
Take a strategic approach to prevent lost opportunities for improvement.
Takeaways:
- Audit and feedback strategies are routinely implemented in clinical practice as a way to monitor compliance with various practices; however, they’re not always completed effectively.
- This article highlights key strategies to ensure audit and feedback success.
Audits are routinely done in clinical practice to monitor compliance with various practices, such as infection prevention bundles or fall and pressure injury prevention. Audit and feedback comprise a beneficial strategy for implementing and sustaining practice changes; however, the feedback component frequently gets lost in the process. Audits become onerous tasks to check off the to-do list, with data entered into a “black hole” never to be seen again, rendering audits unhelpful in improving practice.
In 2012, Ivers and colleagues conducted a systematic review looking at how effective audit and feedback strategies improve compliance with evidence-based practices. They found that audit and feedback may be most effective when:
- baseline data show that health professionals aren’t performing well to begin with
- the individuals completing audit and feedback are a peer or supervisor (known to the clinicians)
- audit and feedback data are provided more than once
- feedback is provided verbally and in writing
- feedback includes clear targets and an action plan.
Based on that information, and my personal experience, this article describes best practices for using audit and feedback to provide meaningful information to clinicians.
Audits
Knowing what should be audited, who should perform audits, how often they should be completed, and where findings should go will help ensure audits are targeted and that data are effectively stored and shared.
What should be audited?
Audits should be completed for practices where deficiencies exist and compliance requires improvement. Audits come in a variety of forms—some are standardized, such as through Institute for Healthcare Improvement bundles—and others are “homegrown” and tailored to the needs and processes of a specific unit or hospital. Common audits may address:
- catheter-associated urinary tract infection (CAUTI) prevention bundles
- central line-associated bloodstream infection (CLABSI) prevention bundles
- ventilator-associated pneumonia prevention bundles
- hospital-acquired pressure injury prevention
- fall prevention
- patient hygiene (such as bathing, oral care)
- hyperglycemia and hypoglycemia.
What should be included in audits?
Comprehensive audits should include the pertinent steps clinicians are required to take to prevent adverse events. CLABSI prevention bundle audits, for example, should include the steps taken to prevent CLABSI—changing the dressing, tubing, and needleless connectors per the manufacturer’s recommendations; assessing that dressings are clean, dry, and intact; assessing the need for a central line daily; and scrubbing the hub before accessing the line.
Who should complete audits?
According to Ivers and colleagues, auditors should be known to the clinicians, either as a peer or supervisor. Audits can be completed by unit staff who are “champions” for specific topics (such as a falls champion) or by charge nurses, unit leaders, or clinical nurse specialists. Anyone can be taught how to complete audits. Teaching nursing students or new nurses how to perform audits may help them learn the components included in various bundles. Having members of the nursing leadership team, such as managers, accompany auditors shows nurses that leaders are committed to and support auditing. In addition, these leaders can hold nurses accountable for any deficiencies noted during the audit.
How should audits be completed?
Audits have a bad reputation; many staff feel as though auditors are “policing” their practice and are simply pointing out what they do “wrong.” For staff to be most receptive, audits should be positioned as nonpunitive—they’re a way to improve practice by recognizing strengths and identifying barriers staff may be facing.
Many audits include observation and documentation review. For example, an auditor would need to review the patient’s chart when checking compliance with appropriate needleless connector changes during a CLABSI prevention bundle audit. However, assessing whether the dressing is clean, dry, and intact would require the auditor to go into the patient’s room and observe the dressing’s integrity.
Standardized forms can be helpful for audit consistency. Logistically, I’ve found it useful to first complete the documentation portion of audits, and then the observation portion. That way, any deficiencies identified through documentation can be communicated to the nursing staff during the observation component.
Where should audit data go?
After audit forms are completed, what should be done with the data? Ideally, it should be put into a repository so trends can be tracked over time. Various platforms exist, such as REDCap, The Joint Commission Resources (JCR) Portal, Smartsheets, or even a shared Microsoft Excel document. The Excel slicer function can be helpful for organizing and storing this type of data. (To learn more about this function, click here.)
Some units or hospitals may have audits sent to a centralized location for data entry. No matter what type of platform is used, repositories should be created so data trends can be easily retrieved and regularly shared with units and hospitals.
How often should audits be completed?
Audit frequency typically correlates with how big a “problem” a specific issue is. For example, if a unit struggles with CAUTIs, but not with falls, you would expect to complete CAUTI prevention bundle audits more frequently. If CAUTI audits show that the unit has high compliance (such as greater than 90%) on four out of five bundle components, but they struggle with one, targeted audits and education on that component may be helpful for a time. Targeted audits, when appropriate, can help alleviate the time and resources needed for full, comprehensive audits and still address the main issue.
When should audits be completed?
Generally, audits can be done at any time of day, but being strategic about timing can make them more effective. If possible, do audits on both day and night shifts. Night shift staff frequently feel left out of these types of activities, so including them can help improve their sense of ownership of any problem that exists. Complete audits when staff can talk with the auditor about the findings. Completing audits at 8:00 am when staff are preparing for their day, assessing patients, administering medications, and anticipating provider rounds, may not be the best time to discuss deficient audit components. Instead, complete audits when the unit is less busy, such as around 2:00 pm. Of course, every day is different and units can be extremely busy at any time, so use your best judgment and wait until a time or day when staff will be most receptive to the audit feedback.
Consider using feedback cards (such as the catheter-associated urinary tract infection [CAUTI] prevention bundle card below) to target comments to specific practices and steps as well as individual staff.
CAUTI prevention bundle feedback card | Yes | No | Comments |
Closed system maintained with red seal intact at junction of tubing/catheter? | |||
Drainage bag below the level of the bladder? | |||
No dependent loops in the tubing? | |||
Catheter tubing secured? | |||
Catheter clinically indicated? | |||
Perineal care completed per policy? | |||
Bag < 2/3 full? | |||
Overall Compliance |
Feedback
The information included in audit feedback, who delivers it, and how it’s delivered can affect how staff receive it and take steps to improve compliance.
What should be included in feedback?
Feedback can be provided in several ways: to individual nurses or as aggregated data to a group. One way to provide specific, individual data to nurses is to simply describe the audit you’re doing and tell them at least one strength and one area of opportunity. For example, “Today I’m doing a CAUTI prevention bundle audit. You did a great job securing the indwelling catheter to the securement device. Remember, though, to make sure the tubing doesn’t have any dependent loops by using the clip that comes with the catheter or by positioning the tubing appropriately.” Some units have small cards that auditors can use to check off practice steps and write comments. They then share the card with the nurse as a reminder. (See Individualize feedback.) Of course, any type of feedback is better received if candy or other type of small treat is provided.
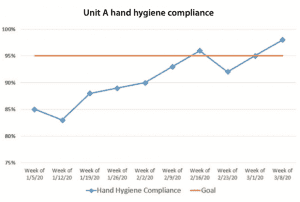
Feedback in the form of aggregated data can be shared at the unit or hospital level. Using run charts to display the data allows staff to see their progress over time. Run charts can be developed in Microsoft Excel and should be simple and easy to read. You want staff nurses to be able to immediately understand whether they’re meeting their target. (See Data on the run.)
Feedback should include clear targets and an action plan. Frequently, targets (such as 90% or 95% hand hygiene compliance) are set by unit or hospital leadership. Whatever the target is, make sure staff know and understand it. If they fall short, have an action plan that lists simple ways to improve compliance. All feedback should be actionable so staff know what they can do to improve.
A “kudos” section listed within the feedback can help improve staff morale and integrate friendly competition among staff members. For example, when I complete bathing audits, under the run chart, I include a list of nurses and nursing assistants who completed and documented a bath during the audit timeframe. This information is sent via email to staff so they’re recognized in front of their peers. Some units may even consider offering raffle prizes to staff with consistently high compliance. Be creative.
Who should provide feedback?
As noted previously, audit and feedback are most effective when it comes from a peer or supervisor. After I complete an audit, I request that the manager or other leadership member of the team communicate the findings to staff. Having a leadership member share feedback data shows that they support it. In addition, managers and leaders have the ability to hold staff accountable if they aren’t adhering to certain practices.
Run charts are a good way to aggregate audit data and share it at the unit or hospital level. The run chart below shows one unit’s improved hand hygiene compliance over 2 months.
How should feedback be provided?
Feedback data should be provided verbally and in writing. Aggregated data can be shared via e-mail, flyers placed on the unit, online dashboards, bulletin boards, and during huddles, rounding, and staff meetings. Communicating data verbally and in writing can help ensure staff receive the information. One emergency department communicated their hand hygiene compliance score on a poster designed to look like a restaurant letter grading form. Again, be creative in how you share audit information to staff.
How often should feedback be provided?
Audit feedback should be provided more than just once. Audits of a new practice (for example, if the unit or hospital just implemented chlorhexidine gluconate bathing) should be completed frequently (from once a week to several times a week). After compliance is at or near the targeted goal, audit and feedback can be done less frequently (once a month to several times a month). When the practice has been established and compliance has been at or near target for 6 to 12 months, audit and feedback can be done less frequently (once to several times a quarter).
Improving personal practice
Using audit and feedback can be an effective way to improve and sustain compliance with evidence-based practices. But simply completing audits isn’t enough. To be most effective, data should be shared with the end users so they know how to improve their personal practice.
Staci Reynolds is an assistant professor at Duke University School of Nursing in Durham, North Carolina.
References
Chan WV, Pearson TA, Bennett GC, et al. ACC/AHA special report: Clinical practice guideline implementation strategies: A summary of systematic reviews by the NHLBI implementation science work group. Circulation. 2017;135(9):e122-37.
Colquhoun HL, Carroll K, Eva KW. Advancing the literature of designing audit and feedback interventions: Identifying theory-informed hypotheses. Implement Sci. 2017;12(117). doi.org/10.1186/s13012-017-0646-0
Gould DJ, Moralejo D, Drey N, Chudleigh JH, Taljaard M. Interventions to improve hand hygiene compliance in patient care. Cochrane Database Syst Reviews. 2017;9(9):CD005186.
Institute for Healthcare Improvement. Evidence-based care bundles. ihi.org/Topics/Bundles/Pages/default.aspx
Ivers N, Jamtvedt G, Flottorp S, et al. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst Reviews. 2012;6(6):CD000259.
Wuchner SS. Integrative review of implementation strategies for translation of research-based evidence by nurses. Clin Nurse Spec. 2014;28(4):214-23.

















