The importance of incorporating the NCBSN Clinical Judgment Measurement Model
When the COVID-19 pandemic hit in 2020, educators from all disciplines faced a compelling challenge: How to ensure continuity in instruction while supporting various student needs, many of which were compounded by quarantine, health issues, job insecurity, and myriad other complex concerns inherent to a global pandemic. Few educational programs felt this more acutely than those that prepare students for careers in healthcare. In nursing curricula, for example, face-to-face teaching was reduced or unavailable, and clinical experiences in healthcare settings became limited or nonexistent. Communities that had already been experiencing the strain of a worsening nursing shortage faced a decrease in nursing students who would soon progress to graduation and practice.
Across the country, the solution appeared in various forms of online instruction, with real-time presentations as the predominant path forward. Online education isn’t a new concept, but for many students and faculty, the pandemic presented the first time they experienced it. With limited time or experience to prepare, many programs selected pre-packaged, web-based solutions to provide learning experiences that closely replicated clinical learning.
Many healthcare facilities have begun re-opening their doors to students, but virtual simulation has become a recognized, vital component of nursing curriculum. It allows students to familiarize themselves with standardized procedures, evaluate their knowledge and decision-making processes, and engage in specific, scaffolded situations in preparation for real-life experiences. It also allows for assessment within the context of the National Council for Licensure Exam (NCLEX) blueprint. However, the immediacy of the clinical need during the pandemic prompted quick adoption of virtual simulation, frequently without traditional due-diligence and training. According to Triemstra and colleagues, many nursing educators had to manage virtual experiences without appropriate training or guidelines, which led to varied accountability measures and expectations. We need standardized protocols that incorporate the National Council of State Boards of Nursing (NCSBN) Clinical Judgment Measurement Model for developing and gauging future nurses’ critical thinking and decision-making skills. (See Measuring clinical judgement.)
Measuring clinical judgment
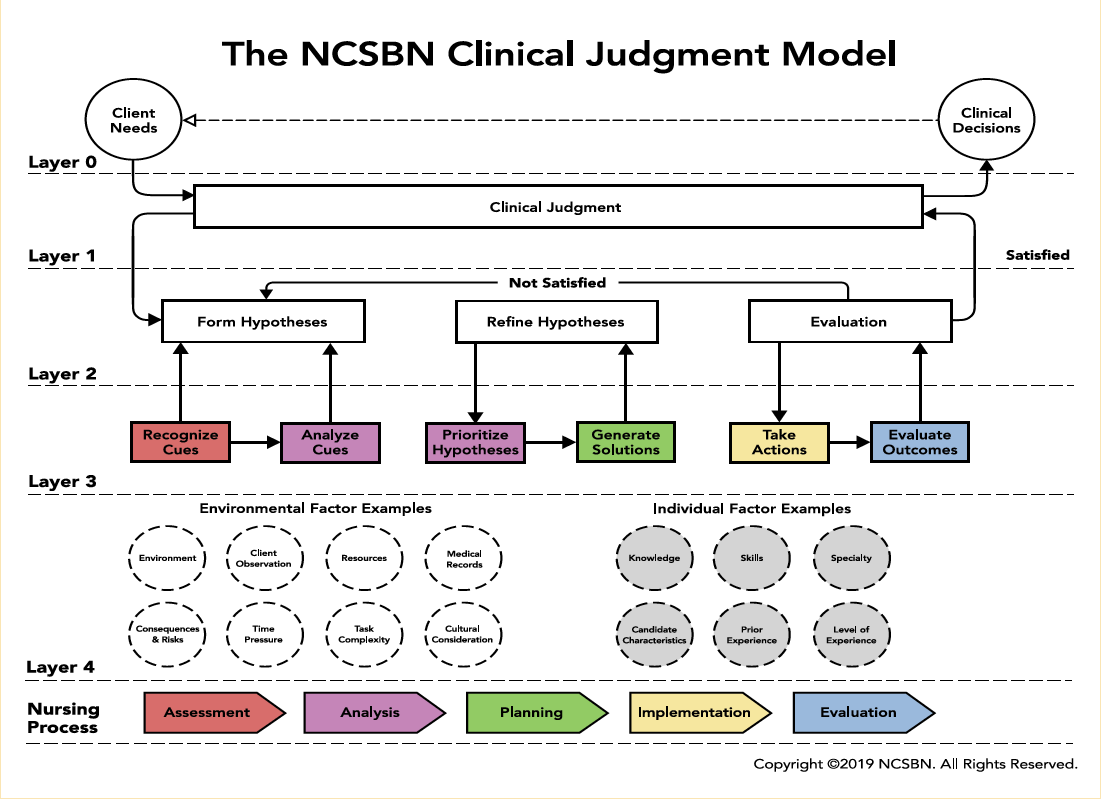
The National Council of State Boards of Nursing Clinical Judgment Measurement Model establishes a standardized method for measuring nurses’ clinical judgment (“a higher-order cognitive construct that represents medical knowledge, skill, decision making, and critical thinking”), which aligns with how nurses think in practice when making decisions about care delivery. The model is described in layers (0 to 4); Layer 3 serves as a basis for developing NextGen NCLEX test items and focuses on recognizing and analyzing cues, prioritizing a hypothesis, generating solutions, taking actions, and evaluating outcomes. Rather than simply collecting assessment findings, students also prioritize their findings to determine the most important.
Standardization and the virtual clinical
A standardized approach requires a curriculum plan, and virtual simulation environments can provide single or multiple patient care experiences designed to meet course objectives. Faculty assess the virtual patients to determine appropriate learning objectives for the experience and align them with objectives and program outcomes. Assigning dedicated virtual patients to specific courses allows educators to provide a consistent learning experience without duplicating the same patient across multiple courses. This approach helps increase active learning.
Virtual clinical simulation provides several advantages. For example, students can treat simulated patients in scenarios that promote realism, collaborative learning, active participation, and clinical reasoning, but with the freedom to make mistakes and learn from them without fear of harming a patient. Within this safe learning environment, instructors can use the simulation to address errors in real-time. In addition, students can review progress, remediate, and repeat a module until they achieve a successful outcome. Each opportunity for self-reflection on their decision-making and the ultimate outcomes helps to reinforce the skills nurses need for bedside autonomy as they encounter increased patient acuity, expanded roles, increased use of technology, and limited resources.
Standardized clinical day
The layout of the clinical day serves as the first step in standardizing the virtual clinical environment, which provides a consistent process for students and educators and optimizes faculty training and new employee orientation. Incorporating International Nursing Association of Clinical and Simulation Learning strategies ensures meeting clinical standards. Necessary criteria include creating the perception of realism. Students receive preparation materials based on the learning objectives, and the clinical day begins with a pre-briefing and ends with a debriefing. For a 7-hour clinical day, we break down assignments and briefing sessions as follows:
- Pre-clinical assignments (60 minutes)
- Pre-briefing (60 minutes)
- Simulation and post-quiz (90 minutes)
- Mid-day briefing (60 minutes)
- Break (30 minutes)
- Post-clinical assignments (60 minutes)
- Debriefing (60 minutes)
Pre-clinical assignments
Before beginning the clinical day, students complete several pre-clinical assignments, including research and reflection, medication cards, clinical judgment worksheets, and solution generation and action. These assignments allow students to form hypotheses and potential plans of action before they interact with the simulated patient.
Research and reflection. Most pre-packaged simulation platforms come with suggested readings and lessons related to each patient; however, educators can create these based on patient specifics and intended learning objectives. After students receive notification of their assigned patient, they review relevant readings related to pathophysiology, patient history, medications, social dynamics, skills, and diagnostics. To ensure completion of independent readings, students take a pre-clinical quiz. They must obtain a passing score to participate in the virtual clinical experience.
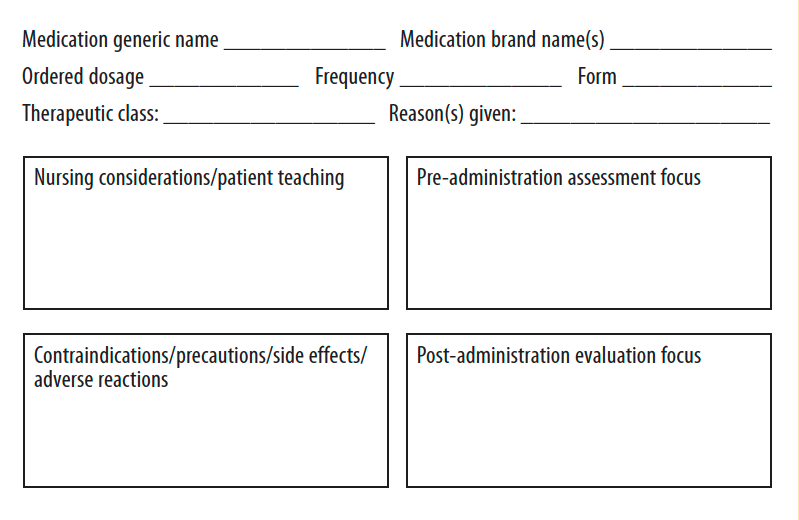
Medication cards. Students create medication cards relevant to their assigned patient. The cards include medications planned for administration during the clinical day, home medications, and potential prescriptions based on patient presentation. Earlier medication card templates were similar to a drug book, which allowed students to easily copy and paste information. The new templates have several changes related to design and completion requirements. For example, they must be handwritten, which, according to Chemin, can better aid comprehension compared with typing notes. In addition, a section added to the cards focuses on pre- and post-assessment. Medications are administered for a reason, and this section forces students to think about why the provider ordered a specific medication and what effect it will have. Knowing the medication’s action helps students establish baseline data during pre-administration assessments, and then determine medication effectiveness after administration. (See Medication cards.)
Medication cards
In pre-clinical assignments, students complete a card for each of the simulated patient’s medications, including those planned for the virtual clinical day, home medications, and those that might be prescribed.
Clinical judgment worksheet. Students complete a clinical judgment worksheet based on information they uncovered when researching the patient and by reviewing the patient shift report and electronic health record (EHR). The worksheet also is incorporated into the pre-briefing discussion on the clinical day. Students review the simulated patient’s information and use the NCSBN Clinical Judgment Measurement Model to organize and prioritize data. They can accomplish this by clustering and linking related information to create groupings of individual cues. They’ll then address data based on priority (first, second, and third). (See Clinical judgment worksheet.)
Clinical judgment worksheet
In the pre-clinical assignment, students use the clinical judgment worksheet to organize and prioritize information gathered during their research and review of the patient’s electronic health record.
- The first column (patient data) emphasizes recognizing cues (situational awareness); students list all patient and associated data that stand out. Many student nurses struggle with situational awareness because of their focus on task completion.
- The second column (relevant/essential patient data) requires students to recognize and analyze cues to identify relevant data essential to address during patient care. This occurs through observation and differentiating between normal and abnormal findings.
- The third column (prioritize data) has students categorize and rank subjective and objective data.
Solution generation and action. Based on the priority data generated using the clinical judgment worksheet, the student develops a list of independent and collaborative nursing interventions and parameters to monitor while providing care. Clinical judgment is a higher-order cognitive skill, so solution implementation may be multifaceted, requiring further measurements of physical status to determine the main concern.
Clinical day
The clinical day includes a pre-briefing, simulation, mid-day debriefing and evaluation, post-clinical assignments, and final debriefing.
Pre-briefing. Before students begin delivering care to the virtual patient, the instructor leads a pre-briefing to set the tone for the upcoming learning experience and to review the simulation objectives. The instructor reviews the information included in the pre-clinical worksheets submitted by students and discusses the day’s patient. To gain insight into students’ knowledge gaps and to guide feedback, the instructor asks about the students’ decision-making processes and rationales behind their choices.
Simulation. After the pre-briefing, the instructor releases the students to independently access their patient and complete the simulation. The instructor also logs onto the virtual platform and accesses the gradebook to ensure students are working on their patient. In real time, instructors can review the number of attempts students make to obtain a passing score, the length of time per attempt, and the feedback log for each student. In addition to seeing the actions taken and in what order, the instructor gains insight into students’ decision-making processes as well as how they prioritize patient care. Each patient faculty guide includes the proper sequence of student actions so instructors can compare individual student’s thought processes to the exemplar. In addition, the instructor can review errors within the simulation to create talking points for the mid-day briefing. (See Correct treatment sequence.)
Correct treatment sequence
The following serves an example of a correct treatment sequence for a patient after knee surgery. The instructor compares the student’s actions and thought processes against this list for later discussion.
- Perform hand hygiene.
- Choose personal protective equipment (PPE) (glove and gown).
- Introduce self.
- Identify the patient.
- Provide patient education on PPE.
- Obtain vital signs.
- Ask about allergies.
- Assess pain level.
- Check the provider’s orders in the electronic health record.
- Asses the diagnostics for signs of infection.
- Assess the I.V. site and flush.
- Assess the knee dressing.
- Provide patient education on wound care.
- Examine the legs for sensation, motion, strength, and color.
- Assess the pedal pulses and capillary refill.
- Auscultate the lungs.
- Provide patient education on incentive spirometry.
- Ask the patient to demonstrate using the incentive spirometer.
- Provide patient education on coughing and deep breathing exercises.
- Ask the patient to demonstrate coughing.
- Provide patient education on activities, safety, and fall risk.
- Complete the head-to-toe assessment.
Students access the virtual EHR during the simulation and begin their documentation.
Using a split screen or opening the simulation and the chart in separate browsers allows students to document throughout the simulation and practice bedside charting, which improves patient safety and saves time.
Mid-day debriefing and evaluation. After a designated amount of time, the students and instructor meet virtually for a mid-day debriefing. The instructor discusses the patient simulation and asks various questions, such as, What did students want to accomplish? What happened when they went into the patient’s room? What would they do differently next time? What alternative outcomes would they hope to achieve by changing their approach to care? What can they learn from this? At the end of the mid-day debriefing, the instructor goes into the virtual EHR and releases new data.
Evaluation forms the final element of the clinical measurement model. Students evaluate whether nursing interventions implemented during the simulation resulted in the expected outcomes. Frequently, nursing students discuss the evaluation of patient outcomes hypothetically by providing their understanding of what outcomes would constitute improvement or decline. When instructors release new data in the EHR, students can see actual outcomes, including new lab results, diagnostic reports, nursing or provider notes, and documented patient feedback. Having actual outcomes available for review enhances students’ ability to critically analyze their meaning.
Post-clinical assignments. After the mid-day debriefing, students work independently for another designated period of time to complete their post-simulation quiz and clinical judgment worksheet. They must score a passing grade on the quiz and submit their worksheets by the end of the clinical day. The post-simulation clinical worksheet takes each step from the NCSBN Clinical Judgment Measurement Model and presents them as answerable questions (see Post-simulation worksheet).
Post-simulation worksheet
The post-simulation worksheet uses the Clinical Judgment Measurement Model to present students with answerable questions.
Recognizing cues:
1. When you initially interacted with your patient, what did you notice? As you spent more time with the patient, what did you notice?
Analyzing cues:
2. What did you think about the situation as you were in it? Did you recognize the cause of the patient problem, any patterns or immediate resolutions to the problem?
3. What other information did you determine you needed? What did you do to obtain that information? How did your patient assist you with obtaining the information?
4. As you observed the patient and collected data, what did you believe was happening in those moments?
Generate solutions:
5. How did your observations and data collection guide your actions?
6. What were your goals for the patient as well as the situation you were involved in?
Reflection in action:
7. Reflect on your actions and what happened. How did your patient respond through the simulation? What was your action based on your patient’s response? How will you use this information in your nursing career?
Students create a table that lists all new findings available in the EHR after the mid-day debriefing, which allows the instructor to assess their ability to evaluate care. Students must determine if each piece of new information represents decline, improvement, or no change in patient status. If the patients’ status deteriorates or remains unchanged, students review and analyze the cues to generate new solutions. These practices aim to promote improvement in patient outcomes and progression toward a safe discharge.
Final debriefing. During the final debriefing, the instructor leads students through a review of any updated information made available in the EHR since mid-day. Before standardization of the virtual environment and the incorporation of the NCSBN Clinical Judgment Measurement Model, students completed their simulation and then worked on assignments for the rest of the clinical day. To make the virtual environment more realistic, an evolution of care delivery needed to occur—providers round, new orders are entered, and patients may experience a change in condition. During the final debriefing, students review this information and discuss additional required interventions.
A simulation vendor may incorporate these EHR information changes into a provided virtual case, or the faculty can create them. For example, during the virtual simulation, a student may be caring for a patient with a pulmonary embolism that develops after hip replacement surgery. They review the diagnostics and patient assessment, then implement a heparin infusion based on the provider’s orders. At the mid-day debriefing, the instructor can release new information into the EHR that indicates the patient’s surgical dressing is now saturated with bright red blood. Students must recognize this change in condition, understand the implications and risks for the patient, and generate new actions to take, which in this case might include calling the provider, additional diagnostic testing, or titration of the heparin drip based on diagnostics and provider orders. Discussion about evaluating care effectiveness provides a vital and meaningful learning opportunity during a final debriefing, but before standardization proved difficult in a virtual simulation experience.
By the end of the final debriefing, students must submit their EHR documentation. Similar to an in-person clinical, students can’t leave the facility until completing their documentation. Students also must submit a post-simulation clinical judgment worksheet for grading. This combination of pre- and post-simulation work, intentional faculty–student and student–student interactions throughout the clinical day, patient care practice in real time, and time spent in three separate briefing sessions has enhanced student engagement and improved learning outcomes.
Enhanced learning opportunities
Benefits of setting expectations regarding a standard clinical day schedule, required assignments, and both student and faculty accountabilities can enhance the overall simulated clinical experience while ensuring measurable and equivalent outcomes. Compared with a traditional facility-based clinical experience—which can include tremendous variability in patient access, staff receptibility, and instructor engagement—the standardized model of virtual clinical delivery provides an approach that helps meet specific goals and fills identified knowledge gaps. Because consistent delivery of virtual clinical experiences requires standardized faculty training, phase two of this project will focus on coaching virtual clinical faculty and staff to improve their performance and promote the intended goal of enriching nursing student learning experiences with frequent opportunities to make clinical judgments.
Lindy Fabry is the faculty clinical coordinator at Herzing University in Madison, Wisconsin, and a doctoral project chair at Grand Canyon University in Phoenix, Arizona. Leila Casteel is the associate vice president of curriculum and innovation at Herzing University and a family nurse practitioner at an internal medicine and pediatric practice in Brentwood, Tennessee.
American Nurse Journal. 2023; 18(6). Doi: 10.51256/ANJ0623119
References
Betts J, Muntean W, Doyoung K, Jorion N, Dickison P. Building a method for writing clinical judgment items for entry-level nursing exams. J Appl Testing Tech. 2019;
20(S2):21-36. ncsbn.org/public-files/Building_a_Method_for_Writing_Clinical_Judgment_It.pdf
Chemin A. Handwriting vs typing: Is the pen still mightier than the keyboard? The Guardian. December 16, 2014. theguardian.com/science/2014/dec/16/cognitive-benefits-handwriting-decline-typing
Cowperthwait A, Graber J, Carlsen A, Cowperthwait M, Mekulski H. Innovations in virtual education for clinical and simulation learning. J Prof Nurs. 2021;37(5):1011-17. doi:10.1016/j.profnurs.2021.06.010
Donovan LM, Mullen LK. Expanding nursing simulation programs with a standardized patient protocol on therapeutic communication. Nurse Educ Pract. 2019;38:126-31. doi:10.1016/j.nepr.2019.05.015
Galeti´c F. Online learning vs traditional learning: The research of student attitudes. Proceedings of FEB Zagreb International Odyssey Conference on Economics and Business; Zagreb. 2021;3(1).
HealthySimulation. Clinical simulation. healthysimulation.com/clinical-simulation
Hillier M, Williams TL, Chidume T. (2022). Standardization of standardized patient training in medical simulation. StatPearls. July 25, 2022. ncbi.nlm.nih.gov/books/NBK560864
Hughes PG, Hughes KE. Briefing Prior to Simulation Activity. National Library of Medicine. St. Petersburg, FL: StatPearls Publishing; 2023.
Ignatavicius DD, Silvestri L. Getting ready for the Next-Generation NCLEX® (NGN): How to shift from the nursing process to clinical judgment in nursing. Elsevier. evolve.elsevier.com/education/expertise/next-generation-nclex/ngn-transitioning-from-the-nursing-process-to-clinical-judgment/
INACSL Standards Committee. Healthcare Simulation Standards of Best Practice™: The debriefing process. Clin Simul Nurs. 2021;58:27-32. doi:10.1016/j.ecns.2021.08.011
Jiminez F. Using Virtual Patient Simulation in Substitution for Traditional Clinical Hours in Undergraduate Nursing. Shadow Health. 2017. evolve.elsevier.com/education/wp-content/uploads/sites/2/virtual_patient_simulation_clinical_hours_research_report_0627.pdf
Lippincott Solutions. Turning new nurses into critical thinkers. Combining domain expertise with advanced technology. June 7, 2018. wolterskluwer.com/en/expert-insights/turning-new-nurses-into-critical-thinkers
Mauk T, Ingram SR. Preparing for the Next Generation NCLEX®. UWorld Nursing. nursing.uworld.com/blog/educators/next-generation-nclex/
National Council of State Boards of Nursing. Clinical Judgment Measurement Model. ncsbn.org/exams/next-generation-nclex/NGN+Resources/clinical-judgment-measurement-model.page
National Council of States Boards of Nursing. 2017 RN Practice Analysis: Linking the NCLEX-RN Examination to Practice. US & Canada. ncsbn.org/public-files/17_RN_US_Canada_Practice_Analysis.pdf
Sokol K. Virtual simulation helps prepare nursing students for NextGen NCLEX. HealthySimulation. February 14, 2023. healthysimulation.com/47920/virtual-simulation-nclex-rn/
Triemstra JD, Haas MRC, Bhavsar-Burke I, et al. Impact of the COVID-19 pandemic on the clinical learning environment: Addressing identified gaps and seizing opportunities. Acad Med. 2021;96(9):1276-81. doi:10.1097/ACM.0000000000004013
Tung HH. [Embracing renovation and innovation during the pandemic: Application of virtual simulation technology in nurse practitioner education]. Hu Li Za Zhi. 2021; 68(5):7-12. doi:10.6224/JN.202110_68(5).02