A quality improvement project aims to provide appropriate and timely care.
- When ambulatory care services can’t meet patient needs, they frequently transfer patients to the emergency department.
- Many of these patients receive minimal intervention before being discharged to home or leave before they’re seen because of long wait times.
- A quality improvement project team proposed creating an advance practice provider ambulatory intermediate care clinic within ambulatory services to address the issue of unnecessary transfers.
When reflecting on the needs of patients using ambulatory care services, it doesn’t take long to realize that their requirements frequently exceed what these settings can offer, which can lead to referrals to an emergency department (ED) for evaluation. At the University of Alabama (UAB) Hospital, provider and patient complaints about this practice resulted in the formation of a quality improvement (QI) project team to assess the issue and find a solution that provides patients with timely access to appropriate care at an acceptable cost and doesn’t add unnecessary volume to the ED.
The back story
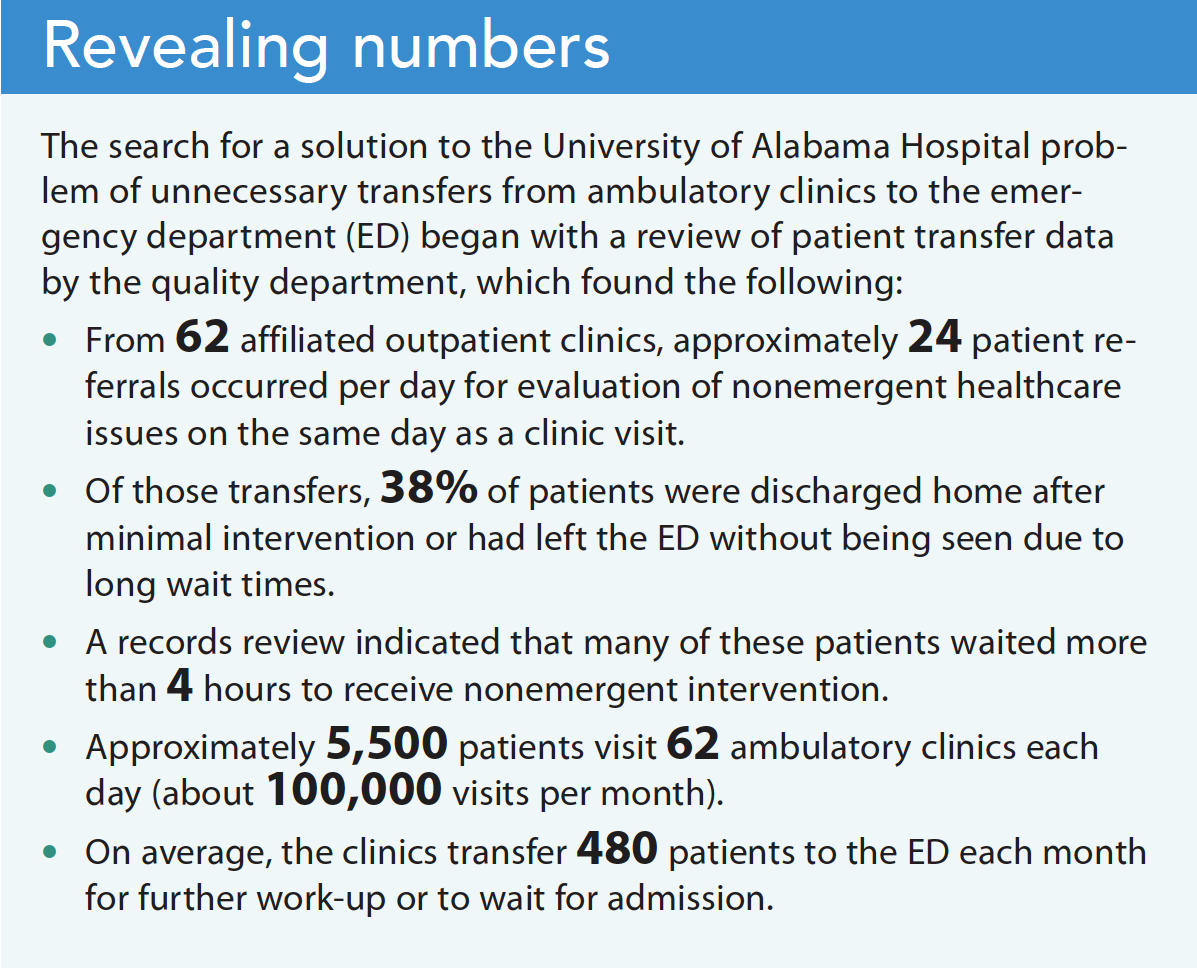
ED overcrowding at UAB Hospital, a longstanding issue, intensified when excess referrals from the clinic exacerbated the problem and resulted in poor patient satisfaction. Initial evaluation indicated that many of these patients were receiving minimal intervention and then being discharged to home, which created an increased cost for patients when compared to the same care in an alternate setting. Developing a plan to move patients to the level of care they needed in a timely manner became a UAB Hospital priority. (See Revealing numbers.)
One of the goals of Healthy People 2030 aims to increase access to comprehensive, high-quality affordable healthcare services. UAB Hospital was unable to provide appropriate access to the level of care required by its own daily patient population. If a patient experienced a healthcare issue on the day of a clinic visit that warranted further evaluation and the issue wasn’t related to the clinic specialty, the patient was sent to the ED. This increase in ED volume created throughput issues and impacted an area where boarding is an ongoing issue.
Research by Allen and colleagues found that with appropriate access to care, up to approximately 50% of all ED visits can be addressed in an outpatient ambulatory setting. They noted that potential cost savings exist when a nonemergent condition is treated in an urgent care center (average cost $156) rather than an ED (average cost $570). An abundance of literature exists related to why patients choose to go to an ED rather than a primary care office, but little research has been conducted to evaluate or understand physician referrals to the ED for minor illness.
UAB Hospital leadership concluded that an alternative to ED transfers could improve access to appropriate care, create a more convenient pathway for patients, and improve health outcomes. The doctor of nursing practice team collaborated with the ambulatory associate vice president to initiate a QI project focused on developing an evidence-based plan to limit the number of nonemergent transfers to the ED from outpatient clinics, decrease the number of patients unable to receive necessary medical care, and reduce the cost of this care for the organization and patients.
What we did
The QI project team included ambulatory senior leadership, nursing administration, and ambulatory quality personnel. Two UAB nursing doctoral students led the QI team. They used a PICOT (patient, intervention, comparison, outcome, time) question and team charter to guide the project. The team identified a list of stakeholders, including ambulatory and inpatient nursing, quality personnel, finance staff, ambulatory providers, and emergency medicine providers. The team then collected and analyzed internal data to identify the number of scheduled clinic patients sent to the ED each day and the reasons for transfer. Next, the team reviewed site data to determine the interventions performed for patients referred from a clinic visit to the ED. Using the information collected, the team worked to find a solution.
Proposed solution
To address unnecessary transfers to the ED, the team proposed an advanced practice provider–ambulatory intermediate care clinic (AICC) within the ambulatory space to which specialty clinics could refer nonemergent patients who require evaluation after a clinic visit. However, development of the AICC space was delayed due to construction constraints. As an alternative, the team worked with inpatient leadership to use an existing inpatient observation unit during a trial phase. After 3 months, the high inpatient demand for the space, which resulted in limited bed availability, led the team to decide that outpatient-driven treatment protocols required a dedicated space within the clinic.
Protocols and guidelines
After internal review board approval and the 3-month pilot, the team developed clinical protocols (based on the three most common nonemergent transfers from outpatient clinics to the ED) for advanced practice RN (APRN) care of patients in the AICC. Patients wouldn’t be allowed to come to this area from home; it would be available only for that day’s scheduled patients. Potential exists for the program to grow as a result of the telemedicine campaign currently underway in the organization, so patients from home may be permitted to come to the intermediate care clinic in the future.
Guideline development focused on determining appropriate healthcare conditions for referral to the AICC. The QI team used the Donabedian model (a framework for evaluating healthcare quality) to guide the process. The model assesses the structure, methods, and outcomes of guideline and protocol development. The team understood the importance of creating strict guidelines to ensure the AICC doesn’t become a dumping ground that delays patients who need higher level care.
Data
To guide protocol development, the team analyzed a 1-month sample of patients transferred to the ED in each quarter for 1 year to identify the most common diagnoses. The three most common diagnoses that could reasonably be managed outside of the ED included hypertension without chest pain, dyspnea, or neurological deficit; nausea, vomiting, or diarrhea; and hyper- or hypokalemia.
Using evidence-based protocols, the QI team, in collaboration with ambulatory administration personnel and physician leadership, developed clinical guidelines for patient treatment in the AICC. A literature review for each diagnosis helped the team create up-to-date, evidence-based treatment guidelines. The target population for the guidelines included emergency medicine providers who treat these types of cases daily and internal medicine providers with direct oversight of the AICC when it opened. The team used the AGREE II instrument (bit.ly/3ibW29R) to assess guideline quality and accuracy. Providers will use the protocols to determine which healthcare conditions meet the criteria for evaluation and treatment and then follow them to guide patient care in the AICC.
An expert panel, selected based on specialty, reviewed the draft guidelines. Clinical experts who expressed an interest in participating in guideline development received a participant information statement and details about the study. The blinded review helped to ensure full disclosure of provider concerns and guideline critique. Each participant viewed a short PowerPoint presentation explaining the problem, internal and external data, and the proposed solution. For the AGREE II protocol evaluation, the QI team received a 50% response rate from the expert panel. After revision based on panelist feedback, the protocols received a second review before the QI project team presented the final product to organizational stakeholders.
The team received encouraging and patient-focused comments from the expert panel. For example, panelists asked about next steps after discovering a potassium abnormality that would deem the patient ineligible to remain in an intermediate care setting and how the APRN would screen for a thoracic aortic dissection in patients with hypertension. A patient flow stakeholder asked how beneficial the plan would be for the ED and whether the numbers justify the intervention.
Challenges
The QI project team faced challenges with regard to available clinic space because of renovations estimated to take about 2 years. Using the observation unit as a temporary alternative had varying levels of success, primarily related to provider comfort level with accepting patients and hospital census. Also, the ED frequently uses the space for overflow and for further evaluation and treatment until a patient can be admitted or stabilized and discharged home.
In addition, because the in-depth protocols require a thorough workup before accepting a transfer to the AICC and some clinic settings have limited testing ability, the team quickly realized that meeting all the criteria for transfer to the observation area presented an issue. In response, the team decided to continue using the observation unit only until a dedicated space could be created in the clinic area.
The protocols used in the AICC will allow for patient workup within the eventual dedicated space because of plans to have access to lab, radiology, and other services. After completing the initial workup, providers can provide treatment and reassessment to determine whether a patient is stable enough to go home, requires continued care, or should be transferred back to the ED. The AICC aims to have 70% of patients discharged home after intervention. Other protocols will be added as needs are identified and other diagnoses are deemed appropriate for care in the AICC.
Next steps
Baxter and colleagues note that the literature supports integrated care as a means to improve patient satisfaction, perceived quality of care, and access. This project and the proposed solution will meet these measures and provide integrated care. The data support the need for a more appropriate level of care for patients, and the expert review endorsed the service. Providing more patient-centric care and reducing ED volume will create a positive impact for the organization and its customers.
More work is required to ensure success after the AICC opens. Next steps include creating a universal guide to improve the decision-making process by which patients are referred to the appropriate level of care, preparing the AICC to open, and continuing protocol development to ensure quality care provided in a timely manner and to decrease the cost of healthcare for patients and the organization.
Diana Dedmon is an assistant professor and director of clinical affairs at the University of Tennessee Health Science Center College of Nursing in Memphis, Tennessee. Lori Mehaffey is director ambulatory services at the University of Alabama (UAB) Hospital. Kimberly Payne is associate vice president of ambulatory services at UAB Hospital. Marisa L. Wilson is UAB School of Nursing faculty chair.
American Nurse Journal. 2023; 18(2). Doi: 10.51256/ANJ022321;
Key words: patient transfers, unnecessary transfers, emergency department, quality improvement
References
Allen L, Cummings JR, Hockenberry JM. The impact of urgent care centers on nonemergent emergency department visits. Health Serv Res. 2021;56(4):721-30. doi:10.1111/
1475-6773.13631
Baxter S, Johnson M, Chambers D, Sutton A, Goyder E, Booth A. The effects of integrated care: A systematic review of UK and international evidence. BMC Health Serv Res. 2018;18(1)350. doi:10.1186/s12913-018-3161-3
Brouwers MC, Kho ME, Browman GP, et al. on behalf of the AGREE Next Steps Consortium. AGREE II: Advancing guideline development, reporting and evaluation in healthcare. CMAJ. 2010;182(18):e839-42. doi:10.1503/cmaj.090449
U.S. Department of Health and Human Services. Healthy People 2030. health.gov/healthypeople


















