
Prompt assessment and acute treatment aid symptom reduction.
- Migraine is a debilitating condition that alters the lives of many people worldwide.
- Migraine frequently goes misdiagnosed, underdiagnosed, and undertreated.
- Nurses play an important role in assessing for and managing migraine symptoms.
Charlotte Browne*, a 26-year-old white woman with no significant health history, arrives at the emergency department (ED) with a headache that started 2 days ago. She rates her pain, in the right temporal region, as 10/10. She also reports associated nausea and photophobia. At home, Ms. Browne took acetaminophen and naproxen with no relief. You take her vital signs, which are temperature 98.2°F (36.8°C), blood pressure 132/88 mmHg, heart rate 92 beats per minute, respiration rate 14 breaths per minute, and oxygen saturation 99% on room air.
Migraine headache, a common primary headache disorder, can present with excruciating pain and various associated symptoms, including nausea, phonophobia, and photophobia. In some cases, before the headache intensifies, the patient may experience an aura or a sensory disturbance. Although migraine affects more than 1 billion people worldwide, it’s frequently misdiagnosed and poorly treated. According to the American Migraine Foundation, less than 5% of those with migraine who sought care received a correct diagnosis and proper treatment.
Managing migraine in underserved populations
Neurocysticercosis: More than a headache
FDA allows marketing of first device to prevent migraine headaches
In addition to the burden of migraine pain, the condition also impacts the quality of life of more than 37 million people in the United States alone. The World Health Organization describes it as one of the 10 most disabling illnesses.
Providers diagnose migraine based on a detailed patient history and physical, so optimal care requires an understanding of the risk factors combined with a prompt and thorough evaluation. Nurses can gather this information and perform the assessment at the bedside.
Understand the ache
In the United States, headache accounts for more than 3.5 million ED visits annually. Headache can be broadly classified as primary or secondary. Distinguishing between the two guides assessment and management. Primary headaches occur in the absence of an underlying pathology or disease. The most common primary headaches include migraine (the second most common), tension-type, and cluster. Secondary headaches occur as a symptom of a disease, disorder, or underlying condition, including those caused by infections, head injuries, vascular disorders, and malignancies.
Risk factors
Many factors increase a person’s risk of migraine. Approximately 70% of those who experience migraine are women. Its prevalence peaks in patients between ages 25 to 55 years; frequency decreases with age. Migraine triggers and risk factors include fatigue, alcohol use, stress, lack of sleep, caffeine intake, certain foods and preservatives/additives, missing meals, physical activity, weather and altitude changes, menstruation, some medications (such as contraceptives), and overuse of acute migraine medications. Knowledge of risk factors can help guide your intuition, but assessment and history are key.
Assessment and clinical findings
 With no specific test for migraine, focus on a thorough physical assessment and history to rule out secondary headaches. Begin by excluding red flags and symptoms of other headache types. Red flags include a patient reporting a first, worse, or new headache; a patient over age 50; papilledema (optic disc swelling secondary to increased intracranial pressure); neck stiffness that worsens with movement or physical activity; changes in level of consciousness; and sudden onset or thunderclap headache. Other red flags include a worsening pain pattern, pain over the temporal artery, headache in the presence of fever or signs of systemic illness, and various focal neurologic symptoms that aren’t typical of a patient’s aura. Although routine diagnostic scanning isn’t recommended, patients presenting with red flag symptoms may require radiologic tests.
With no specific test for migraine, focus on a thorough physical assessment and history to rule out secondary headaches. Begin by excluding red flags and symptoms of other headache types. Red flags include a patient reporting a first, worse, or new headache; a patient over age 50; papilledema (optic disc swelling secondary to increased intracranial pressure); neck stiffness that worsens with movement or physical activity; changes in level of consciousness; and sudden onset or thunderclap headache. Other red flags include a worsening pain pattern, pain over the temporal artery, headache in the presence of fever or signs of systemic illness, and various focal neurologic symptoms that aren’t typical of a patient’s aura. Although routine diagnostic scanning isn’t recommended, patients presenting with red flag symptoms may require radiologic tests.
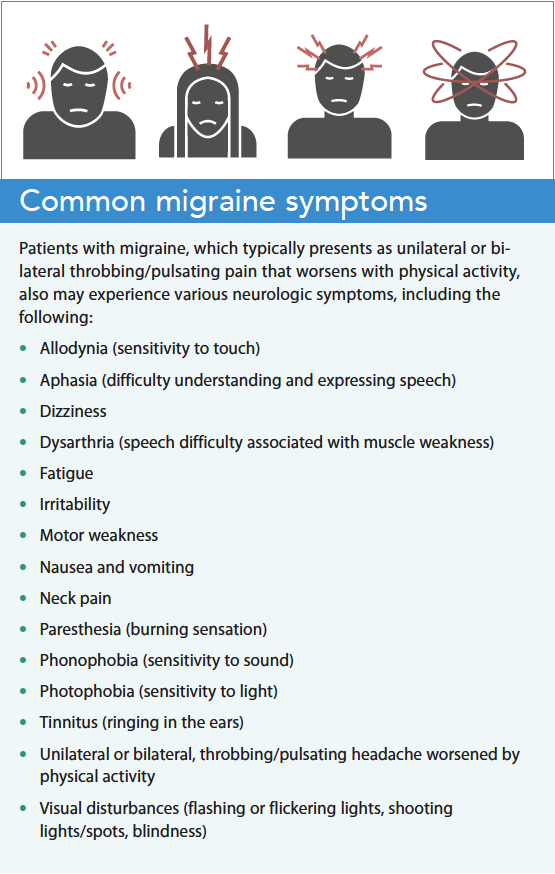
Most patients with migraine experience excruciating headache pain, which they frequently describe as unilateral and throbbing. Associated symptoms include nausea, photophobia, phonophobia, and allodynia. Patients with migraine may report several headache days per month, with some lasting 4 to 72 hours each. The American Headache Society has created specific criteria to help providers diagnose migraine (americanheadachesociety.org/wp-content/uploads/2021/01/AHS-First-Contact-Diagnosing-Migraine-.pdf).
The American Headache Society estimates that one-third of patients with migraine experience an aura or focal neurologic symptom (seeing spots, sparkles, or flashing lights) before the migraine pain begins. Some with aura have physical sensations such as numbness or paresthesia (muscle weakness). When patients present with these symptoms, assess whether the type of aura the patient experiences mimics any red flag disorders. Don’t attribute a focal neurologic complaint to migraine unless the patient has experienced it before. If they haven’t, the patient requires a focused neurologic exam. After ruling out red flags or life-threatening headaches, focus on treating pain and associated symptoms. (See Common migraine symptoms.)
Ms. Browne describes her unilateral, right-sided headache as throbbing. She also reports increased pain associated with bright light and that she feels nauseous but hasn’t vomited. She says that her 10/10 pain worsens with physical activity and movement but that she’s not experiencing allodynia (pain associated with touch). She hasn’t had an aura or other focal neurologic symptoms or change in her level of consciousness. She describes this headache as typical, and that she has headaches 10 to 12 days per month. Ms. Browne reports sleeping only 4 to 5 hours per night because of school stress. Findings during the neurologic exam are within normal limits.
Acute treatment
After the provider eliminates a secondary cause and makes a migraine diagnosis, prioritize acute treatment of symptoms. According to the American Headache Society, important goals include fast and maintained relief of pain and associated symptoms, a return to functional ability, and a minimal need for additional medications or repeat dosing. Suboptimal treatment can result in increased pain, associated incapacitation, and disease progression.
The American Headache Society recommends offering all patients with a migraine diagnosis acute pharmacologic and nonpharmacologic treatment. Nonpharmacologic treatment includes highlighting the importance of improving modifiable risk factors such as stress, hydration, routine exercise, sleep hygiene, and overuse of acute medications. A migraine or headache diary can help the provider understand migraine severity. Various pharmacologic treatment options with differing routes of administration exist, many of which target presenting symptoms. For patients with nausea and vomiting, for example, the parenteral route is preferred.
For patients who don’t experience symptom relief with nonsteroidal anti-inflammatory drugs or nonopioid analgesics, providers may consider migraine-specific medications such as triptans, dihydroergotamine, ditans, and gepants. In addition, several novel therapies (including celecoxib, rimegepant, lasmiditan, remote electrical neuromodulation, and ubrogepant) have proven successful. The American Headache Society has created criteria for the use of these novel therapies ( headachejournal.onlinelibrary.wiley.com/doi/10.1111/head.14153 ). Treat associated symptoms, such as nausea and vomiting, with appropriate medications to promote comfort. For patients with recurring or chronic migraine, preventive medications prescribed by their primary care provider or a migraine specialist may help reduce ED visits.
Nursing implications
Focus your nursing care on patient comfort and education. Administer prescribed medications while closely monitoring patients for adverse reactions or side effects. When possible, provide the patient with a stimulation-free environment to reduce photophobia and phonophobia.
Talk with the patient about the importance of timely treatment and explain that delayed treatment may result in an inadequate response to therapy. Educate the patient about avoiding medication overuse, which can lead to re-hospitalization. Provide information about avoiding triggers, using newly prescribed medications, and taking steps to reduce stress and improve sleep. Recommend that the patient keep a headache diary to help guide future treatment, and counsel the patient to seek outpatient follow-up care with a migraine specialist.
You create a low-stimulus environment for Ms. Browne by dimming the lights and closing the door to her room. The provider orders sumatriptan (6 mg) subcutaneously as well as metoclopramide (10 mg I.V.) for inpatient acute treatment of migraine and nausea. After 1 hour, Ms. Browne reports her pain as 4/10 with no nausea. At discharge, the provider prescribes ubrogepant for acute outpatient treatment, and you advise Ms. Browne to follow up with her primary care provider for ongoing migraine management.
It takes a team
Migraine headache, a global burden that increases functional disability, accounts for millions of annual hospital visits. Migraine presents with debilitating headache pain and various associated symptoms, making timely acute treatment vital for patient comfort. Because no specific tests for migraine exist, a thorough health history and assessment guide diagnosis. The nurse’s role in care management includes patient education, acute treatment administration, and patient comfort. Migraine specialists can aid ongoing care. This complex condition, which isn’t just a headache, requires a team of providers to ensure optimal care.
*Name is fictitious.
Dr. Cory Wilbanks is a board certified AGACNP and FNP. He currently serves as the chief operating officer and nurse practitioner at Pro Health Clinic in Memphis, Tennessee.
American Nurse Journal. 2023; 18(5). Doi: 10.51256/ANJ052318
References
Ailani J, Burch RC, Robbins MS. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache. 2021;61(7):1021-39. doi:10.1111/head.14153
American Migraine Foundation. The facts about migraine. March 28, 2019. americanmigrainefoundation.org/resource-library/migraine-facts
Ceriani CEJ, Wilhour DA, Silberstein SD. Novel medications for the treatment of migraine. Headache. 2019; 59(9):1597-1608. doi:10.1111/head.13661
Goadsby PJ. Headache. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson JL, eds. Harrison’s Principles of Internal Medicine. 21st ed. New York, NY: McGraw-Hill; 2022.
Goadsby PJ. Migraine and other primary headache disorders. In: Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson JL, eds. Harrison’s Principles of Internal Medicine. 21st ed. New. York, NY: McGraw-Hill; 2022.
Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;
38(1):1-211. doi:10.1177/0333102417738202
Schramm S, Tenhagen I, Schmidt B, et al. Prevalence and risk factors of migraine and non-migraine headache in older people—Results of the Heinz Nixdorf Recall study. Cephalalgia. 2021;41(6):649-64. doi:10.1177/0333102420977183
Wootton RJ, Wippold II FJ, Whealy MA. Evaluation of headache in adults. UpToDate; August 12, 2021.
Yang S, Orlova Y, Lipe A, et al. Trends in the management of headache disorders in US emergency departments: Analysis of 2007–2018 National Hospital Ambulatory Medical Care Survey data. J Clin Med. 2022;11(1401):1401. doi:10.3390/jcm11051401
Key words: migraine, headache, migraine triggers, migraine auras


















