How one hospital used lean methodology coupled with evidence-based practice to update nursing care.
Takeaways:
- Healthcare organizations must strive to update policies to reflect the most current updated standard of practice from the Infusion Nurses Society and rotate peripheral IVs (PIVs) upon clinical indication as opposed to a routine frequency
- Rotating PIVs upon clinical indication has many benefits, including avoiding unneeded needled sticks, promoting vessel preservation, and saving time.
- Clinical nurses who are empowered to own their practice can make substantial evidence-based changes that improve outcomes.
Peripheral IV (PIV) assessment and care is an important component in clinical nursing. Organizations must ensure that nursing practice policies regarding the use and care of PIVs are updated according to the best available evidence. After reviewing guidelines from the Infusion Nurses Society (INS) about the frequency of rotating PIVs, nurses at Salem Health formed an interprofessional team and used lean methodology, in conjunction with evidence-based practice (EBP), to align nursing practice with the updated national standards. The lean culture prompted our nurses to close the gap between what should be happening and what is actually happening when it comes to PIV rotation.
 Preparing for change
Preparing for change
 Preparing for change
Preparing for changeIn 2015, a clinical nurse from one of our critical care units attended the American Association of Critical-Care Nurses’ National Teaching Institute (NTI). While in a conference session, she learned that the INS had updated their standards of practice for changing PIVs based on results from a Cochrane Database systematic review. The new standard recommended changing PIVs only when clinically indicated, as opposed to rotating based on a routine frequency. However, our organization’s policy, “Peripheral I.V. assessment & care,” still required that RNs change PIV cannulas every 72 to 96 hours.
Getting things moving
After returning from NTI, the nurse conducted a literature search to find the Cochrane review presented at the conference. In her search, she uncovered other original research studies, as well as the INS standards. The 2011 INS Standards of Practice stated, “The nurse should consider replacement of the short peripheral catheter when clinically indicated…[t]he decision to replace the short peripheral catheter should be based on assessment of the patient’s condition.” The 2015 Cochrane review, which included seven trials of 4,895 patients, concluded that “No difference in phlebitis rates was found whether catheters were changed according to clinical indications or routinely.” The INS’s recommendation was validated in its 2016 Policies and Procedures for Infusion Therapy: “A vascular access device (VAD) is removed on the order of a licensed independent practitioner (LIP) when therapy is completed, when clinically indicated, or when deemed no longer necessary for the plan of care.” The INS does not base removal on a specified timeline.
The nurse presented a summary of these findings in the form of an evidence synthesis table, along with associated proposed policy updates, to the EBP and Practice Councils at Salem Health. After receiving support from these councils and nursing administration, the nurse proceeded to establish an interprofessional team (including the nurse proposing the change, nurse manager, clinical nurse specialist, Kaizen clinical nurse consultant, I.V. therapy nurse, other clinical representatives, and a student intern) to formulate an intervention to address the problem. The neuro-trauma care unit (NTCU) volunteered to serve as the pilot unit.
The purpose of the initiative was to align I.V.practices with best practice recommendations that reduce the use of I.V. therapy resources and decrease RN workload and required equipment without negatively impacting the patient experience with an increased incidence of phlebitis.
Educating staff
The interprofessional team used lean methodology and initiated four-step problem-solving. Baseline data were collected on the NTCU to determine the total number of I.V. restarts performed per protocol in 1 month, as well as phlebitis incidence. The team developed a test of change (TOC) where nurses would rotate PIVs based only on clinical indication. This meant that instead of automatically removing a PIV when the 96-hour deadline was near, nurses would leave the current I.V. in place as long as signs of phlebitis, infiltration, or extravasation were absent.
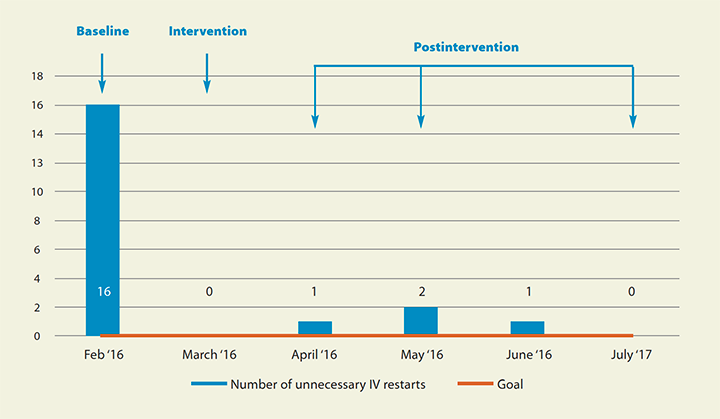
Before starting the TOC, the infection prevention department was consulted to ensure optimal patient safety. NTCU staff were educated on the new process and signs and symptoms of phlebitis, infiltration, and extravasation. In addition, the NTCU resource nurses and leaders of the unit’s specialty practice team disseminated education about the TOC. If a PIV was left in because of the TOC, nurses documented this action in the electronic health record. The NTCU was the only unit participating in the TOC, so if a patient was to be transferred and had a PIV dwell time of greater than 96 hours, a new PIV was started before transfer. (See Unnecessary PIV restarts.)
Unnecessary PIV restartsThe test of change resulted in a successful decrease in the number of peripheral IVs (PIVs) unnecessarily restarted.
|
Reviewing the change
At the end of the 3-month (March to May) TOC, NTCU nurses were surveyed about their perception of the practice change. Results indicated that NTCU RNs believed the TOC improved the patient experience and also saved clinical nurse and I.V. therapy staff time. Before the TOC, nurses frequently paged I.V. therapy staff when they weren’t successful with PIV restarts. In addition, patients no longer had to with stand unneeded needlesticks and vessel preservation was promoted.
A business intelligence report was created from the electronic health record to accurately collect TOC data. Results showed no negative outcomes during the intervention, including no increase in phlebitis rates. During the TOC, 137 PIVs had dwell times greater than 96 hours on the NTCU. Estimated cost savings from the reduced supply usage and RN labor were $435 per month, with an annualized savings of $5,737.44 for a 30-bed critical care unit.
Moving forward
The project team shared the TOC results with Salem Health’s policy stakeholders. The housewide policy was updated to reflect current evidence and went live in August 2016. The Practice Council created a tip sheet that was distributed to nursing units to provide education, and the updated policy was shared in unit announcements, at shift changes, and via e-mail.
After implementing the change, the team presented a follow-up project summary to the EBP Council. The lead nurse presented poster sessions at the Greater Portland Chapter-AACN Critical Care Symposium in November 2016, at the American Nurses Credentialing Center’s National Magnet Conference® in October 2017, and the American Nurses Association’s Quality and Innovation Conference in March 2018.
Impact
Our critical care nurse colleague learned about new evidence that could shape nursing practice and dedicated herself to bringing this new knowledge back to her colleagues. She served as a transformational leader, planting the seed and inspiring other nurses to be champions of the change to improve patient, nursing, and organizational outcomes.
Ellie Barnhart is a clinical nurse on the intermediate care unit at Salem Health in Salem, Oregon. Ann Alway is a critical care CNS at Salem Health Hospitals and Clinics in Salem, Oregon. Margo Halm is the associate chief nurse executive for nursing research and evidence-based practice at VA Portland Healthcare System in Portland, Oregon.
Selected references
Infusion Nurses Society. Policies & Procedures for Infusion Therapy. 5th ed. Norwood, MA; Infusion Nurses Society: 2016.
Infusion Nurses Society. Infusion therapy standards of practice. Sitecare and maintenance. J Infus Nurs. 2011;34(suppl 1):S55-64.
Gorski LA, Hallock D, Kuehn SC, Morris P, Russell JM, Skala LC. Recommendations for frequency of assessment of the short peripheral catheter site. J Infus Nurs. 2012;35(5):290-2.
Morrison K, Holt KE. The effectiveness of clinically indicated replacement of peripheral intravenous catheters: An evidence review with implications for clinical practice. Worldviews Evid Based Nurs. 2015;12(4):187-98.
Rickard CM, Webster J, Wallis MC, et al. Routine versus clinically indicated replacement of peripheral intravenous catheters: A randomised controlled equivalence trial. Lancet. 2012;380(9847):1066-74.
Webster J, Osborne S, Rickard CM, New K. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev. 2015;(8):CD007798.
ant1-Magnet Stories-103


















1 Comment.
Amazing, informative, and inspiring article! Congratulations to the NTCU staff/team on the successful and ongoing motivation and determination of evidence-based practice to improve short peripheral catheter care, quality patient care, and optimal outcomes for patients, nursing staff, organizations and healthcare.
This article is very relevant for me as a current DNP learner with a passion for serving patients by providing best care supported and strengthened by evidence-based research. This article is an inspiring example of commitment to action and change. Short peripheral catheter care and related concerns, issues, management, and complications underscores my dedication now and in the future. THANK YOU!