
Everything healthcare providers need to know
Editor’s note: This is an early release of a web exclusive article for the March 2021 issue of American Nurse Journal.
Takeaways:
• The 2020 American Heart Association (AHA) guidelines for basic life support (BLS) and emergency cardiovascular care have been released with some significant changes.
• For inpatient BLS providers, changes to the AHA guidelines include a new link to the chain of survival, added components regarding the resuscitation of pregnant individuals, opioid overdose assessment with treatment, and modifications for the skill components for some populations in basic cardiac life support.
The American Heart Association (AHA) affirms its commitment to enhancing patient outcomes with each new release of its guidelines, the most recent of which include significant changes. The 2020 AHA Guidelines for Basic Life Support (BLS) and Emergency Cardiovascular Care (ECC) include a new link to the chains of survival, additional components regarding the resuscitation of pregnant patients, opioid overdose assessment with treatment, and BLS skill modifications for some populations. Also, the AHA reminds BLS providers of the importance of early cardiopulmonary resuscitation (CPR) initiation.
General updates for all age groups
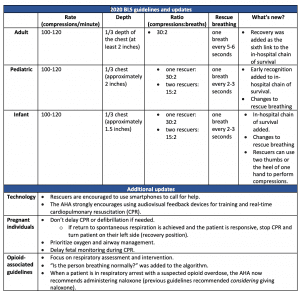
General recommendations for adult, child, and infant BLS include technology, CPR coaches, debriefing, and recovery. (See Guidelines and updates.)
Guidelines and updates
The American Heart Association (AHA) 2020 basic life support (BLS) updates include the addition of technology, new components, and skill modifications, as well as some elements that remain the same.
Technology
The new guidelines recommend using smartphones and audiovisual feedback devices. Using smartphones to call for emergency services decreases emergency response time activation, which promotes early CPR initiation and an optimal chain of survival. A study by Bircher shows that a delay in CPR for longer than 2 minutes decreases survival rates by 2.4%.
Audiovisual feedback devices provide real-time compression rate, depth, and recoil information to rescuers. They let the compressor know if they’re providing high-quality compressions, alerting them when they go below or above the targeted parameters. This allows them to make corrections for optimal perfusion and better patient outcomes. The AHA states that the use of audiovisual feedback devices during in-hospital cardiac arrests is associated with a 25% increase in survival due to improved CPR quality.
CPR coach
The CPR coach role has been added to the resuscitation team. CPR coaches coordinate CPR initiation, ensure adequate compressions, provide feedback to the compressor, and minimize the length of compression pauses, while the team leader focuses on holistic patient care. The AHA Provider Manual (2020) supports CPR coaches as part of the resuscitation team to enhance patient outcomes, including more effective CPR and fewer compression interruptions. This role can be incorporated into one of the existing roles on the team, for example, the person responsible for defibrillation also could serve as coach.
Debriefing
Cardiac arrest is stressful for BLS providers. Debriefing allows them to review the event and address their emotional well-being. In addition to support, debriefing provides opportunities for follow-up and feedback. It can occur immediately after a cardiac arrest or at a scheduled time to ensure team participation and allow for reflective thinking. Successful debriefing can help improve team performance, system processes, and patient outcomes.
Recovery
Recovery was added as the sixth link (in addition to early recognition and prevention, activation of emergency response, high-quality CPR, defibrillation, and post-cardiac arrest care) to the adult and pediatric in-hospital chains of survival because it continues long after a patient returns to spontaneous circulation (ROSC). The team should identify recovery goals early and complete a comprehensive interprofessional assessment. Focus recovery on the patient’s physical, cognitive, and psychosocial needs and incorporate them into discharge planning for return to home and work limitations.
Adult patients
With the exception of the general guideline updates, BLS for adult patients remains the same, including 30 compressions to two breaths. AHA has added specific guidelines for adult patients who are pregnant and those experiencing opioid-associated emergencies.
Pregnant patients
Guidelines for pregnant patients (who are prone to hypoxia, which can result in fetal harm) include initiating early CPR and defibrillation, prioritizing oxygenation and airway management, and delaying fetal monitoring until ROSC has been achieved. Fetal monitoring during CPR may interfere with patient resuscitation; however, if the patient is bradycardic but doesn’t require CPR, fetal monitoring can be performed. If ROSC is achieved and the patient is responsive, stop CPR and roll the patient on their left side (the recovery position). After cardiac arrest, expert fetal and obstetric consultation should be ordered.
A new opioid-associated emergency algorithm created for the 2020 BLS update focuses on the importance of respiratory assessment and intervention during life-threatening opioid-associated emergencies. The question “Is the patient breathing normally?” was added to reinforce the importance of respiratory assessment. Asking this question is included for patients with suspected opioid overdose who have a pulse but are breathing abnormally or gasping. The rescuer may suspect opioid overdose if medication or drug use was witnessed and reported, they see visible signs of injection on the skin, or if medication patches or bottles are found. This list isn’t all-inclusive but rather some indications of possible opioid overdose. If opioid overdose is suspected and the patient has a pulse but isn’t breathing normally, the rescuer should provide rescue breaths (one breath every 5-6 seconds) and administer naloxone per package instructions. However, CPR shouldn’t be delayed for patients with suspected opioid overdose and no pulse; administer naloxone after initiating CPR.
Pediatric patients and infants
Guidelines for infants and children remain at 30 compressions to two breaths for single-rescuer BLS and 15 compressions to two breaths for two-rescuer BLS. Rescue breathing has been increased to one breath every 2 to 3 seconds. This rate is associated with higher occurrence of ROSC and patient survival.
Single-provider CPR on infants has changed to allow the use of two thumbs or two fingers positioned right below the nipple line. Previously, the recommendation was two-finger position for single-rescuer BLS and two-thumb position for two-rescuer BLS. The updated guidelines recommend that if a provider can’t achieve the appropriate rate, depth, or recoil, the heel of one hand may be used. A review comparing different hand and finger positioning for infant BLS identified that all techniques demonstrated adequate CPR depth, rate, and recoil while also reducing rescuer fatigue.
In addition, early recognition has been added to the pediatric in-hospital chain of survival.
Improving patient outcomes
AHA’s guidelines continue to focus on early high-quality CPR initiation. Using technology (such as smartphones and audiovisual feedback devices) can enhance CPR quality and increase survival rates, and the addition of population-specific guidelines and updates to the chains of survival allow for more individualized patient care. Debriefing and recovery enhance healthcare provider and patient support after a cardiac arrest. Incorporating the AHA 2020 guidelines into patient care will improve patient outcomes.
Tiffany L. Conlin, Natalie M. Scarmack, and Courtney Nyoh are advanced clinical education specialists at UPMC Presbyterian Hospital in Pittsburgh, Pennsylvania.
References
American Heart Association. 2020 Guideline Resources. ahasso.heart.org/login?ReturnUrl=%2Fsaml%2Fsso%2Flogin%3FrequestId%3DAOZmI__bH55kDgRhx7wADRel_ZpUZqL3nw
American Heart Association. BLS instructor updates. elearning.heart.org/course/433
American Heart Association. Basic Life Support Provider Manual. Dallas, TX: American Heart Association; 2020.
Bircher C, Chan PS, Xu Y. Delays in cardiopulmonary resuscitation, defibrillation, and epinephrine administration all decrease survival in in-hospital cardiac arrest. Anesthesiology. 2019;130(3):414-22. doi:10.1097/ALN.0000000000002563
Nolan JP, Maconochie I, Soar J, et al. Executive summary: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142(16)(suppl 1):S2-27.
Olasveengen TM, Mancini ME, Perkins GD, et al. Adult basic life support: 2020 International Consensus on Cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142(16)(suppl 1):S41-91. doi:10.1161/CIR.0000000000000892


















3 Comments.
Important guidelines! The 2020 AHA BLS for inpatient settings aids in preserving lives. Thank you for highlighting these critical updates
This is likewise a decent post which I truly appreciated perusing. It isn’t each day that I have the likelihood to see something like this..
its very informative, thank you for sharing. Got new ways to work on this. Keep sharing.