A look at best practices.
Editor’s note: This is part of our continuing series designed to tackle issues related to how the profession will move forward as the COVID-19 pandemic evolves. Access a virtual roundtable on the topic here.
According to The Future of Nursing 2020–2030: Charting a Path to Achieve Health Equity, the COVID-19 pandemic has revealed and amplified significant gaps in the U.S. healthcare system, including race-related health disparities and lack of access to primary healthcare. However, these problems existed before the pandemic. They’re the outcome of a system that fails to address social determinants of health (SDOH) and health equity.
Benton and colleagues summarized the findings of a survey conducted by the American Nurses Association, the American Organization of Nursing Leaders, and Johnson & Johnson. Over 4,000 nurses were surveyed to determine the impact of COVID-19 on nurses. The data show that even during the double crisis of a global pandemic and a collapsing healthcare system, nurses created innovative solutions and designed process changes. The summary makes the following recommendations for transforming the U.S. healthcare system:
- Identify gaps and appoint nurse leaders today.
- Grow the pipeline of new nurses.
- Embrace nurse-led experimentation within health systems.
- Rethink systems and policies that hinder community-level access to care.
Creating opportunities for innovative thinking and new models of care requires nurses to recognize current gaps and acknowledge the need for transformative redesign.
Identifying gaps
Comparing the U.S. healthcare system to those in other countries can help identify gaps in access, efficiency, and equity and provide insights into how to address them. Knowing the gaps and being knowledgeable about innovative practices will support U.S. nurses as they work to accelerate care transformation.
The Mirror, Mirror reports published by the Commonwealth Fund (the Fund) can help nurses compare global health systems. The Fund synthesizes health system data from three sources: surveys it conducts in 11 high-income nations, data from the Organization for Economic Co-operation and Development, and World Health Organization statistics. The intent is to learn which policies and practices lead to high performance that will move all nations toward optimal and affordable healthcare for all.
The Fund’s ranking is based on five domains: access to care, care process, administrative efficacy, equity, and healthcare outcomes. The ranking in each of these domains drives the final overall ranking of each nation’s healthcare system. In 2021, the overall ranking (from one to 11) is: Norway, Netherlands, Australia, United Kingdom, Germany, New Zealand, Sweden, France, Switzerland, Canada, and the United States.
None of the nations rank high or low in all areas. Even Norway, which ranked first overall, came in 8th in equity and in care process. Despite its shortcomings, the United States ranks 2nd in the care process domain. In general, U.S. health professionals deliver excellent preventive care and safe care. They engage patients and honor their preferences. Compared to the other nations, the United States has higher rates of mammography screening and vaccination for influenza, and more patients talk with their providers about nutrition, smoking, and alcohol use. However, these positive results are experienced only by those with healthcare coverage.
Despite the noteworthy strengths in care process, the United States ranks 11th for access, administrative efficacy, equity, and healthcare outcomes, giving it the overall lowest ranking.
To make matters worse, the United States significantly outspends all the other high-income nations for the worst healthcare outcomes. According to the Fund, in 2021 the United States spent nearly 17% of its gross domestic product on healthcare, which is about twice as much as the average high-income nation. Despite this, the United States has the highest infant mortality rate and the lowest life expectancy. In addition, the U.S. rate of preventable mortality (causes of death that can be prevented by effective public health and primary prevention) is twice as high as the best-performing nation in that category.
It can be shocking to learn that the U.S. healthcare system has so many flaws, but failure to admit system shortcomings contributes to an ineffective and inequitable system. These gaps can be opportunities for redesigning a better post-pandemic system.
Examples of global best practices
Based on the Fund’s findings, high-performing nations share these characteristics, which improve healthcare outcomes and equity:

- Universal healthcare coverage and removal of cost barriers. The United States is one of the few countries not to offer free, universal, or free and universal healthcare.
- Primary care available locally in all communities and for all people
- Reduced administrative burdens for providers and patients
- Investment in services to address SDOH.
A closer examination of global models that exemplify these features can provide insights for redesigning U.S. healthcare. The first two examples are from high-income nations profiled by the Fund, and the third demonstrates that excellent health outcomes depend on a well-designed—not a well-financed—system.
Norway: Universal coverage, cost barrier removal
According to United Nations’ Sustainable Development Goals (SDGs), one of the targets for the third goal (health) is to “achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all.” Norway exemplifies excellence in this domain, and the Fund ranks Norway second in access to care and first overall.
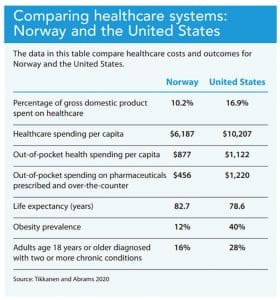
According to the Fund, Norway’s National Insurance Scheme covers 85% of health expenditures. Covered services include primary care, hospital care, mental health treatment, rehabilitation, prescription drugs, preventive care, home and palliative care, medical equipment, and dental care for children and people with chronic diseases and in long-term care. (See Comparing healthcare systems: Norway and the United States.)
Buurtzorg Nederland: Reduced administrative burdens
The Fund ranks the Netherlands second overall. Even though it scored high in access to care, administrative efficiency ranked 8th. One nurse decided to address this issue by redesigning home care. Jos de Blok, a practicing home care nurse became frustrated with excessive layers of bureaucracy, countless administrative tasks, and emphasis on productivity rather than relationships.
Instead of leaving nursing, de Blok returned to the original district model of home nursing and created Buurtzorg (Neighborhood Care). His solution was to create small neighborhood-based teams of nurses who determine the needs of clients and families without additional management layers. He believes that management is the greatest contributing factor to fragmented care and wasted time and resources. According to the Center for Public Impact, Buurtzorg spends only 8% of its budget on administration compared to the 25% Dutch average. This nurse-led model exemplifies the best practice of reduced provider and patient administrative burdens.
In the Buurtzorg model, the home care nurse provides all the care, including intake and assessments, personal care, and complex care. The nurse manages the schedule and maintains records. The nurse also draws upon and coordinates formal and informal networks of support in the neighborhood. This approach solves fragmentation of care, and relationships with the same team of nurses over time yields increased satisfaction for both clients and nurses.
This approach has brought impressive results. According to the Center for Public Impact, client satisfaction rates for Buurtzorg were 30% higher than the national average for other healthcare organizations. Buurtzorg consistently earns the title of best Dutch employer, and the model has financially saved the Dutch healthcare system; Buurtzorg clients use only 40% of the care that they can receive compared to non-Buurtzorg clients who use 70% of services. The Buurtzorg model addresses chronic illness and administration efficiency issues that frequently stymy other healthcare systems.
According to the Fund, bureaucratic tasks in the current U.S. healthcare system have yielded decreased provider and client satisfaction and have needlessly increased costs. The Buurtzorg model doesn’t solve acute care issues, but it may offer a cost-effective solution for preventing many people from advancing to acute care. (Click here to learn more about Buurtzorg.)
Cuba: Free primary care, investment to address SDOH
To dispel the myth that excellent healthcare is delivered only by high-income, global north nations, consider the Cuban healthcare model. Cuba’s system exemplifies primary care that’s available locally in all communities and investment in services that prioritize SDOH.
According to Pineo, a Latin American public health scholar, before the 1959 Cuban revolution, Cuba had only one rural hospital and rural infant mortality rates of 32 per 1,000 live births. Half of adults were illiterate, and two-thirds of the population lived in mud-floor houses without drinking water or electricity.
After the revolution, a new model was developed to deliver primary care throughout the nation. The model draws heavily on primary prevention and consideration of social and environmental determinants of health. Pineo writes: “In Cuba, healthcare, along with education, housing, transportation, and basic necessities, is either free or available at a nominal charge… Cuba practices social medicine, dealing more with the conditions that lead to poor health—nutrition, potable water, sanitation, vaccination, mosquito control—giving less focus to expensive curative treatments… In Cuba, health is regarded as a basic human right, not as a purchasable commodity.”
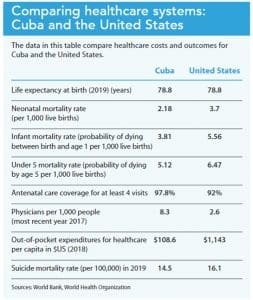
The Cuban model begins with comprehensive family care at the neighborhood level, where citizens receive free primary family medical care at a doctor–nurse clinic. In these clinics, the focus is prevention and individual and population health outcome improvement. The physician and nurse live in the community, frequently in apartments above the clinic. The team also includes a public health expert responsible for mosquito control, drinking water quality management, and sewer system adequacy. Pineo reports that the physician and nurse teams see patients in the clinic in the morning and make home visits in the afternoon, ensuring everyone in the community is seen at least twice a month whether they’re ill or not. (See Comparing healthcare systems: Cuba and the United States.)
Cuba has universal health insurance coverage and offers accessible neighborhood-based primary care for all citizens, but the key to the country’s remarkable outcomes may be that their entire system focuses on health promotion and prevention. It truly is a healthcare model rather than the illness care models seen in the United States and other high-income nations.
Call to action: Accelerate the change
The Fund’s observations about high-performing global healthcare systems and insights from global best practices provide some obvious next steps for nurses eager to accelerate transformation of the U.S. healthcare system.
Nurses must advocate for policy changes that support a national health insurance program to ensure comprehensive healthcare for all. The United States is an outlier. Nations that prioritize healthcare as a right for all citizens enjoy better health outcomes. Evidence from Norway, the Netherlands, and Cuba show that removing cost barriers and investing in prevention and primary care can significantly improve a nation’s health.
Nurses must insist on health equity. The Fund’s ranking of the United States as second in care processes shows that we know how to deliver care. The problem is that optimal care and best practices aren’t available to everyone. Nurses must work for policies that ensure cost-free primary healthcare and preventive care for everyone.
All nurse practitioners (NPs) must be granted authority to practice to the full extent of their education, advanced clinical training, and national certification. The Future of Nursing 2020–2030 report emphasizes that this action will markedly improve access to care, especially in remote and impoverished counties. Full NP practice authority will likely advance health equity.
Nurse-led community care models need further investment and support. Primary care clinics at the neighborhood and community level enhance relationship-based care and advance prevention efforts. The Buurtzorg model demonstrates the positive effects of managing processes locally, and the Cuban model illustrates the benefit of healthcare delivered in the community by providers who live there.
Nursing curriculum must be redesigned to give attention to primary prevention and SDOH. As seen in the Cuban model, health professionals can be educated to advance a healthcare system that focuses on SDOH and emphasizes chronic illness prevention. In The Essentials: Core Competencies for Professional Nursing Education, the American Association of Colleges of Nursing considers SDOH a core nursing concept. The authors dedicated one competency (7.2b) specifically to recognizing the impact of SDOH and health disparities. This competency is an important step forward, but it’s not sufficient for redesigning the healthcare system. All nursing faculty are called to consistently encourage students to address SDOH and primary prevention throughout their nursing education so that it becomes a nursing practice standard.
Every nurse’s responsibility
It is up to every American nurse to ensure that all people have access to, and coverage for, comprehensive healthcare. Nurses have the knowledge and skills to accelerate the transformation of the U.S. healthcare system.
Teddie Potter is a clinical professor, director of planetary health, co-director of the Katharine J. Densford International Center for Nursing Leadership, and coordinator of DNP in Health Innovation and Leadership at the School of Nursing, University of Minnesota in Minneapolis.
References
American Association of Colleges of Nursing. The Essentials: Core Competencies for Professional Nursing Education. April 6, 2021. aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
Benton L, Begley R, Hatmaker D. Look to nurses to help accelerate the transformation of health care. Stat. August 20, 2021. statnews.com/2021/08/20/look-to-nurses-to-help-accelerate-the-transformation-of-health-care
Center for Public Impact. Buurtzorg: Revolutionising home care in the Netherlands. November 15, 2018. centreforpublicimpact.org/case-study/buurtzorg-revolutionising-home-care-netherlands
National Academies of Sciences, Engineering, and Medicine. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. Washington, DC: National Academies Press; 2021.
Pineo R. Cuban public healthcare: A model of success for developing nations. J Dev Soc. 2019;35(1):16-61. doi: 10.1177/0169796X19826731
Schneider EC, Shah A, Doty MM, Tikkanen R, Fields K, Williams II RD. Mirror, mirror 2021: Reflecting poorly: Health care in the U.S. compared to other high-income countries. Commonwealth Fund. August 4, 2021. commonwealthfund.org/publications/fund-reports/2021/aug/mirror-mirror-2021-reflecting-poorly
Tikkanen R, Abrams MK. U.S. health care from a global perspective, 2019. Higher spending worse outcomes? The Commonwealth Fund. January 30, 2020. commonwealthfund.org/publications/issue-briefs/2020/jan/us-health-care-global-perspective-2019
Tikkanen R, Osborn R, Mossialos E, Djordjevic A, Wharton GA. International health care system profiles: Norway. The Commonwealth Fund. June 5, 2020. commonwealthfund.org/international-health-policy-center/countries/norway
Tikkanen R, Osborn R, Mossialos E, Djordjevic A, Wharton GA. International health care system profiles: United States. The Commonwealth Fund. June 5, 2020. commonwealthfund.org/international-health-policy-center/countries/united-states
United Nations. Goal 3: Ensure healthy lives and promote well-being for all at all ages. un.org/sustainabledevelopment/health
World Bank. DataBank: Health nutrition and population statistics. databank.worldbank.org/source/health-nutrition-and-population-statistics
World Health Organization. The global health observatory. who.int/data/gho/data/countries