
Traumatic brain injury (TBI) refers to blunt or penetrating head injury that disrupts normal brain functioning, causing impaired thinking and memory, personality changes, and possible sensory and motor changes. Some people recover completely with no cognitive deficits; others remain in a persistent vegetative state.
TBI occurs in all age groups, and its incidence is increasing. It contributes to about 30% of all injuryrelated deaths and accounts for about 2.5 million emergency department (ED) visits annually. Although most TBIs cause only mild effects, roughly 290,000 patients are hospitalized for TBI annually; of those, about 51,000 die. However, over the past 3 decades, the overall mortality rate has declined from nearly 50% to approximately 25%.
TBI commonly leads to elevated intracranial pressure (ICP), which can have catastrophic consequences. ICP reflects the pressure of the cranial contents—cerebrospinalfluid (CSF), brain tissue, and blood. The cranial vault is a fixed structure, so it can’t enlarge when its contents expand. The sum of the volumes of brain tissue, CSF, and intracranial blood is constant; if one increases, one or both of the other two must decrease. Space-occupying conditions like tumors, infection, and edema compromise brain tissue when they expand, causing brain structures to alter shape, which can obstruct flow of CSF and blood.
Causes of increased ICP
All nurses need to be able to identify the factors that can increase ICP, which include:
• increased neuronal oxygen consumption from pain, anxiety, agitation, fever, and shivering (which increase metabolic demand)
• environmental light and sound
• bathing
• repositioning in bed
• seizures. Patients should receive seizure prophylaxis within the first week after TBI; however, early posttraumatic seizures aren’t associated with worse outcomes.
ICP monitoring
We now know that not all the neurologic damage from TBI occurs at the time of injury. Some continues over several hours to days, so early recognition and treatment are crucial for optimizing patient outcome.
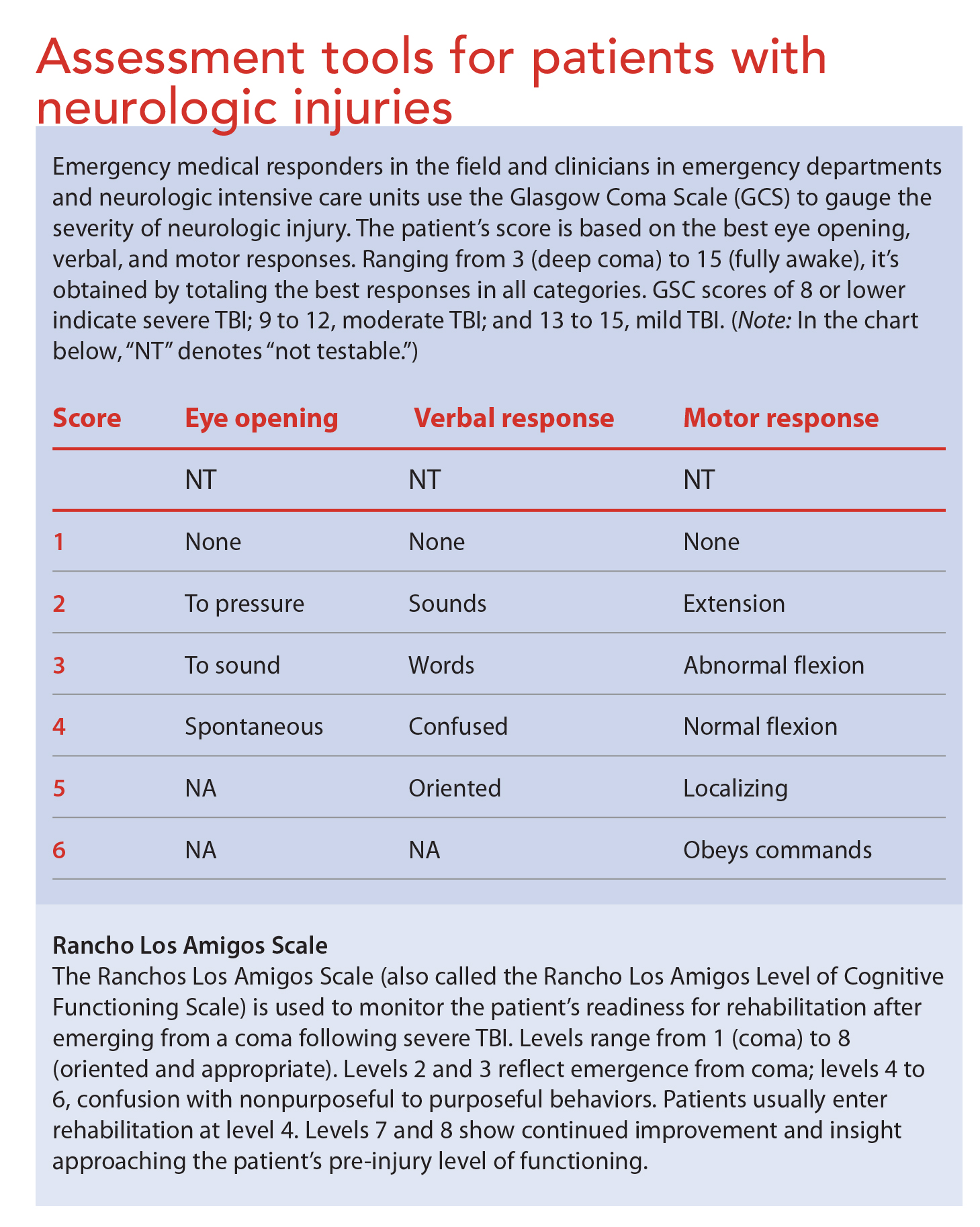
Continuous ICP monitoring allows early identification of increased ICP. Not only does it reveal how the patient responds to routine activities, such as turning, bathing, and suctioning; it also promotes early interventions to treat rising ICP before it climbs dangerously high. The consensus recommendation is to treat ICP above 20 mm Hg. Pupillary changes can occur at ICP as low as 18 mm Hg; herniation, at ICP as low as 20 to 25 mm Hg. (See Assessment tools for patients with neurologic injuries.)
The Brain Trauma Foundation recommends ICP monitoring for all TBI patients who:
• are capable of recovering
• have Glasgow Coma Scale (GCS) scores of 3 to 8
• have abnormal head computed tomography (CT) scans.
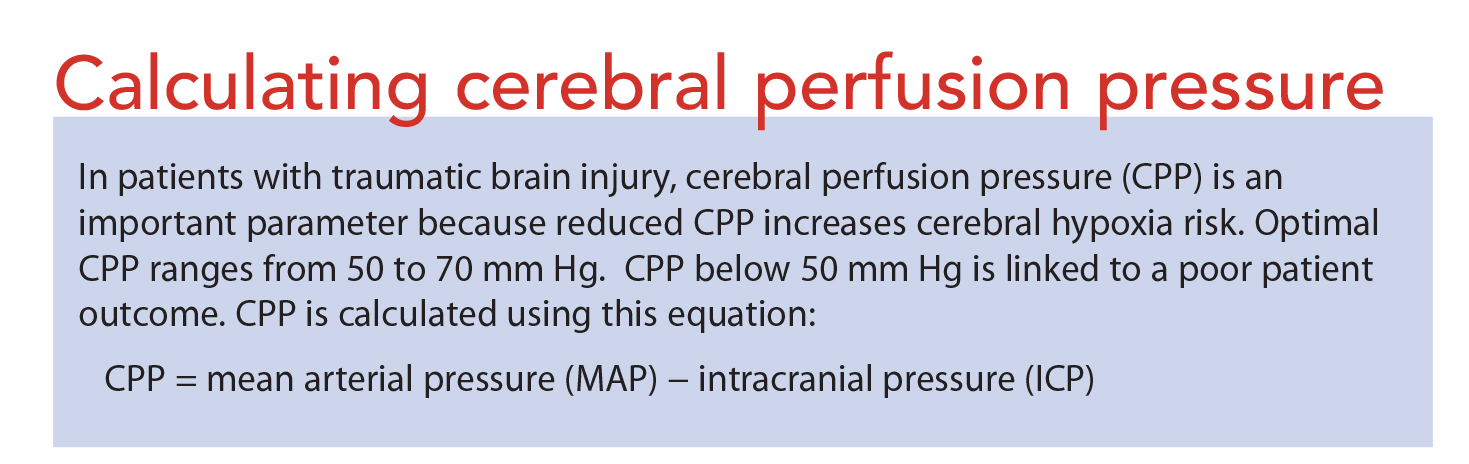
ICP monitoring also is recommended for all severe TBI patients with normal head CT scans who are older than age 40 and show motor posturing (decorticate, decerebrate, or both) and systolic blood pressure below 90 mm Hg. In conjunction with mean arterial blood pressure (MAP) monitoring, ICP monitoring is used to calculate cerebral perfusion pressure (CPP), an indirect measure of cerebral perfusion.
(See Calculating cerebral perfusion pressure.)
Recommended ICP monitoring method
The recommended ICP monitoring method involves placement of an external ventricular drain (EVD) in the lateral ventricle using sterile technique. Typically, this takes place either at the bedside or in the operating room. Advantages of an EVD include reliable ICP monitoring, system recalibration, excess CSF drainage, and intrathecal medication administration.
Alternatively, a parenchymal ICP monitor can be used, although it loses accuracy over time (drift) and can’t be recalibrated after it’s placed in the brain. Also, a parenchymal catheter may not transduce accurate measurements if placed at or near the brain injury site.
Methods for reducing ICP
ICP should be reduced in a stepwise fashion, starting with noninvasive and conservative measures and progressing to other measures as needed. Some interventions may occur simultaneously, depending on the patient’s specific needs and severity of increased ICP.
First steps: Noninvasive and conservative measures
• Elevate the head of the patient’s bed 30 to 45 degrees and ensure venous outflow isn’t obstructed from a kinked neck, constricting tape, or cervical collar.
• Take steps to prevent shivering, which increases ICP.
• Avoid hyperthermia, which can increase metabolic demand as much as 10% per degree C. (Fever is a marker of poor outcome in TBI patients.) Be aware that vasodilation from fever increases CPP, which in turn raises ICP. Increased air circulation blankets, cooling catheters, and antipyretics can be used to decrease fever.
• Take measures to optimize the patient’s blood pressure, avoiding both hypotension and hypertension.
• Know that aggressive fluid resuscitation to drive CPP above 70mm Hg puts patients at risk for acute respiratory distress syndrome. To avoid hypoxia, strive for an oxygen saturation above 90% or a partial pressure of arterial O2 (PaO2 ) above 60 mm Hg.
• Catecholamine stress response in TBI patients can lead to hyperglycemia, which typically warrants supplemental insulin. Untreated hyperglycemia (blood glucose level above 200 mg/dL) is associated with worse neurologic outcomes. Prolonged hypoglycemia also is dangerous because it can reduce the brain’s glucose supply, leading to neurologic deterioration. Experts recommend starting blood glucose monitoring at admission and striving for normoglycemic status. The American College of Surgeons recommends a blood glucose range between 80 and 180 mg/dL. However, optimal hyperglycemia treatment in severe TBI remains controversial.
Second steps: Pharmacologic interventions
If the patient’s increased ICP doesn’t respond to first steps, pharmacologic interventions are added.
• To optimize blood pressure and improve cerebral perfusion, the patient may require vasopressors and I.V. fluid boluses to keep systolic pressure above 90 mm Hg. Stay alert for side effects; depending on the agent used to support blood pressure, the patient may experience tachycardia, peripheral vasoconstriction, arrhythmias, platelet inhibition, hyperglycemia, thrombocytopenia, and increased myocardial demand.
• After TBI, patients may have a stress response marked by hypertension, which may warrant antihypertensive agents. Clinicians should choose agents with the least possible impact on ICP. Be aware that such antihypertensives as nitroglycerin, nitroprusside, and nicardipine can cause side effects that increase ICP— namely, orthostatic hypotension, dizziness, nausea, vomiting, headache, reflex tachycardia, preferential peripheral vasodilation before cerebral vasodilation, thiocyanate toxicity, and platelet dysfunction.
• As needed and ordered, provide interventions for pain, anxiety, and seizures.
• To monitor for nonconvulsive seizures, the physician may consider continuous electroencephalography if ICP rises inexplicably. If ICP remains elevated after antiseizure measures, the patient may require some of the interventions described next.
Third steps: Continuous sedation
If elevated ICP persists despite conservative and pharmacologic measures, continuous sedation may be tried; this technique may reduce ICP by eliminating agitation and pain.
• Opioids or benzodiazepines may be used for sedation; agitated patients also may receive hypnotic or paralytic agents. These drugs may be given individually or in combination. To minimize hypotensive side effects, ensure the patient has normal fluid volume and use smaller doses of opioids, benzodiazepines, or hypnotics, as ordered.
• Paralytics may be given if posturing and agitation increase ICP. Know that if the patient is paralyzed and sedated, a neurologic exam may be difficult or impossible to conduct; you won’t be able to assess mental status, sensation, or movement or obtain a GCS score. Instead, monitor pupillary response and ICP for changes.
• Serial head CT scans may reveal evolving or resolving abnormalities, such as bleeding or swelling.
• The EVD may be used to drain off 3 to 5 mL of CSF.
Fourth steps: Barbiturates, osmotics, hyperventilation, therapeutic hypothermia, and surgery
Patients with refractory ICP elevation may require the additional interventions below.
• Barbiturates. These drugs reduce cerebral metabolic demand and blood flow, providing cerebral protection. The most commonly used barbiturate is pentobarbital. If ICP doesn’t decrease within the first 4 hours after this drug is given, it’s unlikely to lower ICP unless given in combination with other drugs. Know that patients on barbiturates won’t have a pupillary response, so you’ll need to rely on ICP monitoring for evidence of brain herniation. Keep in mind that early changes in pupillary response may indicate early herniation.
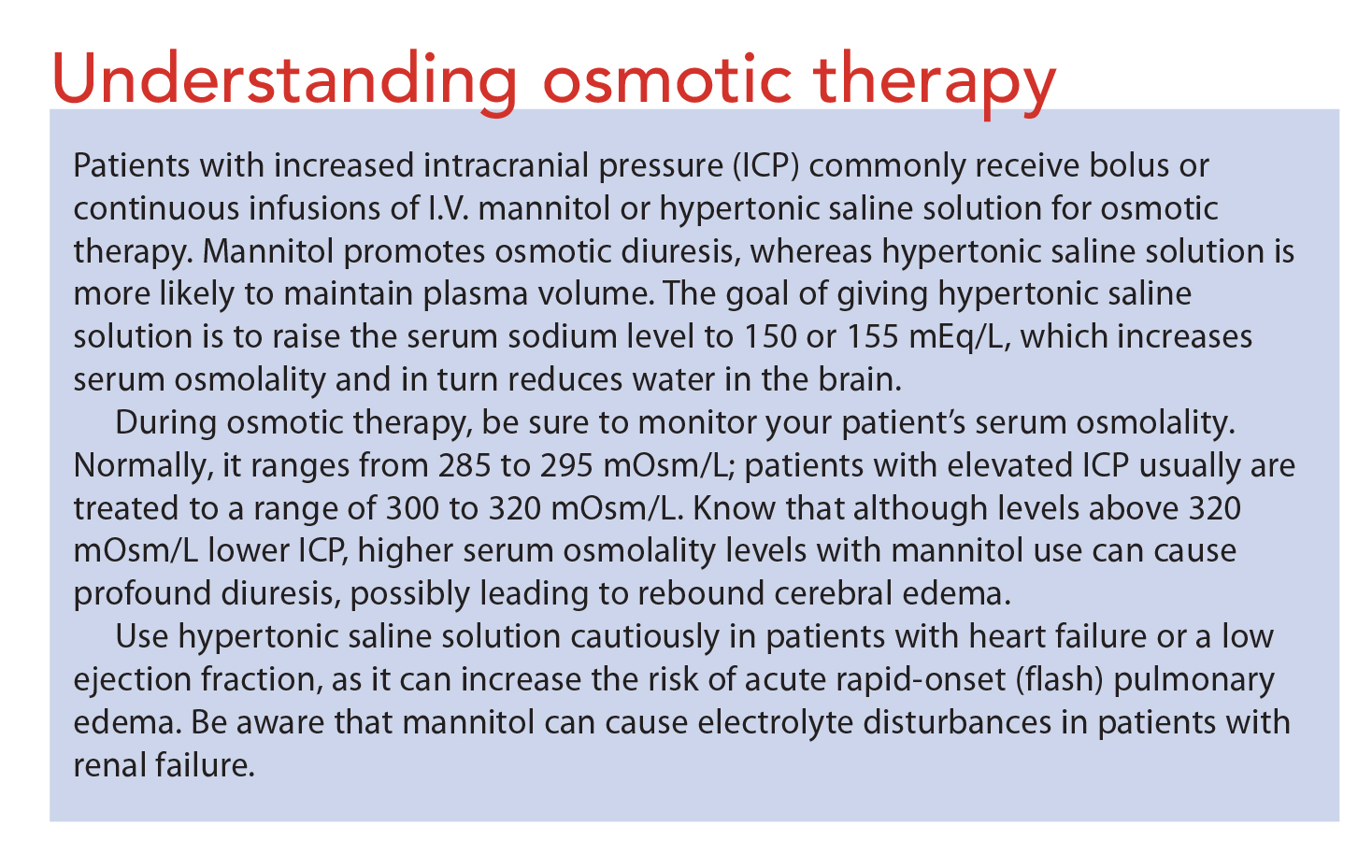
• Osmotics. For patients with persistently elevated ICP, osmotic therapy may be used to expand blood volume by shifting fluid from the brain’s extracellular to intravascular spaces. Osmotics also reduce blood viscosity, which raises CPP and lowers ICP. (See Understanding osmotic therapy.)
• Hyperventilation. The goal of hyperventilation is to reduce PaCO2 , a potent cerebrovascular vasodilator that increases ICP. Hyperventilation reduces ICP by lowering PaCO2 , which causes vasoconstriction. The respiratory therapist induces hyperventilation by adjusting ventilator settings as ordered and monitoring arterial blood gases (ABGs). Usually, PaCO2 should be decreased no lower than 30 mm Hg. However, in patients with refractory increased ICP (above 20 mm Hg), hyperventilation may be used to reduce PaCO2 from 35 to 29 mm Hg, which typically lowers ICP 25% to 35%.
Hyperventilation isn’t recommended as first-line therapy because it leads to cerebral vasoconstriction at a time when cerebral blood flow already is reduced. It’s used intermittently and only for several minutes at a time—and never when ICP is within normal limits or as continuous therapy. It must be avoided during the first 24 hours after injury because it can further compromise cerebral perfusion. It shouldn’t be used as preventive therapy.
• Therapeutic hypothermia. This technique has been shown to reduce ICP but not to consistently improve outcomes. Limiting cooling to less than 48 hours can minimize complications, such as cardiac dysfunction and abnormal O2 delivery. Although cooling protocols vary, body temperature shouldn’t be decreased below 89.6° to 91.4° F (32° to 33° C).
• Surgical options. Surgery may reduce ICP by allowing the brain to swell. Craniectomy removes a large section of bone, which is stored for later replacement. But such decompressive surgery is controversial: Although it lowers ICP, it doesn’t change overall mortality. Also, some experts speculate that axonal stretch and altered cerebral blood flow may cause neural injury in craniectomy patients.
Timing of surgical intervention may vary. A TBI patient with an expanding hematoma that’s causing brain herniation is likely to undergo surgical decompression as soon as possible after arriving at the ED. If the patient doesn’t have a hema toma or evidence of cerebral edema, clinicians may decide to monitor ICP and try conservative measures first. Preexisting illness, age, and patient wishes also should be considered before surgical intervention.
TBI case study
The following case study illustrates the possible course of a hospital stay for a patient with TBI.
Anna S, age 17, experiences seizures and loss of consciousness after suffering head trauma in a sports injury. In the field, emergency medical technicians determine her initial GCS score is 3 (eye opening 1, verbal response 1, motor response 1), which warrants intubation. They transport her to the ED, where an initial head CT shows areas of hemorrhage. Subsequent magnetic resonance imaging confirms diffuse axonal injury.
Here’s a summary of Anna’s condition and medical care during her 4-week hospitalization:
Day 1: A parenchymal catheter is placed for ICP monitoring. Anna’s ICP is 10 mm Hg.
Day 4: Anna’s ICP increases intermittently up to 30 mm Hg. The physician orders sedation and intermittent boluses of hypertonic saline solution.
Day 5: Anna’s temperature rises to 104° F (40° C). A cooling catheter is placed to keep her temperature at 98.6° F (37° C). When her ICP monitor wire fails, the parenchymal catheter is removed and an EVD is placed for continued ICP monitoring and CSF drainage.
Day 14: Anna opens her eyes spontaneously and looks around.
Day 16: Anna is extubated; she responds purposefully to noxious stimulation.
Day 18: Anna’s GCS score is 10 (eye opening 4, verbal response 1, motor response 5). Her Rancho Los Amigos Scale score is 2 with emerging 3, as she begins to wake up and respond to her environment. Her ICP drops below 10 mm Hg and her EVD is discontinued.
Day 25: Anna is able to follow commands, converse, and eat. Her Rancho Los Amigos Scale score is 4.
Day 28: Anna is discharged to a rehabilitation facility for patients with brain injury.
Team approach to TBI
Managing increased ICP in patients with TBI calls for a team approach to optimize outcomes. Bedside nurses are better positioned than other clinicians to identify rising ICP early to ensure appropriate interventions.
Use your critical thinking skills and start conservative measures while anticipating next steps during communication with care providers.
Cindy L. Zerfoss is a neuroscience acute care nurse practitioner at Centra-Lynchburg General Hospital in Lynchburg, Virginia.
Selected references
Abdelhak, T, Abrego GC. Traumatic brain injury. In: Wartenberg KE, Shukri K, Abdelhak T, eds. Neurointensive Care: A Clinical Guide to Patient Safety. New York, NY: Springer; 2015:219-48.
American College of Surgeons. Trauma Quality Improvement Program. Best practices in the Management of Traumatic Brain Injury. 2015.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons; Joint Section on Neurotrauma and Critical Care, AANS/CNS; Bratton SL, Chestnut RM, Ghajar J. Guidelines for the management of severe traumatic brain injury. Antiseizure prophylaxis. J Neurotrauma. 2007;24(Suppl 1):S83-8.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons; Joint Section on Neurotrauma and Critical Care, AANS/CNS; Bratton SL, Chestnut RM, Ghajar J. Guidelines for the management of severe traumatic brain injury. Hyperosmolar therapy. J Neurotrauma. 2007;24(Suppl 1):S14-20.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons; Joint Section on Neurotrauma and Critical Care, AANS/CNS; Bratton SL, Chestnut RM, Ghajar J, et al. VI. Guidelines for the management of severe traumatic brain injury. Indications for intracranial pressure monitoring. J Neurotrauma. 2007;24(Suppl 1):S37-44.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons: Joint Section on Neurotrauma and Critical Care, AANS/CNS; Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury. Intracranial pressure treatment thresholds. J Neurotrauma. 2007;24(Suppl 1):S55-8.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurology Surgeons; Joint Section on Neurotrauma and Critical Care, AANS/CSN; Carney NA, Ghajar J. Guidelines for the management of severe traumatic brain injury. Introduction. J Neurotrauma. 2007;24(Suppl 1): S1-2.
Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons; Joint Section on Neurotrauma and Critical Care, AANS/CNS; Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury. Recommendations for intracranial pressure monitoring technology. J Neurotrauma. 2007;24(Suppl 1):S45-54.
Centers for Disease Control and Prevention. TBI: Get the Facts. 2016.
Cooper DJ, Rosenfeld JV, Murray L, et al. DECRA Trial Investigators; Australian and New Zealand Intensive Care Society Clinical Trials Group. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med. 2011;364(16):1493-502.
Cramer D, Miulli D, Siddiqi J. Cerebral protective measures. In: Siddiqi J, ed. Neurosurgical Intensive Care: The Essentials. New York, NY: Thiemes Medical Publishers; 2008:228-36.
Greenberg MS. Handbook of Neurosurgery. 7th ed. New York, NY: Thieme Medical Publishers; 2010.
Haddad, SH, Arabi YM. Critical care management of severe traumatic brain injury in adults. Scand J Trauma Resusc Emerg Med. 2012;20:12.
Le Roux P, Menon DK, Citerio G, et al. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Neurocrit Care. 2014;21(Suppl 2):S1-26.
Qandah N, Houck EA, Miulli, D. Neuropharmacology. In: Siddiqi J, ed. Neurosurgical Intensive Care: The Essentials. New York, NY: Thieme Medical Publishers; 2008:239-66.
Society of Critical Care Medicine. Fundamental Critical Care Support. 5th ed. Mount Prospect, IL: Society of Critical Care Medicine; 2012.
Teasdale G, Allan D, Brennan P, et al. Forty years on: updating the Glasgow Coma Scale. Nurs Times. 2014;110:(42):12-6.
Teasdale, G, Maas A, Lecky F, et al. The Glasgow Coma Scale at 40 years: standing the test of time. Lancet. 2014;13(8):844-54.

















{kind=link}
{kind=link}
{kind=link}
2 Comments.
I enjoyed reading you post. I am sharing it with my other friends as the information is really very useful. Keep sharing your excellent work.
please forgive me if this is a repeat — but, thanks a lot for this very interesting article. I had worked in a Neuro ICU during nursing school, so I was able to get into the unit where these patients would be cared for, and I needed to transcribe the orders — so I needed to learn more deeply than what we’d had in our 2yr program — but this article so easily helped me get back to that knowledge level. And it’s amazing the changes that have taken place too !!