
Quick action ensures prompt diagnosis and treatment.
- Metformin-associated induced lactic acidosis (MALA) is a life-threatening condition that requires prompt, aggressive management.
- Early recognition of signs and symptoms of toxicity saves lives.
Macy Wilson*, a 48-year-old woman, is admitted to the hospital with diffuse abdominal pain that started 24 hours earlier. She describes the pain as coming in waves every 20 minutes, and intensifying. She also reports headache, nausea, dry heaving, bloating, and constipation. When Ms. Wilson was 35, she had a Roux-en-Y gastric bypass and lost over 150 pounds in the first 18 months after surgery.
History and assessment
Ms. Wilson’s vital signs are BP 120/80 mmHg, HR 100 bpm, RR 22 breaths per minute, and temperature 99.0° F (37.2° C). Her breathing is regular but slightly labored due to pain, which Ms. Wilson rates as 9/10 on a visual analog scale. When you assess her abdomen, you find it slightly distended, tympanic to percussion with tinkling auscultated bowel sounds, and diffusely tender to palpation.
Two hours after admission, Ms. Wilson, while drinking contrast fluid in preparation for a computed tomography scan of the abdomen and pelvis, becomes restless. She then screams out in pain, runs to the bathroom, forcefully vomits, and doubles over in pain.
You help Ms. Wilson back to her bed and take her vital signs. Her HR is 140 bpm and her BP is 90/50 mmHg. Her abdomen is distended and taut, she rates her pain as 25/10, and she’s pale and diaphoretic. Recognizing that Ms. Wilson is decompensating, you call the rapid response team (RRT). While waiting for their arrival, you start I.V. access in the left arm and administer pain medication prescribed on admission. You then place the patient on her side and apply cool compresses to her forehead. You ask the unit secretary to page the gastroenterologist and surgeon on call.
On the scene
The RRT secures a 12-lead ECG, starts an I.V. in the right arm with lactated ringers, draws blood for labs, and places a nasogastric tube for decompression. They also perform a bedside ultrasound scan of Ms. Wilson’s abdomen, which reveals a nonspecific dilated fluid-filled bowel segment. The RRT accompanies the patient to radiology for a CT scan, which shows a target sign (forward moving of the bowel by peristalsis prolapses into another bowel segment) characteristic for intussusception.
Education
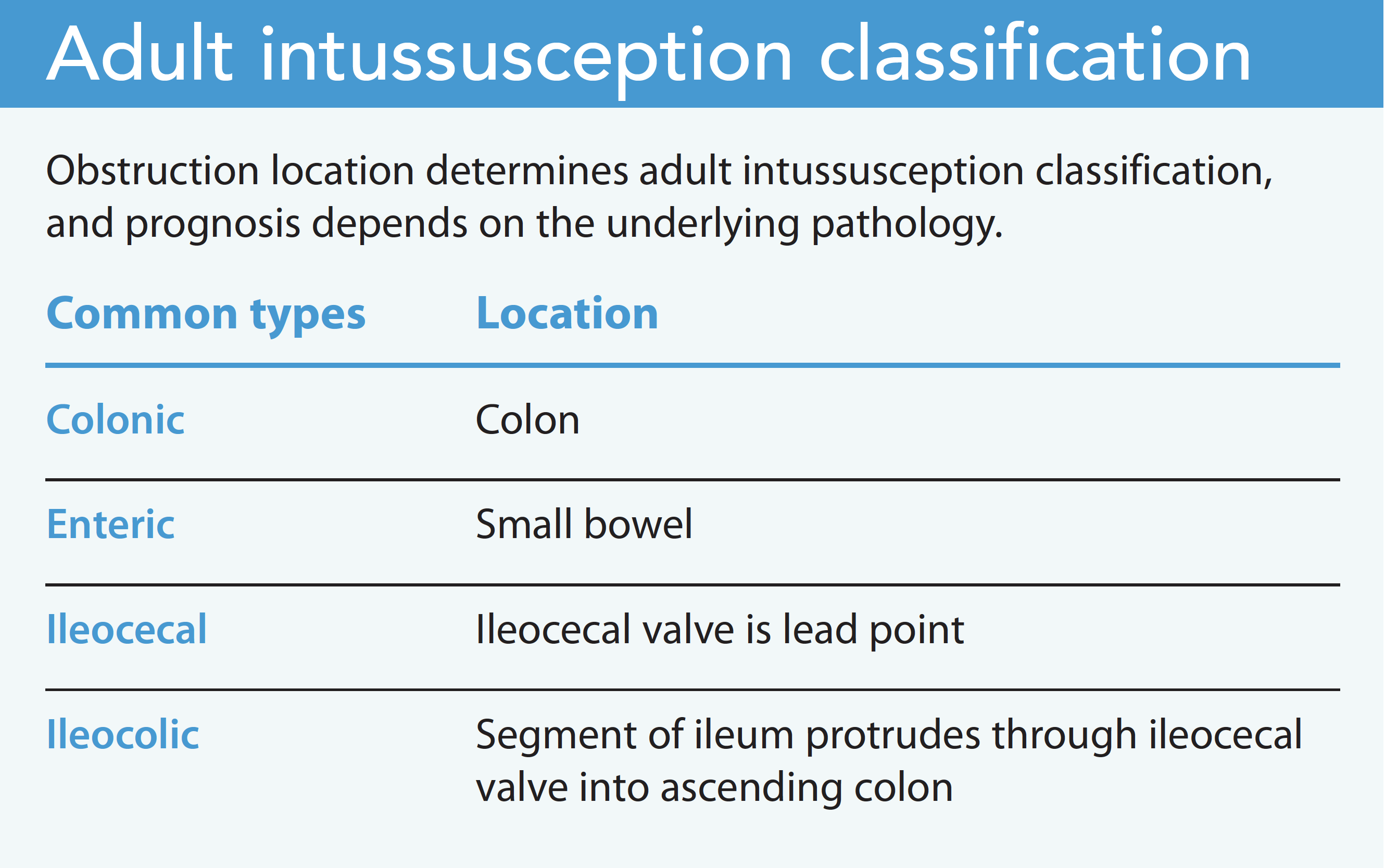
Intussusception occurs when a section of bowel slips into the lumen of an adjacent segment, causing obstruction, inflammation, and ischemia. It’s rare in adults and typically associated with malignancy, adhesions, or infection.
In Ms. Wilson’s case, abdominal adhesions and past surgery resulted in the intussusception. The omentum’s supportive structure became lax, which created areas of weakness.
Although surgical resection is the most common treatment in adults, some advocate for reducing the area first to avoid potential perforation, release of cancerous cells, or tissue destruction. If intussusception is secondary to an inflammatory process, such as Crohn’s or celiac disease, resection may not be necessary. Healing requires treating the underlying condition.
Outcomes
After laparoscopic release of the intussusception and 3 days of clear liquids, Ms. Wilson advances to pureed foods (no more than 4 ounces per meal). She experiences constipation, which requires 3 days of polyethylene glycol 3350. She’s then discharged home, and her provider prescribes daily docusate sodium to prevent constipation. Your quick action ensured a good outcome for Ms. Wilson.
*Name is fictitious.
Donna J. Purviance is a DNP at Union Medical Group in Terre Haute, Indiana.
References
Aydin N, Roth A, Misra S. Surgical versus conservative management of adult Intussusception: Case series and review. Int J Surg Case Rep. 2016;20:142-6. doi:10.1016/j.ijscr.2016.01.019
Hadid T, Elazzamy H, Kafri Z. Bowel intussusception in adults: Think cancer! Case Rep. Gastroenterol. 2020;14(1):27-33. doi:10.1159/000505511
Kim KH. Intussusception in adults: A retrospective review from a single institution. Open Access Emerg Med. 2021;13:233-7. doi:10.2147/OAEM.S313307
Lu T, Chng Y. Adult intussusception. Perm J. 2015;19(1):79-81. doi:10.7812/TPP/14-125
American Nurse Journal. 2022; 27 (11). Doi: 10.51256/ANJ112219


















