
This fingerprint of nursing enhances the visibility of nurses’ contributions.
Takeaways:
- A unique nurse identifier (UNI), a defined code or series of characters, represents an individual nurse within healthcare technology systems and across healthcare organizations.
- UNIs can help quantify nursing-sensitive outcomes and increase the evidence of their contributions to patient care.
With the growing prevalence of digital technologies in healthcare and a shift toward value-based reimbursement, a mechanism to identify and quantify nursing contributions to quality patient outcomes is critical. Implementing a unique nurse identifier (UNI) to leverage across systems and technologies will provide evidence of nursing’s value to patient care delivery from multiple data sources.
What is a UNI?
A UNI is a defined code or series of characters that represents an individual nurse within various healthcare technology systems and devices (such as electronic health records [EHRs]). (See Definitions.) It connects data across these systems to provide evidence of nursing’s value to patient care delivery, making the effects of nursing assessments and interventions (such as fall prevention) more visible. Brennan and Bakken emphasized that data from medical devices and the EHR using a unique identifier will help customize intervention strategies for patients and healthcare operations. When nursing actions are identified, associated data can be mined to help benefit healthcare and the nursing profession. (See You already have a UNI.)
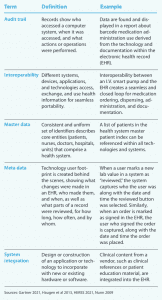
Definitions
Knowing these terms will help nurses better understand the benefits of unique nurse identifiers and advocate for their use.
Why do we need UNIs?
Despite the long history of nursing’s contributions, nursing-sensitive outcomes have been difficult to quantify. The work of a single nurse frequently is encompassed into the larger cost-reporting aspects of care that are captured by healthcare organizations in administrative billing and claims data. Without a mechanism to enable selecting data that describe individual nurse roles, we face challenges finding tangible evidence of the care we provide and demonstrating how it affects patient outcomes.
Nurses use many technologies (EHRs, physiologic monitoring, nurse call systems, secure messaging, automated medication dispensing systems, smart beds, smart infusion pumps) in the clinical care environment. In some organizations, the EHR is connected to an enterprise resource planning (ERP) system. These systems require user identification to provide access and track use. Standardizing the source of master data and user information can help simplify technology integration, workflow, and data collection.
When technologies aren’t integrated, nurses frequently become the human interface for information sharing between systems, sometimes manually entering data from one system or technology into another, which takes time away from patient care and can lead to communication errors. Automated data sharing among technologies can streamline workflows and eliminate steps, clicks, and duplicate documentation, helping to reduce errors.
How can UNIs help us?
UNIs provide opportunities beyond identifying nurses’ contributions to healthcare and streamlining workflows. For example, Macieira and colleagues studied the value and secondary use of standardized nursing data and found that UNIs can aid research, quality improvement, education, and performance recognition by connecting data to education level, years of experience, and expertise. A next step in improving the quality of care is to pay attention to the human effort of the individual nurse, in addition to organizational quality, safety structures, and processes.
Lulat and colleagues conducted a scoping review to develop a database of studies exploring RN effectiveness on outcomes (clinical, organizational, nurse, and patient). The aggregated database supported findings that better staffing is associated with decreased mortality, increased quality of care, fewer pressure injuries and infections, reduced length of stay, higher job satisfaction, reduced turnover, and positive financial outcomes for organizations.
However, we don’t know how variable staff composition might influence these outcomes. For example, individual nurse performance must be considered when evaluating medical surgical patient discharge acuity scores. Yakusheva and colleagues demonstrated that variation existed in nursing practice and outcomes when both a patient’s discharge acuity and the proportion of time a patient received care from an individual nurse were analyzed. We also must evaluate staff composition, performance, and needed organizational interventions to drive improvements.
In addition, UNIs can help facilitate quality improvement (QI) efforts. Frequently, QI and patient safety systems aren’t integrated with the EHR or other technologies. The UNI can simplify data evaluation, even when systems aren’t integrated, because nursing performance measures and outcomes will be more transparent, allowing for quality scores at aggregate and individual levels. These insights can provide opportunities for positive reinforcement and performance role models.
Other implications for UNIs in nurse staffing include the ability to easily measure, track, and quantify nursing work, transforming the traditional approach to staff mix from intuitive to quantifiable and measurable.
You already have a UNI
The National Council of State Boards of Nursing (NCSBN) has responded to the need for identifying nurses across educational programs, care settings, and individual state licensures by developing and maintaining the NCSBN unique identifier (NCSBN ID), which is matched exclusively to a nurse and not a state or organization. An ID is assigned to each nursing student when they register for the National Council Licensure Examination (NCLEX). Nurses licensed before NCLEX was implemented in 1994 also have been assigned IDs.
NCSBN maintains the identifiers in its Nursys database. Each day, state boards of nursing update licensure data in Nursys via secure file transfer. This data transfer makes Nursys the primary source for current information on existing and new nursing licensure records. The result is a report that the public can view immediately and is sent to healthcare organizations (hospitals, clinics, health systems) registered to receive the report.
The NPI
Nurses may choose to pursue additional identification numbers, such as National Provider Identification (NPI). The NPI, implemented in 2004, is a unique 10-digit number required for providers and organizations that transmit financial transactions electronically to federal and private health programs. In contrast to the NCSBN ID, which is automatically assigned, the NPI is granted through an online process using the National Plan and Provider Enumeration System (NPPES). Typically, the number is assigned in about 10 days.
Many nurses don’t apply for an NPI unless they provide a service for direct billing to payers. Similar to NCSBN IDs, individual NPIs are retained across care settings; however, holding an NPI does not confer licensure. Healthcare disciplines with NPIs provided by NPPES must select their taxonomy codes (which designate their classification and specialization), including primary care. NPPES doesn’t verify the accuracy of taxonomy codes selected by individuals.
What are the challenges?
Some nurses are concerned about how UNIs will be used, especially as a data point for measuring and tracking behavior. Will the information gathered with UNIs be used by organization leaders, operational stakeholders (such as nurse managers), and litigators to take disciplinary action? The focus of UNIs should be on addressing how nursing assessments, interventions, and documentation impact patient care, not as a tool to punish behavior.
Keep in mind that computer coding models used to monitor behaviors and clinical effectiveness aren’t new. Health data analysis to track and trend individual provider impact on care quality, clinical performance, and patient outcomes for public reporting already exists. Similarly, nursing data are captured and used to provide evidence of meeting nursing standards of care and measuring interventions associated with patient outcomes via nurse-sensitive quality and safety measures.
The Health Insurance and Portability Accountability Act (HIPAA) requires health system administrators to maintain records of all access to personal health information in the EHR and review the records intermittently to determine user conduct. Using HIPAA, healthcare organizations also closely examine who views the EHR to maintain data integrity for detecting changes. Strategies to fulfill this national mandate include audit functionality and metadata. For example, EHR audit trails assess compliance for timely documentation, messaging, and medication administration. Metadata (computer-generated data about other data) can be used to monitor safety alert acknowledgments and dismissals. These reporting strategies validate system integrity, mine quality improvement data, and detect insufficient workflows and opportunities for process improvements. Although these required audit capabilities may raise fears about tracking individual data, they actually identify opportunities for improvement and connect nursing contributions to patient outcomes.
Unique nurse identifier in action
According to Dudzik and colleagues, in-hospital cardiac arrest presents unique and critical challenges in which a healthcare provider’s performance can significantly alter patient survival rates. Clinicians maintain certifications that verify their competency to perform cardiopulmonary resuscitation (CPR) and other interventions, and recertification training usually occurs every 2 years. However, skill levels vary with no significant measurement or assessment on the potential impact on patient outcomes. For example, one care team member may use their CPR skills during several codes per week, but another may not administer CPR for 2 years. Currently, clinician CPR performance can’t be assessed objectively in real-time or longitudinally because no dynamic record of their previous performance exists. As a consequence, clinicians may be improperly matched with patient need.
To improve patient survival in pediatric code blue resuscitations, the Center for Medical Interoperability (C4MI) is exploring the concept of using a holistic learning system to measure caregiver task performance with a time-stamped process and medical devices. Evidence suggests that the value of understanding team and individual clinician knowledge development, improvement, and application may help improve patient outcomes.
Using the National Council of State Boards of Nursing (NCSBN) ID is a secure way to associate an individual nurse and medical device data. In addition to the medical device association, the unique ID may include license portability and continuing nursing education credit tracking in a longitudinal record associated with professional interventions. Ongoing medical device operability and data liquidity challenges associated with specific interventions remain the focus and intent of C4MI’s use case demonstration. Data liquidity challenges refer to data that aren’t in real-time, aren’t being useful, or aren’t within the workflow (for example, workflow data aren’t time-stamped or associated with a username). Nurse interventions must be measured so they can be studied to determine when care delivery adaptations are needed.
Use case
This case demonstrates using UNIs, data, and an intelligently coordinated system to match nurse skill with patient need. Each nurse has an associated score that reflects their CPR station performance so the team leader can best position each nurse when responding to a cardiac arrest. Individual caregiver credentials (based on NCSBN ID and CPR performance metrics) are displayed on an overhead dashboard. As care team members enter the patient’s room, the team leader assigns roles based on associated skill levels.
During the code, data from the patient monitor, defibrillator, and EHR along with the appropriate American Heart Association algorithm and caregivers’ active roles are aggregated on a CPR dashboard, giving the care team a simple visual display of all events, data, and guidance during the code. These data are accurately time-stamped and stored for debriefs and analytics.
This system helps bridge and synchronize disparate data streams to assess caregiver performance during cardiac arrest. When medical device and system outputs are time-synchronized alongside human activities and interventions, such as CPR compression depth and rate, real-time analysis is generated for event management, clinician performance, and outcomes scoring.
Future research in artificial intelligence and machine learning may be considered as data are collected, synchronized, and compared to data sets of similar patient populations. Using real-time analytics at the point of care, clinicians can receive guidance and feedback to maximize intervention and protocol effectiveness.
![]()
![]()
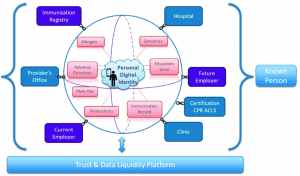
A known person has a personal digital identity that encompasses multiple points where data can be collected. This model illustrates using the unique nurse identifier in the pediatric code blue resuscitation use case.
How do we advance the use of UNIs?
Sensmeier and colleagues highlighted the importance of active collaboration with healthcare organizations and health information technology (IT) vendors as a focal point for advancing the UNI. Advocacy requires outreach, education, promotion strategies, and reducing barriers to adopting the National Council of State Boards of Nursing (NCSBN) ID. For example, the Alliance for Nursing Informatics has approved a policy statement recommending use of the NCSBN ID. Other advocacy strategies include partnerships with national associations and organizations such as HIMSS, American Academy of Nursing, American Medical Informatics Association, American Nurses Association, American Organization for Nursing Leadership, and the Office of the National Coordinator for Health Information Technology.
Implementing UNIs as a standard will require some vendors to revamp their products, while others may have an existing field where the UNI can be implemented. In either scenario, healthcare organizations will need to dedicate resources to implement the standard, and the work required may compete with an organization’s other clinical IT budget priorities and projects. However, implementing UNI is foundational to enabling organizational, nursing, and patient outcome insights, so organizations must evaluate both existing and new technology implementations to prioritize UNI.
Transforming practice
The road to transforming nursing practice will include UNIs, which will increase the evidence of our contributions to care delivery and healthcare outcomes through more nursing research, initiatives, and proof-of-concept pilot opportunities. UNI adoption is gaining traction with policymakers and advocates from national nursing and medical associations, societies, organizations, government agencies, and technology vendors. Individual nurses can aid the effort by supporting organizations in their implementation efforts and learning more about how the UNI can promote the profession and improve outcomes.
References
Afaneh T, Abu-Moghli F, Ahmad M. Nursing-sensitive indicators: A concept analysis. Nurs Manag. 2021;28(3):28-33. doi:10.7748/nm.2021.e1982
Brennan PF, Bakken S. Nursing needs big data and big data needs nursing. J Nurs Scholarsh. 2015;47(5):477-84. doi:10.1111/jnu.12159
Center for Medicare and Medicaid Services. Clinician Performance Information on Medicare Care Compare: 2019 Doctors and Clinicians Public Reporting. 2019. edit.cms.gov/files/document/2019-clinician-performance-information-release.pdf
Center for Medicare and Medicaid Services. Find your taxonomy code. October 10, 2020. cms.gov/Medicare/Provider-Enrollment-and-Certification/Find-Your-Taxonomy-Code
Dudzik LR, Heard DG, Griffin RE, et al. Implementation of a low-dose, high-frequency cardiac resuscitation quality improvement program in a community hospital. Jt Comm J Qual Patient Saf. 2019;45(12):789-97. doi: 10.1016/j.jcjq.2019.08.010
Gartner. Gartner glossary: Master data management (MDM). gartner.com/en/information-technology/glossary/master-data-management-mdm
Gartner. Gartner glossary: System integration. gartner.com/en/information-technology/glossary/system-integration
Haugen MB, Herrin B, Slivochka S, McNeil Tolley L, Warner D, Washington L. Rules for handling and maintaining metadata in the EHR. J AHIMA. 2013;84:50-4.
HIMSS. What is interoperability? himss.org/resources/interoperability-healthcare#Part1
Lulat Z, Blain-McLeod J, Grinspun D, Penney T, Harripaul-Yhap A, Rey M. Seventy years of RN effectiveness: A database development project to inform best practice. Worldviews Evid Based Nurs. 2018;15(4):281-9. doi:10.1111/wvn.12283
Macieira TGR, Chianca TCM, Smith MB, et al. Secondary use of standardized nursing care data for advancing nursing science and practice: A systematic review. J Am Med Inform Assoc. 2019;26(11):1401-11. doi:10.1093/jamia/ocz086
Nunn S. Managing audit trails. J AHIMA. 2009;80(9):44-5.
Nursing Knowledge: Big Data Science Conference Proceedings. Health IT Policy Workgroup: Engage and equip all nurses in health IT policy. 2018-2019 National action plan. June 13-15, 2018. nursing.umn.edu/sites/nursing.umn.edu/files/nkbds_proceedings_2018.pdf
Sensmeier J, Androwich I, Baernholdt M, et al. Demonstrating the value of nursing care through use of a unique nurse identifier. Online J Nurs Inform. 2019;23(2). himss.org/resources/demonstrating-value-nursing-care-through-use-unique-nurse-identifier
US Department of Health and Human Services. HIPAA Administrative Simplification: Standard Unique Health Identifier for Health Care Providers; Final Rule. 45 CFR Part 162. Federal Register. 2004;69(15):3434-69. cms.gov/Regulations-and-Guidance/Administrative-Simplification/NationalProvIdentStand/Downloads/NPIfinalrule.pdf
Werley HH. Introduction to the nursing minimum data set and its development. In: Werley HH, Lang NM, eds. Identification of the Nursing Minimum Data Set. New York City, NY: Springer; 1988; 1-15.
Yakusheva O, Needleman J, Bettencourt AP, Buerhaus PI. Is it time to peek under the hood of system-level approaches to quality and safety? Nurs Outlook. 2020;68(2):141-4. doi:10.1016/j.outlook.2019.11.004
Nancy Beale is the president of Beale & Assoc. LLC, in Cottage Grove, Wisconsin. Whende Carroll is the founder of Nurse Evolution in University Place, Washington. Kelly Aldrich is senior advisor at the Center for Medical Interoperability in Nashville, Tennessee. Susan Alexander is an associate professor at the University of Alabama in Huntsville. Marianne Baernholdt is associate dean of global initiatives and professor at the University of North Carolina in Chapel Hill. Willa Fields is a professor at San Diego State University in San Diego, California.


















3 Comments.
Spot on with this write-up, I actually believe this web site needs far more attention. I’ll probably be returning to read more, thanks for the information!
HI Alex, Using the UNI will not allow anyone to collect your personal information. The UNI is assigned to you when you take the NCLEX exam and is a publicly available ID which allows tracking your professional licensure across multiple states. Being able to use the UNI could help a university track the career progression of its graduates without using any personally identifiable information. The value within an organization comes from being able to capture nurse driven data across care settings or multiple systems to:
o Quantify the value of nursing care on patient outcomes
o Use data to improve nursing practice
Can I ask what exactly the purpose of my personal information being connected to a UNI? You claim that it’s going to provide all kinds of new data, but that’s not true. You can already know my title and what I accessed in an EHR without knowing my personal information. It can be anonymous, yet you claim that tying everything to a nurse and being able to track everything that they’ve done with all patients will somehow improve data that you can already obtain with EHR systems.