Identification and treatment
- A case study discusses the prevalence of sepsis and the impact it has on patients and healthcare.
- Successful outcomes require fast sepsis recognition and initiation of treatment within 1 hour.
- Nurse knowledge of changes in the sepsis guidelines and current recommendations as well as patient education and post-discharge management help ensure appropriate care.
Learning Objectives
- Define sepsis patient presentation and risk factors.
- Describe risk factors associated with sepsis.
- Identify treatment for sepsis, in particular Hour-1 priority treatments.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 5/1/28
Sepsis navigators and hospital outcomes
Pediatric sepsis: Are you ready?
Mr. Randall Martin*, age 42, arrives in the emergency department (ED) with his wife. He tells the triage nurse that he hasn’t been feeling like himself lately. Mr. Martin explains that 3 days ago he stepped on an old nail, which penetrated his work boot and punctured his left foot. He easily removed the nail and didn’t think he needed medical attention because he received a tetanus booster last year. When the nurse assesses the left foot, she finds it tender, cool, and edematous, with erythematous and mottling, which appears to be advancing to the ankle. The nurse notes +2 pulses in both lower extremities with capillary refill <2 seconds.
Although awake, alert, and oriented to person and place, Mr. Martin has difficulty answering questions. His wife helps with the patient interview.
The patient’s vital signs are temperature 101.5° F (38.6° C), heart rate 105 beats per minute, respiration rate 24 breaths per minute, blood pressure (BP) 89/44 mmHg (mean arterial pressure [MAP] 59 mmHg), and SpO2 91% on room air. The ED provider prescribes 650 mg of acetaminophen by mouth for fever and orders a serum lactate level, prothrombin time (PT), partial thromboplastin time (PTT), international normalized ratio (INR), basic metabolic panel, and complete blood cell count and differential. In addition, the provider orders two sets of blood cultures using aerobic and anaerobic bottles and a wound culture. The ED nurse cleans the wound and applies a bandage.
Mr. Martin doesn’t remember the last time he urinated. The nurse places an I.V. catheter with maintenance fluids infusing at 100 mL/hour as ordered.
Mr. Martin exhibits signs and symptoms of a systemic infection, including tachycardia, fever, tachypnea, mottling, altered mental status, hypotension, and suspected oliguria. The ED provider identifies sepsis and admits the patient to the intensive care unit (ICU) for further evaluation and treatment. (See Sepsis: Info of note.)
Sepsis: Info of note
In 2017, the World Health Organization declared sepsis a global health priority.
- According to the Centers for Disease Control and Prevention, approximately 1.7 million cases of adult sepsis hospitalizations occur in the United States each year.
- Of these, about 350,000 patients either die or require hospice care, leading to new disabilities, morbidity, and an inability to return to work.
- Sepsis can result from almost any infection, including COVID-19, influenza, and respiratory syncytial virus.
- Most adult patients with sepsis (87%) arrive to the hospital with an ongoing infection.
Defining sepsis
Sepsis, a medical emergency, results from a dysregulated response of the body to infection as evidenced by organ dysfunction and infection. The condition ranges in severity from infection to septic shock, which causes abnormalities throughout the body. Patients receive a diagnosis of septic shock when they meet the criteria for sepsis, can’t maintain a MAP of at least 65 mmHg despite fluid resuscitation, and require vasopressors. Patients with a lactate level greater than 2 mmol/L (or 18 mg/dL) also are considered to have septic shock. In severe cases, sepsis can cause multiple organ dysfunction syndrome, resulting in death.
However, the precise definition of sepsis has evolved. Recently, the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM) provided updated definitions based on expert opinion. The definition of sepsis has shifted from a physiologic derangement (Sepsis-1 and Sepsis-2) to organ dysfunction (Sepsis-3). The Third International Consensus provided definitions for sepsis and septic shock (Sepsis-3).
Tools to identify sepsis early have proved difficult to establish; they each have advantages and disadvantages. For example, some current tools no longer consider systemic inflammatory response syndrome (SIRS) in the definition as it can result from factors other than infection. The 2021 guidelines advise against using the quick Sepsis Related Failure Assessment (qSOFA) alone as a screening tool; however, a study by Neviere and colleagues showed that patients who meet the qSOFA criteria have a higher mortality rate than those who don’t. Other studies recommend using the National Early Warning Score or SIRS score because they have better sensitivity in predicting patient outcomes than qSOFA.
The term “severe sepsis,” which Sepsis-2 defines as sepsis with organ dysfunction, is no longer used. The Sepsis-3 definitions reflect this change. However, the new definitions haven’t been universally accepted. For example, the Centers for Medicare and Medicaid Services (CMS) still support Sepsis-2 (SIRS, sepsis, severe sepsis, and septic shock). Infections may progress to sepsis (or severe sepsis), so prevention requires monitoring patients suspected of having the condition.
The 2016 SCCM/ESICM task force defined organ dysfunction as an increase of two or more points in the Sequential Organ Failure Assessment (SOFA) Score. The SOFA score serves as a prognostic tool based on organ dysfunction; it’s not a sepsis diagnostic tool. Providers should use it to identify patients at high risk of dying from infection. Lactate levels, capillary refill, and patient presentation offer an additional measure of perfusion, and patients who require intensive care should be admitted to the ICU within 6 hours of diagnosis. Primarily, providers base the diagnosis on clinical suspicion, which relies on the signs and symptoms of an infection, diagnostic tests, and treatment response.
Risk factors
The risk factors for sepsis include age (≥65 years), ICU admission, hospitalization, bacteremia, immunosuppression, cancer, diabetes, obesity, and pneumonia. Identifying a patient’s risk factors can aid monitoring and improve outcomes. (See Know the risks.)
Know the risks
Knowing the risk factors for sepsis can aid early identification.
Age (≥65 years)
Sepsis occurs more frequently in older adult patients. Advanced age also serves as a predictor for sepsis mortality. Death from sepsis among these individuals tends to occur early in the disease process. Most of those who survive require placement in a long-term care facility after hospitalization.
Diabetes and obesity
Obesity and type 2 diabetes can increase the risk of sepsis by altering the immune system. Both conditions are associated with a higher likelihood of infections that can lead to sepsis. In the intensive care unit (ICU), patients with obesity may have a higher risk of infectious complications and increased mortality rates.
Hospitalizations and bacteremia
An association exists between previous hospitalization and increased sepsis risk. Patients admitted to the hospital with an infection and those who develop an infection during hospitalization increase their risk. Patients with bacteremia frequently develop systemic effects of infection, which can progress to sepsis.
ICU admission
Patients in the ICU have a high incidence of hospital-acquired infection, which increases their risk for sepsis.
Immunosuppression and cancer
Immunosuppressant medications and cancer (along with its comorbidities) place patients at risk for sepsis or septic shock.
Pneumonia
Community-acquired pneumonia and hospital-acquired pneumonia (ventilator and nonventilator associated) can lead to sepsis.
Sources: Neviere, et al 2025, Giuliano and Baker 2020
Signs and symptoms
Most patients with a confirmed diagnosis or a suspected case of sepsis have a low BP and rapid heart rate. They also may have a fever. Some patients experience hypothermia or hyperthermia. However, research indicates a high risk of mortality among patients with normothermia. Other findings include a high or low white blood cell count. As the condition worsens, signs of shock and organ dysfunction may develop. However, it’s important to note that the signs and symptoms of sepsis aren’t specific; they may appear similar to other medical conditions. (See What to look for.)
What to look for
The following signs and symptoms may indicate sepsis or septic shock.
Blood pressure
Systolic blood pressure <90 mmHg, mean arterial pressure <70 mmHg, and systolic blood pressure decrease >40 mmHg (or less than two standard deviations below normal for the patients age) may indicate sepsis.
End-organ perfusion
Warm, flushed skin can occur in the early phases of sepsis. Cool skin may indicate redirection of blood flow to core organs. Decreased capillary refill, cyanosis or mottling, altered mental status, oliguria or anuria, and ileus or absent bowel sounds serve as signs of end-stage hypoperfusion.
Heart rate
Tachycardia >90 beats/min or more than two standard deviations above the normal value for the patients age may be a sign of sepsis.
Infection
Signs and symptoms specific to an infectious source should raise suspicion for sepsis. Leukocytosis or leukopenia may be present.
Respiratory rate
Tachypnea >20 breaths/minute serves as a sepsis sign.
Temperature
Temperature >100.9F (>38.3C) or <96.8F (<36C) may indicate sepsis. However, some patients with sepsis are normothermic.
Sources: Neviere et al 2025, Singer et al 2016
Diagnosis
Providers frequently make sepsis and septic shock diagnoses based on patient presentation or when diagnostic tests result in positive blood, sputum, or urine cultures, or when the patient responds to antibiotics and treatment. Although it’s preferable to identify the organism responsible, this may not be possible if a patient received antibiotics before obtaining cultures.
Originally, the Surviving Sepsis Campaign (SSC) established 6-hour and 24-hour bundles, which transitioned to 3-hour and 6-hour bundles. These bundles outline what care providers should deliver to patients with sepsis within these designated times from initial presentation. In 2018, the Surviving Sepsis Campaign Hour-1 Bundle of Care emphasized the importance of taking prompt action. Providers should initiate (not complete) this care within 1 hour of identifying criteria for sepsis and from the earliest charted finding consistent with all elements of sepsis or septic shock. The CMS still follow the 3-hour and 6-hour bundles. (See The hour-1 bundle.)
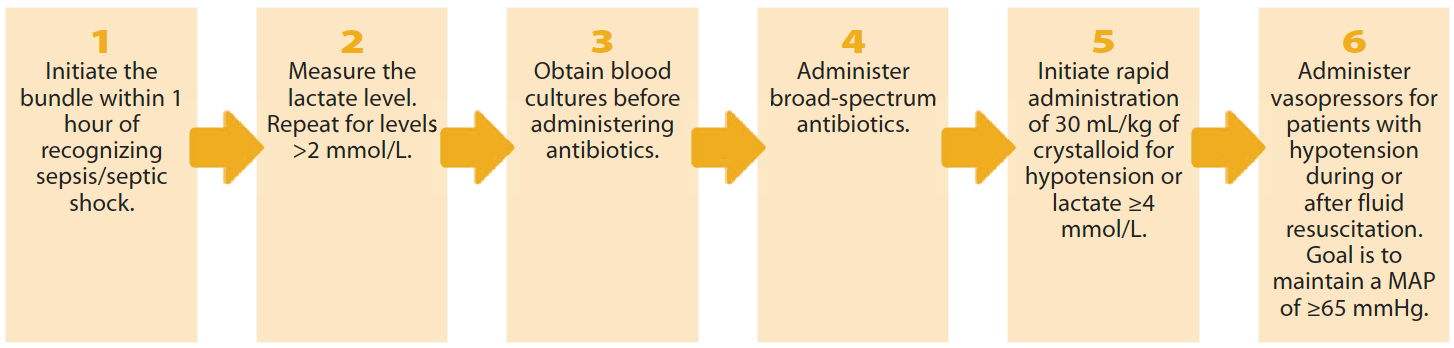
The hour-1 bundle
The 2018 Society of Critical Care Medicine and European Society of Intensive Care Medicine Surviving Sepsis Campaign Hour-1 Bundle of Care includes the following steps
Initiating treatment
Within 1 hour of recognizing sepsis in Mr. Martin, the emergency provider orders I.V. access and laboratory specimen collection. When the patient arrives in the ICU, the nurse practitioner (NP) orders titrated supplemental oxygen 2L via nasal cannula to keep SpO2 above 96%. Supplemental oxygen should be given to all patients with sepsis to maintain oxygenation between 90% and 96%. If Mr. Martin develops sepsis-induced hypoxemic respiratory failure, the guidelines suggest using high-flow nasal oxygen rather than noninvasive ventilation when appropriate.
The NP orders arterial blood gases (ABGs). Results include pH, 7.25; PaCo2, 59; PaO2, 55; HCO3, 11. Bloodwork shows the following: white blood cell, 21.3 × 103 cells/mm3; creatinine, 2.7 mg/dL; and blood glucose, 178 mg/dL. In addition, the coagulation studies indicate PT, 10; PTT, 26; and INR, 1.1.
The ICU nurse identifies two qSOFA components (tachypnea and altered mental status) and three SIRS criteria (tachypnea, febrile illness, and leukocytosis). She reports these findings to the NP.
In addition, tests indicate lactic acidosis (4.5 mmol/L), which frequently occurs in patients with sepsis or septic shock; it’s associated with an increased risk for morbidity and mortality. Treatment involves addressing the underlying cause and any additional contributors, which supports the need to avoid delays. One possible course of treatment includes sodium bicarbonate; however, the International Guidelines for Management of Sepsis and Septic Shock recommend against bicarbonate therapy to improve hemodynamics or reduce vasopressor requirements in patients with hypoperfusion-induced lactic acidemia with pH ≥7.15.
The NP orders I.V. broad-spectrum antibiotics after ensuring that cultures have been obtained. Empiric antibiotics should target the suspected infection sources based on patient history, physical examination, and preliminary laboratory findings and imaging. Infection sources that require incision, drainage, or debridement require prompt action. Given the suspicion that Mr. Martin’s foot wound may be the source of his infection, the NP orders a wound consultation. Ultimately, the team decides that the wound doesn’t need incision, drainage, or debridement.
The NP orders hourly vital signs with the goal of maintaining a MAP of ≥65 mm Hg. Because Mr. Martin can’t remember the last time he urinated and he’s hemodynamically unstable, the NP places an order for 0.9% sodium chloride at a rate of 1,000 mL every 60 minutes for a total of 3 L (3,000 mL) in 3 hours. (The patient weighs 220 lb [100 kg] and the guidelines suggest 30 mL/kg.).
The ICU staff observe Mr. Martin’s response to the I.V. fluids and monitor him for signs of fluid volume overload. The nurse places a urinary catheter as ordered. The urine output goal is ≥0.5 mL/kg per hour. Urinary catheters increase the risk of infections and should be considered only if clinically necessary. Patients like Mr. Martin who have sepsis and fail to respond to initial therapy, are hypotensive, in shock, and require ICU monitoring, fit this criterion. The NP discusses the plan of care for the first 72 hours with Mr. Martin and his wife.
Continuum of care
At the 2-hour mark, Mr. Martin’s BP is 92/36 mmHg (MAP 55 mmHg). The NP orders catheters to monitor central venous pressure (CVP) and an arterial line (A-line) for BP monitoring. These catheters increase the risk of infection and should be placed only when necessary. They’re indicated for patients with sepsis, those with labile blood pressures, or when hemodynamic responsiveness requires frequent monitoring. A CVP may be placed if the patient is receiving large volumes of I.V. fluids or vasopressors are anticipated or administered.
The A-line confirms Mr. Martin’s low BP; his CVP is 6 cm H2O (normal is 5 to 12 cm H2O). Central venous oxygen saturation (ScvO2) will aid monitoring of Mr. Martin’s oxygen consumption, which serves as an indicator of tissue perfusion and reflects the percentage of oxygen returned to the right side of the heart after tissue consumption. The target ScvO2 for Mr. M is 70%.
Venous thromboembolism prophylaxis and vasopressors
Also, at the 2-hour mark, after reporting the BP and pulse pressure to the NP, the nurse suggests ordering venous thromboembolism (VTE) prophylaxis and norepinephrine.
In sepsis, the arterioles and capillary beds vasodilate, resulting in a widened pulse pressure and occasionally a low diastolic pressure. Capillary beds dilate, causing fluid to leak into the interstitial spaces, which leads to intravascular volume deficit. Dilated capillary beds and dehydration impair oxygen delivery to the tissues, promoting intravascular thrombosis. Fluid resuscitation helps restore circulating blood volume and tissue perfusion and decreases the risk for thrombus formation.
To reduce the risk of a VTE, adults with sepsis or septic shock should receive pharmacologic VTE prophylaxis, unless contraindicated. Mr. Martin displays no contradictions, so the NP places an order for low-molecular-weight heparin per the hospital’s protocol.
If I.V fluids fail to work, I.V. vasopressors such as norepinephrine are added per the guidelines. Norepinephrine is an α1-adrenergic agent with β1-adrenergic properties, which can increase cardiac output when administered early in septic shock. Norepinephrine will cause peripheral arteriolar vasoconstriction, slow the leakage into the interstitial spaces, help maintain circulating blood volume, increase myocardial contractility and heart rate, and improve tissue oxygen consumption.
Mr. Martin’s NP orders I.V. norepinephrine infusion to help achieve a MAP of 65 mmHg and continues initial fluid resuscitation. She also orders another infusion of 0.9% sodium chloride at 100 mL/hr after completing resuscitation fluids. The nurse continues to monitor Mr. Martin’s oxygen saturation and response to therapy.
Treatment response
Six hours after starting the norepinephrine infusion, the NP orders a repeat ABG, which shows signs of normalization. In addition, a repeat lactate level indicates a decrease to 2.8 mmol/L; Mr. Martin’s ScvO2 is 72% and CVP is 8 cm H2O. His urine output is 0.6 mL/kg per hour. His skin feels warm and moist. He’s more alert and asks why he’s in the hospital. These findings indicate improved tissue perfusion and mental status.
Over the next few days, the healthcare team continues monitoring Mr. Martin for signs and symptoms of improvement and complications. The NP orders repeat laboratory values every 6 hours until trends normalize; for Mr. Martin, that means a MAP of 65 mmHg and CVP of 8 to 12 mmHg.
When he achieves these levels, the nurse reports them to the NP and requests an order to discontinue all catheters and I.V. devices that are no longer required and to de-escalate the antibiotics.
Because I.V.s and catheters present an infection risk, all unneeded devices should be removed. The guidelines recommend daily assessment for de-escalation of antimicrobials, as shorter antimicrobial therapy may offer more effectiveness than longer therapy. Procalcitonin levels combined with clinical evaluation (rather than clinical evaluation alone) can aid in determining antimicrobial de-escalation.
Mr. Martin’s NP orders the removal of all unneeded I.V.s and catheters. In addition, the team begins weaning the patient off of vasopressor support. The wound and the skin around the wound show marked improvement with +2 pulses and capillary refill >2 seconds.
On Day 3, Mr. Martin is transferred to the medical–surgical unit and prepared for discharge home on Day 5 after admission.
Patient education and discharge
New guidelines recommend involving both the patients recovering from sepsis and their families in care discussions and hospital discharge plans. These discussions can help address physical and psychological concerns and ensure early and ongoing follow-up with healthcare providers to manage long-term effects. Barriers to providing care include a lack of patient education, misunderstanding of that education, differences in healthcare delivery systems, and confusion about dosing and the intensity of many proposed interventions. Each barrier requires investigation and resolution to ensure proper post-hospital care.
For Mr. Martin and his wife, the nurse provides written and verbal education, discusses his discharge plan, and makes a follow-up care appointment with his primary care provider. The nurse also offers information about local support groups. By the time Mr. Martin is discharged home, all of his questions had been answered.
Special considerations
All patients with sepsis and septic shock have individual requirements for treatment. The 2021 guidelines include other recommendations that don’t apply to Mr. Martin but should be considered in other situations. For example, the guidelines contain specific information regarding patients with glucose instabilities, cardiac dysfunctions, renal complications, and ventilation requirements. Nurses and other healthcare providers should compare the new guidelines to the needs of each patient.
Saving lives
Early recognition and treatment of sepsis proved pivotal to Mr. Martin’s recovery. The condition must be identified with treatment initiated within 1 hour of presentation. Nurses’ role in screening patients for sepsis saves lives.
*Name is fictitious.
Kelly Martinez is an assistant professor in the School of Nursing at Southern Connecticut State University in New Haven.
References
Agency for Healthcare Research and Quality. Toolkit for reducing catheter-associated urinary tract infections in hospital units: Implementation guide. October 2015. ahrq.gov/hai/cauti-tools/impl-guide/index.html
Bassett AM, Ka-Chun S, Honaker JA. Using functional ability measures to assess fall risk in acute care. West J Nurs Res. 2020;42(12):1050-8. doi:10.1177/0193945920924637
Centers for Disease Control and Prevention. CDC launches new effort aimed at strengthening survival and recovery rates for all sepsis patients. August 24, 2023. cdc.gov/media/releases/2023/s0824-sepsis-patients.html
Centers for Disease Control and Prevention. Hospital sepsis program core elements. cdc.gov/sepsis/hcp/core-elements/?CDC_AAref_Val=https://www.cdc.gov/sepsis/core-elements.html
Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063-e1143. doi:10.1097/CCM.0000000000005337
Giuliano KK, Baker D. Sepsis in the context of nonventilator hospital-acquired pneumonia. Am J Crit Care. 2020;29(1):9-14. doi:10.4037/ajcc2020402
Guarino M, Perna B, Cesaro AE, et al. 2023 update on sepsis and septic shock in adult patients: Management in the emergency department. J Clin Med. 12(9):3188. doi:10.3390/jcm12093188
Hamzaoui O, Shi R. Early norepinephrine use in septic shock. J Thorac Dis. 2020;12(Suppl 1):S72-7. doi:10.21037/jtd.2019.12.50
Koch C, Edinger F, Fischer T, et al. Comparison of qSOFA score, SOFA score, and SIRS criteria for the prediction of infection and mortality among surgical intermediate and intensive care patients. World J Emerg Surg. 2020;15(1)63. doi:10.1186/s13017-020-00343-y
Mikkelsen ME, Gaieski DF, Johnson NJ. Novel tools for hemodynamic monitoring in critically ill patients with shock. UpToDate. 2019. uptodate.com/contents/novel-tools-for-hemodynamic-monitoring-in-critically-ill-patients-with-shock?search=sepsis%20and%20urine%20output%20&topicRef=1613&source=see_link
National Institute of Neurological reference Disorders and Stroke. Meningitis and encephalitis fact sheet. March 3, 2020. catalog.ninds.nih.gov/sites/default/files/publications/meningitis-encephalitis.pdf
Neviere, R., Parsons, P. E., & Finlay, G. Sepsis syndromes in adults: Epidemiology, definitions, clinical presentation, diagnosis, and prognosis. UpToDate. 2025. uptodate.com/contents/sepsis-syndromes-in-adults-epidemiology-definitions-clinical-presentation-diagnosis-and-prognosis
Oczkowski S, Alshamsi F, Belley-Cote E, et al., Surviving Sepsis Campaign Guidelines 2021: Highlights for the practicing clinician. Pol Arch Intern Med. 2022;132(7-8):16290. doi:10.20452/pamw.16290
Park S, Jeon K, Oh DK, et al. Normothermia in patients with sepsis who present to emergency departments is associated with low compliance with sepsis bundles and increased in-hospital mortality rate. Crit Care Med. 2020;48(10):1462-70. doi:10.1097/CCM.0000000000004493
Schmidt GA, Mandel J, Bell TD. Evaluation and management of suspected sepsis and septic shock in adults. UpToDate. October 17, 2024. uptodate.com/contents/evaluation-and-management-of-suspected-sepsis-and-septic-shock-in-adults
Seetharaman S, Wilson C, Landrum M, et al. Does use of electronic alerts for systemic inflammatory response syndrome (SIRS) to identify patients with sepsis improve mortality? Am J Med. 2019;132(7):862-8. doi:10.1016/j.amjmed.2019.01.032
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801-10. doi:10.1001/jama.2016.0287
Society of Critical Care Medicine. Surviving Sepsis Campaign Guidelines 2021. sccm.org/clinical-resources/guidelines/guidelines/surviving-sepsis-guidelines-2021
Key words: sepsis, quick Sepsis Related Failure Assessment, systemic inflammatory response syndrome, sepsis guidelines
American Nurse Journal. 2025; 20(5). Doi: 10.51256/ANJ052506