Prompt, proper care will help reduce complications and improve quality of life.
Venous ulcers are the most common lower extremity wounds in the United States. Patients experience poor quality of life as a result of pain and immobility, and they require advanced levels of wound care. Any delay in care increases the risk of infection, sepsis, amputation, skin cancers, and death. Patients who develop complications may require frequent care visits, dressing changes, and recurrent hospitalizations. In addition, they may experience loss of productivity, significant discomfort, or disability.
Many patients with venous ulcers struggle with adherence to rigorous treatment regimens, and the COVID-19 pandemic has added to that challenge because of treatment delays. For example, risk of complications increases when venous reflux goes undertreated or untreated, increasing the incidence of venous ulcers, which can be costly for the healthcare system and detrimental to patients’ lives.
Targeted nursing education is essential to improve the assessment and management of venous leg ulcers. In addition, empowering patients to care for themselves can help bridge care gaps.
Pandemic impact on wound care
The COVID-19 pandemic has had a profound impact on healthcare, including wound care. The risk factors for venous ulcers and chronic wounds are similar to those that put patients at significant risk for COVID-19 infection and mortality. In addition, chronic wounds increase the risk of infection and hospitalization, which presents another challenge for an already overwhelmed hospital system.
A multidisciplinary approach in collaboration with a wound care center is the most beneficial for addressing wound care. However, during the height of the pandemic, the availability of expert care from a wound center was limited. The situation has eased in some geographic regions, but remains problematic in others.
Risk factors
Venous ulcers develop as a result of venous hypertension, which occurs due to valve dysfunction, outflow obstruction, arteriovenous malformation, and calf muscle pump failure. Risk factors include age (55 years and older), family history of chronic venous insufficiency, high body mass index (BMI), venous reflux in deep veins, medical history (pulmonary embolism, superficial or deep vein thrombosis, lower extremity skeletal or joint disease), multiple pregnancies, physical inactivity, and a history of venous ulcers. Poor prognostic indicators include a venous ulcer lasting more than 3 months, an ulcer 3.9 inches or larger, presence of arterial disease in the lower extremities, advanced age, and elevated BMI.
Evaluation of venous ulcers
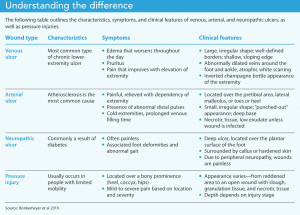
Venous ulcers are large and irregularly shaped with well-defined borders and a shallow, sloping edge. Slough with granulation tissue comprises the base of the wound, with moderate to heavy exudate. Patients typically experience no pain to mild pain in the extremity, which is relieved with elevation. Venous ulcers are most frequently located on the lower legs, such as above the lateral or medial malleolus with a medial and circumferential presentation.
Common symptoms include edema that worsens throughout the day, pruritus, pain that improves with elevation, and heaviness of the affected limb. Assessment frequently finds abnormally dilated veins around the foot and ankle, atrophic white scarring, and an inverted champagne bottle appearance of the extremity.
Differentiating lower extremity wounds
Understanding other lower extremity wounds—arterial ulcers, neuropathic ulcers, and pressure injuries—can help nurses differentiate them from venous ulcers. A detailed clinical history and thorough assessment when evaluating lower extremity ulcers can aid diagnosis and guide treatment, which may differ depending on the type of ulcer. (See Understanding the difference.)
Treatments for some types of wounds may be harmful for others. For example, if compression therapy is applied to a limb with arterial insufficiency that resulted in an arterial ulcer, blood flow can be reduced further, potentially leading to amputation.
Arterial ulcers
Arterial ulcers are small, have an irregular shape, and appear “punched-out” with a deep base. Typically, necrotic tissue is present with low exudate unless the wound is infected. The ulcers usually are located over the pretibial area, the lateral malleolus (outside ankle), or on the toes or heel.
Most patients report severe pain that’s relieved when the extremity is placed in a dependent position and increased when the extremity is elevated. Assessment findings include abnormal distal pulses, cold extremities, and prolonged venous filling time. Arterial ulcers may be caused by tissue ischemia resulting from atherosclerosis.
Arterial vs. venous ulcer
The following table compares venous and arterial ulcers, which can occur as a result of peripheral vascular disease.
| Arterial | Venous | |
| Pain | Intermittent on claudication | Dull, achy |
| Edema | None | Lower legs |
| Pulse | None or weak | Present |
| Drainage | None | Present |
| Shape | Round, smooth | Irregular borders |
| Skin | Black eschar | Ruddy or yellow slough |
| Temperature of extremity with ulcer | Cool | Normal to increased, if infection present |
| Common ulcer location | Toes and feet | Ankles |
Source: Vivas et al 2016
Neuropathic ulcers
Neuropathic ulcers are deep, surrounded by callus or hardened skin, and usually appear on the plantar surface of the foot or over a bony prominence such as the heel. The most common causes are diabetes or other neurologic diseases, which cause an abnormal gait with repetitive, uneven distribution of pressure on the foot. Because peripheral neuropathy is associated with these wounds, usually they’re painless and patients may not realize they exist.
Pressure injuries
Most pressure injuries are the result of limited mobility. They frequently develop over a bony prominence, such as the sacrum, coccyx, heels, or hips. Pressure injuries are attributed to three main causes: high pressure for a short time (such as an immobile patient lying in bed without repositioning), low pressure over a prolonged period, and device-related pressure and shear forces. A shear force pressure injury can occur when a patient is sitting “slumped” in a chair and the skin of the buttocks is stretched, interfering with circulation.
Pressure injuries can cause mild to severe pain depending on location and severity. Their appearance ranges from a reddened area to an open wound with slough, granulation tissue, and necrotic tissue. Wound depth depends on its stage.
Venous ulcer care
Venous ulcer management varies depending on severity and whether the current wound is a recurrence. Treatment options include conservative management and advanced therapy. The main goal of treatment for any stage of venous ulcer is healing, but preventing recurrence and reducing edema also are important.
Conservative treatment
Conservative treatment consists of compression therapy, dressings, debridement, and medication.
Compression therapy. Medical compression therapy (compression garments, containment devices, Velcro systems, and short and long stretch-fiber compression wraps) is the standard treatment for initial and long-term venous ulcer management in patients without arterial disease. Treatment goals include edema and pain reduction, circulation improvement, and healing enhancement. Adherence to this evidence-based therapy reduces the risk of recurrence.
Compression therapy works by providing static or dynamic mechanical compression to the extremity. Static compression, including hosiery and compression, is used to treat lower extremity chronic venous insufficiency. Dynamic (intermittent) compression therapy in the form of pneumatic compression pumps and sleeves may be useful under select circumstances, such as when lymphedema is present.
Different levels of compression are indicated for various conditions. For example, a compression garment that can compress at 15 to 20 mmHg (which can be obtained over-the-counter) is appropriate to reduce minor and occasional swelling as well as deep vein thrombosis risk when a patient is sitting for extended periods, such as on an airplane. Garments with a compression level greater than 20 mmHg require a prescription.
Compression therapy is contraindicated in arterial wounds, so correct diagnosis is required. To ensure appropriate compression therapy use, confirm that the patient’s ankle brachial index is in the safe range (0.5–0.8). Patients with diabetes, neuropathic disease, and peripheral artery disease should use compression carefully and only under their provider’s supervision.
Barriers to using compression garments include cost, wound drainage, pain, difficulty applying the garment, and physical impairments (such as obesity). Decreased range of motion and leg shape may cause the garment to roll down the leg or wrinkle, making garment donning and doffing difficult and compromising its effectiveness. Limited insurance coverage also may hinder access to compression therapy. Some insurance companies don’t cover preventive care, and Medicare covers only compression hose when a patient has an active ulceration; the mmHg must be 30 to 40 mmHg.
Dressings. Covering the wound with a dressing is recommended to promote moist wound healing. Choose dressings based on wound size, location, depth, moisture balance, presence of infection, allergies, comfort, odor management, ease and frequency of dressing changes, cost, and availability. Available dressings include those that cover wounds (absorbent and nonabsorbent) and topical (cadexomer iodine, povidone iodine, honey-based preparations, and sliver). Depending on the wound’s characteristics (stage of healing, amount of drainage), multiple types of dressings may be needed. For example, a wound bed may require a honey-based preparation dressing, but drainage from the surrounding peri-wound and tissue requires an absorbent dressing to keep the wound dry.
Debridement. Removing necrotic tissue by debridement may help expedite wound healing, but it requires a provider who is experienced with the procedure. In a study by Bonkemeyer and colleagues, patients receiving debridement at a wound care center showed significant reduction in wound size compared to those not treated with debridement. The amount of necrosis present in the wound bed will determine the type of debridement used. Maggots, lasers, monofilament fibers, forceps, scissors, or scalpels can be used to remove dead or blackened tissue to help promote healing. Debridement with monofilament fibers is relatively painless. The fibers detach, bind, and remove debris from the wound bed but also protect viable tissue.
Medications. Pentoxifylline (400 mg three times daily) may be used to increase microcirculation and oxygenation. In the study by Bonkemeyer and colleagues, this oral medication, used with or without compression therapy, promoted wound healing in patients with venous ulcers. Antibiotics should be prescribed if local signs of infection (swelling, redness, increased pain, and foul-smelling drainage) are present.
Other conservative treatments. Encouraging an hour of leg elevation daily may reduce the risk of venous ulcer recurrence. Also, mild exercise (such as walking and progressive resistant exercises) in conjunction with compression therapy may aid healing.
Advanced therapy
If a venous ulcer is unresponsive after 4 weeks of conservative therapy or does not respond to conventional therapy, advanced therapies are recommended. Approximately 6 million people in the United States are affected by ulcers that don’t respond to conventional therapy. Several options are available for these types of wounds, including collagen products, biological dressings, biological skin equivalents, keratinocytes, platelet-derived growth factor, platelet-rich plasma, silver products, intermittent pneumatic compression therapy, negative pressure wound therapy, electromagnetic therapy, hyperbaric oxygen, topical oxygen, and ozone oxygen. Skin grafting is another advanced option, but it should be reserved for large wounds. (See Advanced therapy options.)

Implications for future practice
Improving venous ulcer care requires increasing nurse wound care knowledge across settings and ensuring nurses work at the top of their scope of practice. For example, barring exclusion from a state’s nursing practice act, training in debridement of venous ulcers can be taught to nurses in many settings (including intensive care units, urgent care, primary care, and skilled nursing facilities) to facilitate care outside of wound care centers. In addition, nurses and patients can use monofilament devices for mechanical debridement.
The Centers for Medicare & Medicaid Services has paved the way for using telehealth during the pandemic, making it an ongoing viable option for helping patients adhere to treatment recommendations. It can be used for patient and family education and to perform screening and monitoring visits, effectively reducing barriers to care.
For more complex patients, home health nurses should be trained in advanced wound care to help reduce gaps in care during times of crisis and for patients unable to visit a wound care center. In addition, in-person or virtual patient self-care education is vital to ensure proper venous ulcer management if in-office or home health visits aren’t possible.
Nurse education
As more nurses who are inexperienced in wound care are required to care for venous ulcers, they should participate in additional continuing education, including online programs, to help improve decision-making during assessment and care. Flexible education options are needed to address the variety of settings where venous ulcer care occurs. Internet-based learning, such as clinical tools offered by the Wound, Ostomy, and Continence Nurses Society, provides easily accessible information to help guide nurses through venous ulcer identification, as well as care guidelines for assessment, prevention, protection, and management.
Prepared for the future
Partly as a result of the pandemic, healthcare providers who have limited experience assessing and managing venous ulcers and who work in locations that typically don’t see patients with these types of wounds are delivering care. Offering more education for providers in all settings and increasing the availability of home care will offset the risks and complications that patients with venous ulcers face. Ironically, the pandemic has resulted in innovative changes to ensure quality care for patients suffering from venous ulcers and prepare healthcare professionals for future crises.
Deetta K. Vance is an assistant professor, and Jessica Durbin is an associate professor at Indiana State University School of Nursing in Terre Haute.
References
Alonso-Zaldivar R. To keep seniors safe at home, Medicare expands telemedicine. US News & World Report. March 17, 2020.
Armstrong DG, Meyr AJ. Compression therapy for the treatment of chronic venous insufficiency. UpToDate. July 6, 2021.
Bonkemeyer Millan S, Gan R, Townsend PE. Venous ulcers: Diagnosis and treatment. Am Fam Physician. 2019;100(5):298-305.
Eschenbacher S, Barrera A. With obesity and diabetes epidemic, Mexico braces for coronavirus. U.S. Reuters. March 26, 2020.
Franki R. Comorbidities the rule in New York’s COVID-19 deaths. The Hospitalist. April 8, 2020.
Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. Washington, DC: Department of Veterans Affairs (US); 2012.
Guarnera G, Tinelli G, Abeni D, Di Pietro C, Sampogna F, Tabolli S. Pain and quality of life in patients with vascular leg ulcers: An Italian multicentre study. J Wound Care. 2007;16(8):347-51.doi: 10.12968/jowc.2007.16.8.27856
Hicks CW, Selvarajah S, Mathioudakis N, et al. Burden of infected diabetic foot ulcers on hospital admissions and costs. Ann Vasc Surg. 2016;33:149-58. doi:10.1016/j.avsg.2015.11.025
Kim PJ, Evans KK, Steinberg JS, Pollard ME, Attinger CE. Critical elements to building an effective wound care center. J Vasc Surg. 2013;57(6):1703-9. doi:10.1016/j.jvs.2012.11.112
Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: Systematic review and meta-analysis of observational studies. Ann Epidemiol. 2019;29:8-15. doi:10.1016/j.annepidem.2018.10.005
Mehrotra A, Chernew M, Linetsky D, Hatch H, Cutler D. The impact of the COVID-19 pandemic on outpatient visits: A rebound emerges. The Commonwealth Fund. May 19, 2020.
Nussbaum SR, Carter MJ, Fife CE, et al. An economic evaluation of the impact, cost, and Medicare policy implications of chronic nonhealing wounds. Value Health. 2018;21(1):27-32. doi:10.1016/j.jval.2017.07.007
Rogers LC, Armstrong, DG, Capotorto J, et al. Wound center without walls: The new model of providing care during the COVID-19 pandemic. Wounds. 2020;32(7):178-85.
Vivas A, Lev-Tov H, Kirsner RS. Venous leg ulcers. Ann Intern Med. 2016;165(3):ITC17-32. doi:10.7326/AITC201608020
Wound, Ostomy, and Continence Nurses Society. Clinical tools.