Take steps to protect patient and nurse well-being.
Eyes see only light, ears hear only sound, but a listening heart perceives meaning. -David Steindl-Rast
- Implicit biases (unconscious biases) are pervasive; we all have them, but they can be unlearned.
- Similar to medication, nurses words have the ability to heal or harm.
- Listening is the essence of good communication; it’s a skill that requires practice.
On the other side of the nurse-as-superhero coin lies a hard truth—some nurses may not like caring for certain patients. Corley and Goren highlighted dark side behaviors that some patients may trigger in nurses, which ultimately threaten quality of care. It’s a fallacy to think that we can separate ourselves from our attitudes, beliefs, and values when we step across the threshold of healthcare into our nursing role. The truth is, we may not like caring for some patients because they’re different from us. We may struggle to understand them on a basic human level. We may not understand the choices they made or didn’t make that brought them into the hospital.
In 1978, Groves’ classic article highlighted physician struggles when caring for difficult patients. In the nursing literature, caring for difficult patients is well-documented, but much less exists about strategies to help us stay the course. To ensure just care delivery, we must first acknowledge that we might not like caring for some patients and then seek to understand why. Several trauma-informed strategies can help improve care delivery to these patients and also improve nurse wellness by striving, as Gunderman and Gunderman implored, to “glimpse the dignity…in every patient.”
Acknowledge our limitations, understand implicit bias
Throughout our lives we form implicit associations regarding certain character traits, such as race, age, ethnicity, appearance, or behaviors, such as drug use. The implicit associations that develop can be negative or positive, and they overshadow all our interactions, assessments, and reactions. This implicit bias results in unconsciously projecting these associations onto the people we encounter. Implicit biases are pervasive—we all have them. Implicit (unconscious) bias isn’t the same as known bias, which we consciously choose to conceal due to social constraints. (See Bias examples.)
Bias examples
We all have implicit biases that we’ve learned throughout our lives. Unlearning them begins with acknowledgement. Types of biases include the following:
- Affinity bias: A preference for people who look like us.
- Ageism: Discrimination based on age.
- Attribution bias: Judgments and assumptions made about a person’s behavior that may not reflect reality. For example, attributing blame for a sexual assault on the victim for the clothing they were wearing or alcohol they consumed.
- Beauty bias: Judgments based on outward appearance.
- Confirmation bias: Tendency to lean toward evidence that supports our opinions, giving it greater weight.
- Conformity bias: To achieve acceptance by the social group, individual opinion is swayed and tends to agree or align with group views.
- Gender bias: Preference for one gender over another.
- Name bias: Discrimination based on an individual’s name. For example, favoring English-sounding names over names from other nationalities.
To better understand implicit bias, let’s examine it through the lens of patients with substance use disorder. These individuals tend to experience marginalization, stigmatization, and traumatization in their interactions, including those with healthcare professionals and systems.
Consider a patient with substance use disorder who arrives in the emergency department. Diagnostic overshadowing and confirmation bias, which are similar, may occur as we make assumptions that support our beliefs. In diagnostic overshadowing, we attribute the patient’s symptoms to drug use. With confirmation bias, we may assume that the patient is only coming into the hospital for drugs. These assumptions endanger patient care. As nurses, we tend to practice in concert, resulting in conformity bias. For example, when nurses on a unit espouse the same views and share collective frustrations when caring for patients with substance use disorder, they may give those patients a lower priority assessment level. A study by Monks and colleagues noted one nurse’s comment of saving patients with substance use disorder till last or dropping them to the “bottom of the heap.”
Because our biases occur involuntarily, triggered deep within our subconscious, identifying them through reflection can challenge us. The good news is that we can unlearn our biases. The first step is to acknowledge that we all have them.
Embrace our vulnerabilities as nurses
Rather than denying that we may have the capacity to dislike or dread caring for certain patients, we need to embrace this as a human truth. From this perspective, we can work on unlearning our implicit biases. We can deconstruct the implicit associations that we’ve built over a lifetime and then unlearn or combat them using strategies developed by Devine and colleagues. (See 6 strategies to deconstruct implicit bias).
6 strategies to deconstruct implicit bias
Implementing the following strategies can help us understand our implicit biases and ultimately improve patient outcomes.
Replace the stereotype
Stop, think, and consciously choose to adjust your response to the patient.
Counter the stereotype
Pause and reimagine the possibilities for your patient.
Individuation
See your patient as an individual human, not the disease or condition they have.
Take perspective
Metaphorically place yourself on the other side of the bed rail and dare to imagine what your patient might be experiencing.
Increase opportunities for connection
Pull up a stool and spend time with your patient to get to know them. Listen to their stories.
Build partnership
Work with your patient and embrace them as a care collaborator.
As nurses, we must make a conscious effort to question our ideologies. If we find ourselves experiencing dread over a patient assignment, we must ask ourselves why. Am I experiencing bias?
Words as medicine
Words have the power to heal or destroy, to induce or reduce harm. When caring for patients with substance use disorder, for example, we tend to “talk dirty” (for example, we refer to a patient’s urine sample as “dirty” when it’s positive and “clean” when it’s negative). A study by Kelly and colleagues highlighted the harm of stigmatizing language. We must think before we speak. Patients aren’t “dirty” or “clean.”
Using person-first language acknowledges our patients as people living with a disease or condition (they’re a patient still actively using drugs or an individual in recovery). When we call them an addict or alcoholic, we apply a label and relegate them to a disease, erasing their humanity. Goffman started the conversation about the damaging effect of stigma in his 1963 classic work. It can prove highly caustic and has the power to affect population health.
Marissa Angerer, a Texas Shatterproof Ambassador (Shatterproof works to eliminate the stigma and shame associated with addiction prevention and treatment by focusing on science and compassion), shared her experience with the power of words: “Some words felt like attacks, attempting to replace my true identity…The words become grenades—strategically spoken at times in order to do the most damage…These labels erased my humanity. Total strangers felt allowed to criticize or judge me, saying that I was ‘such a waste of life,’ ‘useless,’ or ‘just a drunk or addict’…Spoken words cannot be un-said and they have the power to build up a person, or to destroy a person. When we choose to be compassionate, we become part of the solution, giving an opportunity to others to be successful.”
If we greet our patients on admission with outright disdain (terse voice, arms crossed, and using stigmatizing language), they may react negatively, increasing the risk for violence. Humans are no different than animals when wounded and will react to their environment. With incidents of violence toward nurses increasing, we must work strategically to protect ourselves by mitigating care-related drama, which may cause trauma and a subsequent negative reaction from the patient. In a study by Monks and colleagues, a patient recalled a nurse asking, “‘Why should we waste a bed on you, you type of people?’… So that was it, I went nuclear [became verbally and physically violent].”
We must change the conversation to improve patient outcomes and nurse wellness with thoughtful and compassionate trauma-informed communication. This approach allows us to build a bridge that will cross the chasm created by implicit bias. (See Learn a new language.)
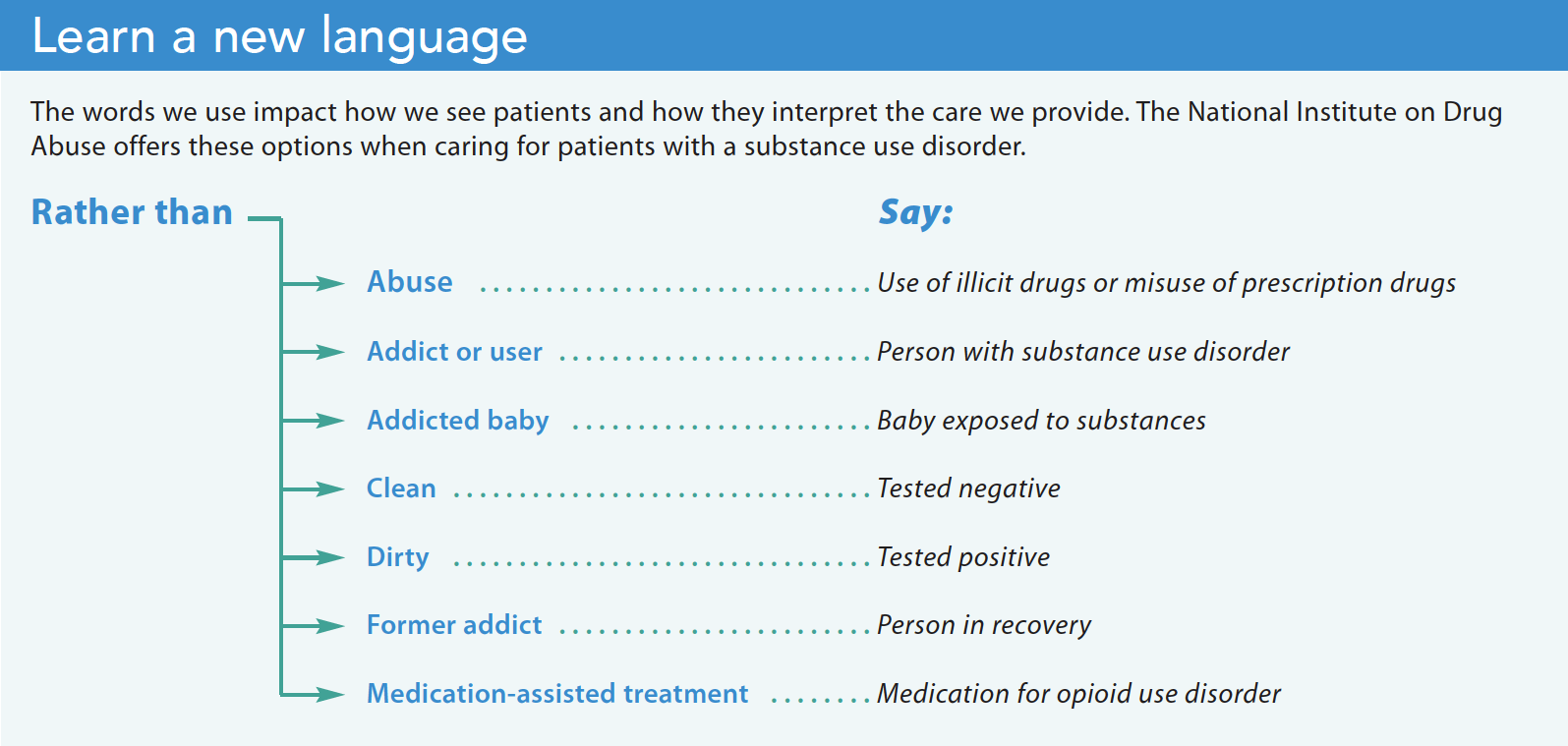
Let’s go even further. If words are medicine, might we then check them against the same standard as the medications we administer? We must remember that it’s not just what we say, but also how we say it and the context of the conversation. (See Words as medicine: Six rights of administration.)
Words as medicine: Six rights of administration
Similar to the rights of medication administration (right patient, right medication, right indication, right dose, right time, right route), we should pause before speaking and ask ourselves the following questions:
- Is the message communicated to the right person?
- Does the message contain the right words for the situation (therapeutic, not therapeutic)?
- Is the message the right amount (not too much or too little)?
- Is the message communicated at the right time?
- Is the message communicated via the right route (verbal, demonstrated, written) in the appropriate manner (intonation, pitch, speed, gestures, facial expression)?
- Do I have the right documentation to capture the essence of the message?
Our goal should be to understand our patient’s perspective before we expect them to understand ours. That requires compassionate, trauma-informed communication, which includes practicing the art of listening.
Learn to listen
Listening requires work, including psychological and emotional investment with the person who’s speaking. When we truly listen to our patients we give them the dignity and respect they deserve. Keep in mind that hearing and listening aren’t the same. Hearing is the decoding of a message, a physical response and perception involving sound waves. Listening involves attention, which entails selective perception because our brains allow only a few stimuli to come into our focus. We can hear someone, without listening to them. People frequently say, “I hear what you’re saying,” but that’s not accurate. A better response might be, “I hear you, I’m listening, and I want to understand you.” (See Listening modes.)
Listening modes
Tyagi, who describes the following three modes of listening, contends that with practice, we can improve our listening skills.
- Active or reflective listening: You’re actively engaged and genuinely interested in the views and message of the other person. You check in with the speaker to verify that you understand.
- Does the message contain the right words for the situation (therapeutic, not therapeutic)?
- Passive or attentive listening. You’re interested in what the other person is saying, but you’re not reflecting back. You assume that you understand what the speaker said.
- Competitive or combative listening. Rather than focusing on the speaker, you’re preoccupied with your response. You look for opportunities to jump in with your opinion or you interrupt.
How often do we stress that communication is key but place little value on listening. We need to listen not only to what our patients are saying, but also pay attention to the subtle nuances of body language that convey the unspoken. We must dare to be silent, and just listen. (See Improve your listening skills.)
Embrace our professional identity, improve nurse wellness
Godfrey defines nurse professional identity as having four domains that undergird our practice. They include a set of core values and principles that serve as a guide for our professional behavior (values and ethics) and our capacity to appraise and apply best information and evidence to enhance the care we give (knowledge). As the most trusted profession, we can influence others to transform a vision into reality (nurse as leader). In addition, our professional behavior includes the words we speak, our actions, and our steadfast presence, which demonstrate our courage to care—even for people we might not like (professional comportment).
We can embrace our vulnerabilities to combat our biases, engage in compassionate communication that replaces words that harm with words that heal, and we can learn the skills required to listen to our patients. We have the power to overcome implicit bias with kindness. AN
Improve your listening skills
Tyagi, who describes the following three modes of listening, contends that with practice, we can improve our listening skills.
- Face the patient. Sit tall and lean in a little.
- Meet their eyes. If the patient is comfortable with eye contact, maintain it as much as possible.
- Focus. Pay attention to what the patient is saying, not on how you want to respond.
- Keep an open mind. To avoid making assumptions and jumping to conclusions, wait until the patient has finished speaking.
- Hold your tongue. This is hard, but wait to speak until after the patient has shared their thoughts.
- Respond appropriately. To show you understand, communicate understanding with your body, such as a raise of the eyebrows, a nod of the head, or a “hmmm.”
- Listen with your eyes. Observe the unsaid communication and pay attention to nonverbal cues.
- Visualize. Try to see what the patient is telling you; attempt to mentally enter their world.
Kendrea Todt is an assistant professor of nursing and honors coordinator at the College of Nursing, East Tennessee State University in Johnson City.
American Nurse Journal. 2023; 18(7). Doi: 10.51256/ANJ072319
References
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: American Nurses Association; 2015. nursingworld.org/practice-policy/nursing-excellence/ethics/code-of-ethics-for-nurses/coe-view-only/
Botticelli MP, Koh HK. Changing the language of addiction. JAMA. 2016;316(13):1361-2. doi:10.1001/jama.2016.11874
Corley MC, Goren S. The dark side of nursing: Impact of stigmatizing responses on patients. Sch Inq for Nurs Pract. 1998;12(2):99-22.
Devine PG, Forscher PS, Austin AJ, Cox WTL. Long-term reduction in implicit race bias: A prejudice habit-breaking intervention. J Exp Soc Psychol. 2012;48(6):1267-78.
Godfrey N. New language for the journey: Embracing a professional identity in nursing. J Radiol Nurs. 2022;41(1):15-7. doi:10.1016/j.jradnu.2021.12.001
Goffman E. Stigma: Notes on the Management of Spoiled Identity. New York, NY: Touchstone; 1963.
Greenwald AG, Banaji MR. Implicit social cognition: Attitudes, self-esteem, and stereotypes. Psychol Rev. 1995;102(1):4-27. doi:10.1037/0033-295X.102.1.4
Groves J. Taking care of the hateful patient. N Engl J Med. 1978;298:883-7. doi:10.1056/NEJM197804202981605
Gunderman RB, Gunderman PR. Forty years since Taking care of the hateful patient. AMA J Ethics. 2017:19(4):369-73. doi:10.1001/journalofethics.2017.19.4.nlit1-1704
Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Pub Health. 2013;103(5):813-21. doi:10.2105/AJPH.2012.301069
Institute for Healthcare Improvement. How to reduce implicit bias. September 28, 2017. ihi.org/communities/blogs/how-to-reduce-implicit-bias
The Joint Commission. Diagnostic overshadowing among groups experiencing health disparities. Sentinel Event Alert. June 22, 2022. jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/sentinel-event/sea-65-diagnostic-overshadowing-6-16-22-final.pdf
Kelly JF, Wakeman SE, Saitz R. Stop talking dirty: Clinicians, language, and quality of care for the leading cause of preventable death in the United States. Am J Med. 2015;
128(1):8-9. doi:10.1016/j.amjmed.2014.07.043
Kirwan Institute for the Study of Race and Ethnicity. Understanding implicit bias. May 29, 2012. kirwaninstitute.osu.edu/article/understanding-implicit-bias
Landau SF, Bendalak J, Amitay G, Marcus O. Factors related to negative feelings experienced by emergency department patients and accompanying persons: An Israeli study. Isr J Health Policy Res. 2018;7(1):1-9. doi:10.1186/s13584-017-0200-1
Monks R, Topping A, Newell R. The dissonant care management of illicit drug users in medical wards, the views of nurses and patients: A grounded theory study. J Adv Nurs. 2013;
69(4):935-46. doi: 10.1111/j.1365-2648.2012.06088.x
National Institute on Drug Abuse. Words matterTerms to use and avoid when talking about addiction: A CME/CE. July 15, 2021. https://nida.nih.gov/nidamed-medical-health-professionals/health-professions-education/cmece-activities/your-words-matter-terms-to-use-avoid-when-talking-about-addiction-cmece-activity
National School of Healthcare Science. Understanding different types of bias. October 13, 2022. nshcs.hee.nhs.uk/about/equality-diversity-and-inclusion/conscious-inclusion/understanding-different-types-of-bias
Pauly BB, McCall J, Browne AJ, Parker J, Mollison A. Toward cultural safety: Nurse and patient perceptions of illicit substance use in a hospitalized setting. Adv Nurs Sci. 2015;38(2):121-35. doi:10.1097/ANS.0000000000000070
Shatterproof. National Movement to End Addiction Stigma. Addiction Language Guide. shatterproof.org/sites/default/files/2021-02/Stigma-AddictionLanguageGuide-v3.pdf
Substance Abuse and Mental Health Services Administration. TIP 57: Trauma-informed care in behavioral health services. store.samhsa.gov/product/TIP-57-Trauma-Informed-Care-in-Behavioral-Health-Services/SMA14-4816
Todt KL, Thomas SP. The lived experience of nurses caring for patients diagnosed with intravenous drug useassociated infective endocarditis in Appalachia: A phenomenological study. J Am Psychiatr Nurses Assoc. 2021:10783903211037735. doi:10.1177/10783903211037735
Tyagi B. Listening: An important skill and its various aspects. The Criterion. 2013;12:1-8. the-criterion.com/V4/n1/Babita.pdf
Key words: implicit bias, stigma, trauma-informed care, communication skills, substance use disorder



















2 Comments. Leave new
Good article I plan on using this in a session with 1st year students.
We’re glad you enjoyed it! Thank you for reading American Nurse!