glucose value notification wasn’t automatically sent for a blood glucose level of 42 mg/dL. The patient was asymptomatic, and because of the lack of notification, no intervention was taken. Subsequently, the glucose level dropped to 32 mg/dL, and the patient developed serious signs and symptoms of hypoglycemia, which resulted in the need for aggressive management. When the patient’s nurse discussed this incident at a diabetes resource nurse committee (DRNC) meeting, other nurses revealed that they had similar experiences. Lack of notification at an appropriate glucose level not only puts patients at risk but also places undue stress on nurses, who must take emergent action rather than manage a less-serious event. (See Diabetes fast facts.)
Diabetes continues to be a significant healthcare issue in the United States.
- More than 30 million adults and children live with diabetes.
- Approximately every 21 seconds, someone is newly diagnosed with diabetes.
- People with diabetes have a threefold greater risk of hospitalization compared to those without diabetes.
- An estimated 25.7% of hospitalized patients have diabetes.
Hypoglycemic events among hospitalized patients with diabetes place patients at risk for death, neurologic injury, and increased length of stay. When exploring the relationship between hospitalized patients with diabetes and the number and severity of hypoglycemic episodes (blood glucose ≤ 50 mg/dL):
- hypoglycemia is observed in 7.7% of admissions, and the length of stay increases 2.5 days for each day with hypoglycemia
- the odds of inpatient death increases 85.3% with each additional day of hypoglycemia
- the odds of death within 1 year from discharge increase 65.8%.
Financial impact
Hypoglycemia also has a financial impact on patients and organizations. Research considers the social determinant of income and explores the cost of care for hypoglycemic emergency department (ED) visits and hospital admissions.
- The hypoglycemia visit/admission rate is 203.4 per 100,000 people per year among the lower-income population, and 149.6 per 100,000 people per year among the higher-income population.
- The estimated average per person cost of an ED visit for hypoglycemia is $1,965 per person, and the average per person inpatient admission cost is estimated to be as high as $11,632.
- The estimated average per person ED cost for any diagnosis with a secondary diagnosis of type 2 diabetes is $1,979, and the estimated average per person inpatient admission cost is $13,474.
Sources: American Diabetes Association 2019, Basu et al. 2017, Turchin 2009
The organization’s laboratory critical value policy at the time of the event defined a critical blood glucose value as < 40 mg/dL. However, the American Diabetes Association (ADA) standards of medical care in diabetes for critical blood glucose values were updated to < 54 mg/dL in 2017.
The hospital embarked on an interprofessional quality improvement project to review and revise its laboratory critical value policy to comply with current ADA best practices. With the diabetes care specialist serving as a change leader, the hospital enacted a successful process for policy revision and nursing education to support sustainable change for managing critical blood glucose values.
Team
The quality improvement team included nursing, medical, and laboratory members. The certified diabetes care and education specialist (CDCES) (with 23 years of clinical experience) chairs the DRNC, which includes a clinical nurse representative from each nursing unit and a clinical education department representative. The DRNC’s purpose is to provide clinical nurses with diabetes management education and resources to promote optimal patient care. At monthly committee meetings, open lines of communications are maintained so members can safely share information and concerns related to patients with diabetes. The CDCES synthesizes information and identifies appropriate collaboration with other departments to maintain care quality and improve patient outcomes.
In collaboration with the DRNC, the outpatient endocrinologist, and medical director of medicine service line (MDMSL) support open communication between the medical and nursing staff. And the medical director of the laboratory (MDL) maintains policy implementation for lab practice and lab value dissemination.
Intervention
Consistent with the organization’s process for professional development and practice, the CDCES reviewed the best available evidence related to blood glucose values and presented it, along with current organization policy, at the March 2017 DRNC meeting. The evidence identified the need to prevent and control hypoglycemia to reduce patient length of stay and lower mortality during and after hospital admission. Specifically, the evidence pointed to following the ADA standard of defining clinically significant hypoglycemia as blood glucose levels < 54 mg/dL. The DRNC members agreed to revise the critical blood glucose value to < 53 mg/dL, per the MDMSL’s recommendation.
The MDL presented the planned change at the July 2017 medical executive committee (MEC) meeting, but the MEC didn’t accept the plan, possibly because the reason for the change wasn’t clearly explained. The CDCES met with the director of clinical and service excellence (quality), accreditation/patient safety, and clinical documentation improvement to discuss the MEC outcome. The interprofessional team unanimously agreed that a meeting with the outpatient endocrinologist was the next best action to take to ensure patient safety.
In August 2017, the CDCES and the outpatient endocrinologist met and reviewed the revised policy. They decided that the CDCES would resubmit the revised policy to the MEC for reconsideration and request that an opportunity to present it in person. In addition, the CDCES and the MDMSL reviewed the ADA standards of medical care in diabetes and implications of the revised policy. The MDMSL supported both and agreed to attend the next MEC meeting along with the CDCES.
At the November 2017 MEC meeting, the CDCES presented the proposed policy change along with explanations about its importance to nursing care and patient safety. The revised policy was approved. The CDCES then collaborated with the point of care coordinator and laboratory manager to implement the change.
Results
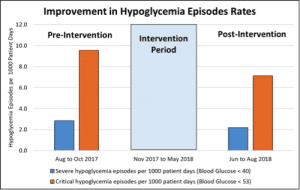
The critical blood glucose value change from < 40 mg/dL to < 53 mg/dL was communicated by DRNC members to their respective units at staff meetings and via email. Communications highlighted the accepted critical blood glucose value and compliance with the ADA standards of medical care in diabetes. The result of the policy change was a reduction in both severe and critical hypoglycemic episodes. (See Project results.)
The interprofessional quality improvement project to revise the critical blood glucose value based on American Diabetes Association standards at a 253-bed semirural hospital resulted in reduced severe and critical hypoglycemic episodes.
Education
Starting in May 2018, the revised laboratory critical value policy practice change was included in the annual nursing skills event at the glucometer skills station. All clinical nurses and certified nursing assistants are required to review the revised policy and demonstrate competency in understanding defined critical blood glucose values and appropriate actions.
Discussion
Interdisciplinary collaboration is crucial for organizational change, and administration commitment allows for successful process improvement. Coordination between the CDCES and staff nurses was the catalyst for this quality improvement project. The culture of open communication at DRNC meetings provides opportunities for staff to share concerns with the CDCES, who follows up and implements best evidence and clinical expertise.
This quality improvement project shows how the role of the CDCES can drive evidence-based practice guideline implementation. Professional communication executed via emails, formal and informal meetings, and conversations promote collaboration. Education through DRNC discussions at staff meetings, implementing education at skills event, and emails supported best practice.
Practice implications
This quality improvement project demonstrates that using the recommended ADA critical value for hypoglycemia promotes earlier detection and reduces hypoglycemic episodes. Other organizations should consider taking similar steps to promote patient safety. This project also demonstrates the impact nurses can have when implementing a strong evidence-based practice process for quality improvement.
Crystal C. Allison is a certified diabetes care and education specialist at Meritus Medical Center in Hagerstown, Maryland.
References
Akirov A, Grossman A, Shochat T, Shimon I. Mortality among hospitalized patients with hypoglycemia: Insulin related and noninsulin related. J Clin Endocrinol Metab. 2017;102(2):416-24.
American Diabetes Association®. Standards of medical care in diabetes. Diabetes Care. 2020;43(suppl 1). care.diabetesjournals.org/content/43/Supplement_1
Bansal V, Mottalib A, Pawar TK, et al. Inpatient diabetes management by specialized diabetes team versus primary service team in non-critical care units: Impact on 30-day readmission rate and hospital cost. BMJ Open Diabetes Res Care. 2018;6(1):e000460.
Basu S, Berkowitz SA, Seligman H. The monthly cycle of hypoglycemia: An observational claims-based study of emergency room visits, hospital admissions, and costs in a commercially insured population. Med Care. 2017;55(7):639-45.
Curkendall SM, Natoli JL, Alexander CM, Nathanson BH, Haidar T, Dubois RW. Economic and clinical impact of inpatient diabetic hypoglycemia. Endocr Pract. 2009;15(4):302-12.
Marathe PH, Gao HX, Close KL. American Diabetes Association standards of medical care in diabetes 2017. J Diabetes. 2017;9(4):320-4.
Turchin A, Matheny ME, Shubina M, Scanlon JV, Greenwood B, Pendergrass ML. Hypoglycemia and clinical outcomes in patients with diabetes hospitalized in the general ward. Diabetes Care. 2009;32(7):1153-7.

















