
Improve adherence for all acute care nurses.
- A quality-improvement project team performed direct observational audits of anesthesia clinicians’ compliance with aseptic technique during I.V. medication administration.
- Despite improvements in infection prevention behaviors 1- and 3-months after a multifaceted educational program, overall adherence rates remained below the expected target.
- Nursing leadership should consider ongoing quality improvement efforts to increase and maintain compliance with infection prevention practices.
Learning Objectives
- Discuss the development of standardized education programs that include I.V. aseptic techniques and the impact on outcomes.
- Describe how audit and feedback strategies can prompt behavioral change and adherence with aseptic technique targets.
- Discuss the importance of ongoing education efforts to improve adherence to safe injection practices to decrease healthcare-associated bloodstream infections.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 11/1/26
I.V. push medications: An evidenced-based practice guide
Myths of I.V. push administration
Central lines: Recognizing, preventing, and troubleshooting complications
According to Rupp and colleagues, over 300 million peripheral I.V. (PIV) catheters are placed annually. Despite their ubiquity across healthcare settings, I.V. injections continue to play a role in disease transmission. A study by Wax and colleagues found that each year in the United States over 500,000 healthcare-associated bloodstream infections are attributed to I.V. catheters, including central and peripheral lines. These infections lead to increased morbidity and mortality risk, increased length of stay, additional antibiotic administration, potential adverse effects of antibiotic therapy, and higher healthcare system costs. A study by Zhu and colleagues determined that each healthcare-associated bloodstream infection had an average excess cost of $27,668. (See Contamination sources.)
Contamination sources
Unsafe injection practices, including needle reuse and I.V. access port or medication vial contamination, can contribute to bloodstream infection risk. The operating room (OR) serves as a well-known source of pathogen transmission due to its fast pace, abundance of potentially infectious materials, and frequent disruptions to the skin. In the perioperative setting, most medication—including anesthesia—is administered intravenously. Large quantities of antibiotic-resistant strains of bacteria have been cultured from I.V. access lines and OR surfaces, and poor adherence to aseptic technique by anesthesia clinicians may be a contributing factor.
Robinson and colleagues found that I.V. access stopcocks may be contaminated with pathogens, including Staphylococcus aureus, in up to 32% of surgical cases, with OR surfaces and anesthesia providers’ hands as the main source of this contamination. The contamination rates found in this 2019 study were comparable to findings in prior studies, demonstrating that little to no improvement has occurred in perioperative contamination rates within the past several years.
Aseptic technique
To prevent the risk of healthcare-associated infections, the Infusion Nurses Society, the Institute for Safe Medication Practices, the Association of periOperative Registered Nurses, and the Compendium of Strategies to Prevent Healthcare-Associated Infections advocate for the use of aseptic technique before I.V. medication administration. Aseptic technique is defined as the use of hand hygiene as well as the disinfection of vascular access devices (scrub the hub practices) before administering I.V. medications. Current guidelines recommend using an alcohol or chlorhexidine-based disinfectant product.
Frequently, lack of compliance with aseptic technique results from a knowledge deficit. Studies support using education and re-education to improve disinfection adherence. After administering knowledge assessments to various critical care nurses and physicians, a cross-sectional study by Al Qadir and Hani determined that many clinicians didn’t know how to prevent catheter-associated bloodstream infections. The authors recommended developing standardized educational training programs and performing regular observation and evaluation of aseptic technique adherence.
Duke University Hospital targeted aseptic technique adherence during perioperative I.V. medication administration for quality improvement (QI). Adherence rates among anesthesia clinicians was less than 30%, lower than the internal target of 95%. The QI project aimed to evaluate the efficacy of a multifaceted educational program in increasing compliance with aseptic technique by anesthesia clinicians, including physician anesthesiologists and certified registered nurse anesthetists (CRNAs). The specific goals included increasing adherence with hand hygiene before medication administration, I.V. access disinfection, dry time after disinfection, and improving anesthesia clinicians’ knowledge of disinfection best practices.
The project
We conducted this QI project in a 957-bed university hospital, which is part of a large, academic health system. The hospital contains over 51 ORs and performs over 74,000 procedures each year. The project included a convenience sample of CRNAs and physician anesthesiologists.
We evaluated aseptic technique via direct observation audits, including three components: hand hygiene to assess the use of alcohol-based hand sanitizer before I.V. medication administration; scrub time to assess whether the clinician scrubbed the I.V. access device for at least 15 seconds with isopropyl alcohol; and dry time to assess whether the clinician allowed the device to dry for at least 15 seconds before access. We collected data using a template that included provider type, surgical case type, and direct observations of aseptic technique. Auditing occurred in both the preoperative areas, where anesthesia clinicians typically administer an I.V. anxiolytic, as well as in the ORs at different points within the case (induction, maintenance, and emergence). We didn’t perform audits on any non-OR anesthesia services, such as magnetic resonance imaging or during obstetric, trauma, or emergency cases.
The project audited only the first instance of I.V medication administration in each surgery or procedure for one patient (not the entirety of a clinical day or surgery). Clinicians were audited only once per audit day; however, we may have audited the same clinician more than once during the course of data collection, as provider identifiers weren’t gathered. To protect the surreptitious nature of data collection and prevent bias, we withheld feedback for nonadherence.
After collecting baseline adherence data (from January through March 2022), we implemented a multifaceted educational program, which included educational outreach visits, visual reminders, and audit and feedback during April 2022. Chan and colleagues noted that educational outreach visits, which involve a trained clinician providing specific education, can help modify the behavior of healthcare professionals. Our educational outreach visits included an informational booth in the hallway separating the two sides of the OR unit. During these visits, clinicians could receive education related to a review of aseptic technique, recommended scrub and dry times, and a visual demonstration with a Glo Germ propofol solution to simulate I.V. line contamination. An educational presentation with similar information was delivered at a CRNA staff meeting. We emailed an electronic version of the presentation to the CRNA and anesthesiology departments, embedded within a Qualtrics link, so clinicians could attest that they’d viewed the presentation. Based on the sign-in sheets for the staff meeting presentation and outreach visits, 55 clinicians received the education.
According to Giguère and colleagues, visual reminders and printed educational materials also effectively improve behaviors of healthcare professionals. We posted images from the simulated propofol contamination, reminders of recommended scrub and dry times, images of pathogens at various intervals of scrubbing, and laminated icon cues on the CRNA educational whiteboard and distributed them to several ORs. We placed the icons above the anesthesia machines as well as on the Pyxis machines where medications are dispensed and drawn up.
Because several studies have noted the use of audit and feedback as an effective strategy to modify and sustain behavioral change, we shared adherence data with the clinicians via run charts so they could see that they were below the 95% compliance target. We incorporated pre-intervention adherence data into the educational outreach visits and staff meeting presentation; we also emailed them to the anesthesia department. During post-implementation data collection (May 2022 and from July through August 2022), we posted run charts and emailed live adherence rates every 2 weeks to anesthesia clinicians, which allowed them to track their progress over time.
According to Paul and colleagues and Plemmons and colleagues, knowledge of infection risks and best practice guidelines directly correlates with improved adherence. To assess knowledge of best practice infection prevention behaviors, we distributed pre- and postimplementation assessments and surveys to the anesthesia department. The anonymous and voluntary questionnaire included three multiple-choice questions to assess knowledge of best practice guidelines and four 4-point Likert scale questions to evaluate infection-prevention behaviors. An open-ended text field allowed anesthesia clinicians to note perceived barriers to completing aseptic technique practices before medication administration.
The results
Power analysis revealed the need for a minimum of 128 audits (64 pre- and 64 postimplementation). We analyzed data using chi-square tests and run charts and surveys using Fisher’s Exact and Mann-Whitney tests. We completed a total of 260 audits (pre-implementation n=95; 1-month post-implementation, n=85; 3-months post-implementation, n=80). Most audits were conducted on CRNAs (n=134, 51.5%) during general surgery cases (n=73, 28.1%) and orthopedic surgery cases (n=42, 16.2%).
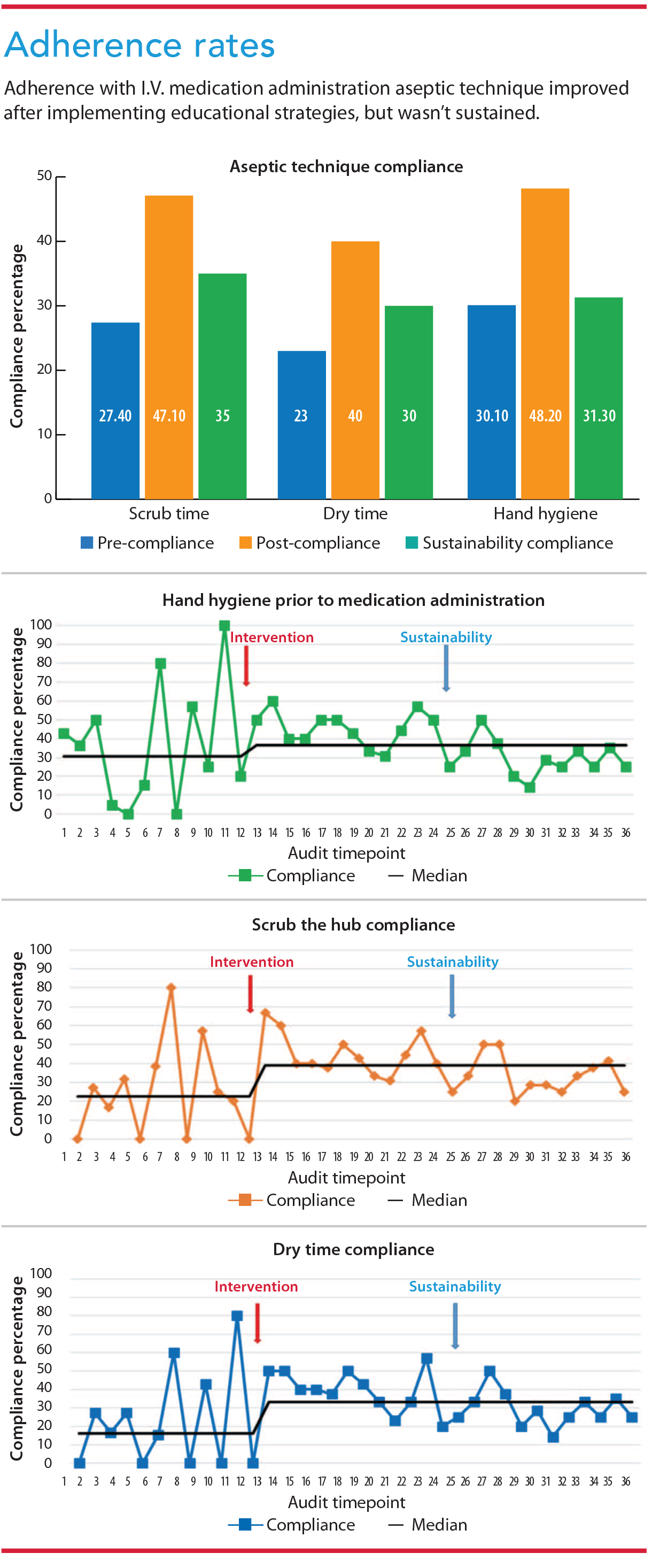 Median adherence increased from 30.7% at baseline to 36.4% after the intervention. Using statistical analyses, adherence with hand hygiene before medication administration significantly improved from a mean of 30.1% pre-implementation to 48.2% 1-month after implementation (P=.022) but declined to 31.3% after 3 months. Median adherence with scrub the hub practices increased from 22.5% at baseline to 38.8% after the intervention. Using statistical analyses, overall scrub time adherence increased significantly from 27.4% pre-implementation to 47.1% 1 month after implementation (P=.022) but declined to 35% after 3 months.
Median adherence increased from 30.7% at baseline to 36.4% after the intervention. Using statistical analyses, adherence with hand hygiene before medication administration significantly improved from a mean of 30.1% pre-implementation to 48.2% 1-month after implementation (P=.022) but declined to 31.3% after 3 months. Median adherence with scrub the hub practices increased from 22.5% at baseline to 38.8% after the intervention. Using statistical analyses, overall scrub time adherence increased significantly from 27.4% pre-implementation to 47.1% 1 month after implementation (P=.022) but declined to 35% after 3 months.
Median adherence with dry time after scrubbing the hub increased from 16% at baseline to 33.3% after the intervention. Using statistical analyses, dry time adherence increased significantly from 23.2% pre-implementation to 40% 1 month after (P=.05) but declined to 30% after 3 months. (See Adherence rates.)
Small and variable sample sizes made it impossible to draw any statistically significant conclusions regarding differences in adherence and knowledge based on professional role (CRNA vs. MD) or adherence during certain surgical cases (for example, pediatric vs. ear, nose, and throat). Forty-eight clinicians completed the pre-implementation knowledge survey and 13 completed the postimplementation survey. We saw improvements in knowledge postimplementation, but they weren’t significant. (View survey responses)
What we learned
This project showed improvements in aseptic technique during I.V. medication administration after implementing a multifaceted educational program, with the most significant improvements occurring 1 month after implementation. Despite these improvements, adherence rates didn’t reach the hospital’s internal target of 95%. Our results were similar to the findings seen by Plemmons and colleagues and Paul and colleagues. As more time elapsed postimplementation, adherence improvements became less robust. It’s unclear why hand hygiene adherence decreased more than the other audit criteria, as hand sanitizer locations and availability were consistent throughout the data collection period.
Anesthesia clinicians identified several barriers to aseptic technique adherence, including production pressure, focus on more immediate patient safety concerns, and lack of explicit and unequivocal data linking infection rates to infection prevention behaviors. As noted in implementation science literature, fundamental changes to practice habits are difficult to implement, particularly with experienced clinicians, and habitual sustainability remains a challenge.
Adapting interventions and implementation strategies to the local level may help facilitate sustainability of these important evidence-based practices. To improve future adherence, infection prevention teams may consider persistent and extended education, incorporation of peer-to-peer accountability, financial incentives linked to adherence, as well as consultation with biomedical engineering, pharmacy, and technology to develop a contactless I.V. line.
Survey responses
Anesthesiology clinicians participated in a voluntary and anonymous survey pre- and postimplementation of the quality improvement project. We were limited by the few responses to the postimplementation survey.
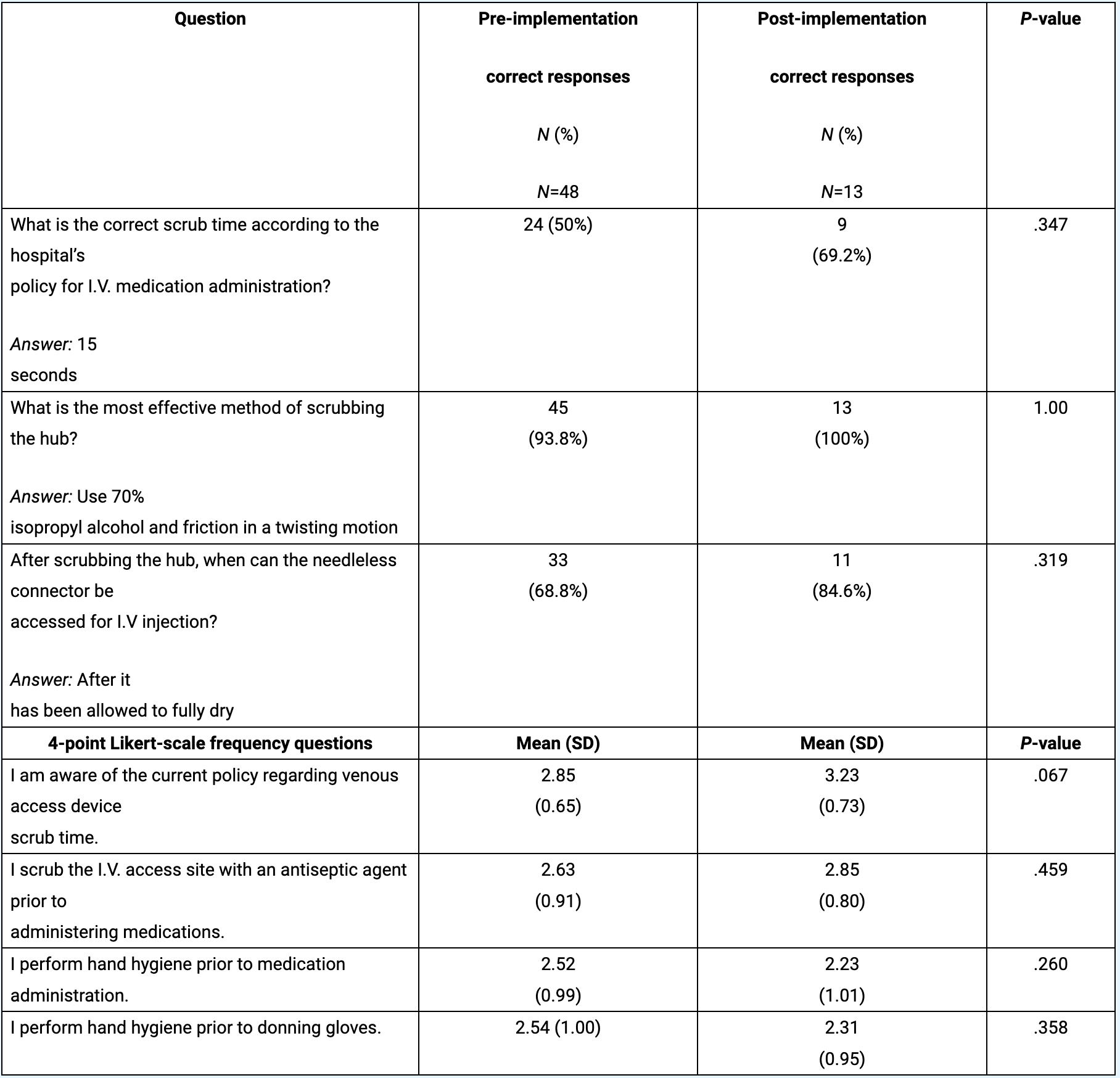
Likert-scale: 1=strongly disagree to 4=strongly agree, or 1=never, 2=rarely, 3=sometimes, 4=every time
Implications for nursing practice
We recommend that ORs institute ongoing education and audit and feedback strategies to keep aseptic technique practices at the forefront of clinicians’ minds. Education should reiterate friction disinfection of the I.V. access device before use, and that the system should be kept closed with syringes or caps to reduce the risk of pathogen entry. These steps can occur during preoxygenation, before induction, if time constraints present a concern.
Beyond the OR setting, acute and critical care RNs also should practice aseptic technique when administering I.V. medications. Nurse leaders and clinical educators should consider similar interventions in these units. For example, educational outreach visits, frequent reiteration of recommended scrub and dry times, visual reminders, and audit and feedback if resources permit. A review by Fithriyyah and Aulawi suggests using mobile phone reminder applications to engage and educate nursing staff in catheter-associated bloodstream infection prevention. Nurses also should consider assessing their workspaces regularly to ensure the availability of alcohol-based hand sanitizers and alcohol pads in areas of most need. The Infusion Nurses Society recommends initial evaluation of nurses for vascular access competency followed by regular and ongoing review as well as multimodal education for both nurses and nurse leaders.
Limitations
Conducting this project at one institution and data collection by one individual hindered generalizability of results. Although most audit data were obtained via observations from the sterile core areas or outside of the ORs to mitigate the Hawthorne effect (alteration of study subject behavior due to awareness of observation), some clinicians may have known they were observed, thus creating bias. The educational period lasted only 1 month; additional education and resources over a longer period may have yielded better results. Sustainability data collected in July and August may have been impacted by the hiring of a new cohort of anesthesiology residents, who may have been audited postimplementation and didn’t receive the educational intervention. In addition, the small number of completed postimplementation surveys precluded any statistically significant conclusions regarding knowledge improvement.
Ongoing education
Improvements in aseptic technique among anesthesia clinicians during I.V. medication administration were seen following this project’s multifaceted educational program. However, continued improvement remains in question. Clinicians and leaders should consider ongoing QI efforts to increase and maintain adherence with aseptic technique and infection prevention practices in the OR and throughout acute and critical care units.
Lauren Gilmore is a CRNA at Inova Hospital in Falls Church, Virginia. Virginia C. Simmons, is a clinical professor at Duke University School of Nursing in Durham, North Carolina. Jessica Seidelman is an associate professor of medicine at Duke University School of Medicine, an infectious disease physician in the Duke Center for Antimicrobial Stewardship and Infection Prevention at Duke University Medical Center, and a physician in infection prevention and hospital epidemiology at Duke University Hospital. Staci S. Reynolds is associate clinical professor at Duke University School of Nursing.
American Nurse Journal. 2023; 18(11). Doi: 10.51256/ANJ112306
References
Al Qadire M, Hani AM. Nurses’ and physicians’ knowledge of guidelines for preventing catheter-related blood stream infections. Nurs Crit Care. 2022;27(4):594-601. doi:10.1111/nicc.12577
Association of periOperative Registered Nurses. Guideline summary: Medication safety. AORN J. 2018;107(4):489-94. doi: 10.1002/aorn.12096
Chan WV, Pearson TA, Bennett GC, et al. ACC/AHA special report: Clinical practice guideline implementation strategies: A summary of systematic reviews by the NHLBI Implementation Science Work Group: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;69(8):1076-92. doi:10.1016/j.jacc.2016.11.004
Fithriyyah YN, Aulawi K. Using mobile phone applications in engaging nurses for preventing healthcare-associated infections: A systematic review. Nurs Pract Today. 2022;9(2):84-101. doi:10.18502/npt.v9i2.8892
Giguère A, Zomahoun HTV, Carmichael PH, et al. Printed educational materials: Effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2020;8:CD004398. doi:10.1002/14651858.CD004398.pub4
Gorski LA, Hadaway L, Hagle ME, et al. Infusion Therapy Standards of Practice, 8th edition. J Infus Nurs. 2021;44(1S):S1-224. doi:10.1097/NAN.0000000000000396
Hailemariam M, Bustos T, Montgomery B, Barajas R, Evans LB, Drahota A. Evidence-based intervention sustainability strategies: A systematic review. Implement Sci. 2019;14(57). doi: 10.1186/s13012-019-0910-6
Institute for Safe Medication Practices. ISMP Safe Practice Guidelines for Adult IV Push Medications. 2015. ismp.org/sites/default/files/attachments/2017-11/ISMP97-Guidelines-071415-3.%20FINAL.pdf
Paul ET, Kuszajewski M, Davenport A, Thompson JA, Morgan B. Sleep safe in clean hands: Improving hand hygiene compliance in the operating room through education and increased access to hand hygiene products. Am J Infect Control. 2019;47(5):504-8. doi:10.1016/j.ajic.2018.10.021
Plemmons MM, Marcenaro J, Oermann MH, Thompson J, Vacchiano CA. Improving infection control practices of nurse anesthetists in the anesthesia workspace. Am J Infect Control. 2019;47(5):551-7. doi:10.1016/j.ajic.2018.12.009
Reynolds SS, Woltz P, Keating E, et al. Results of the CHlorhexidine gluconate bathing implementation intervention to improve evidence-based nursing practices for prevention of central line associated bloodstream infections Study (CHanGing BathS): A stepped wedge cluster randomized trial. Implement Sci. 2021;16(1):45. doi:10.1186/s13012-021-01112-4
Robinson ADM, Dexter F, Renkor V, Reddy S, Loftus RW. Operating room PathTrac analysis of current intraoperative Staphylococcus aureus transmission dynamics. Am J Infect Control. 2019;47(10):1240-7. doi:10.1016/j.ajic.2019.03.028
Rupp ME, Tandon H, Danielson P, Cavalieri RJ, Sayles H. Peripheral intravenous catheters – “They Don’t Get No Respect.” Open Forum Infect Dis. 2017;4(suppl 1):S636. doi:10.1093/ofid/ofx163.1689
Wax DB, Shah A, Shah R, Lin HM, Katz D. Efficacy and usability of a novel barrier device for preventing injection port contamination: A pilot simulation study. Anesth Analg. 2020;130(3):e45-8. doi:10.1213/ANE.0000000000004235
Yokoe DS, Anderson DJ, Berenholtz SM, et al. A compendium of strategies to prevent healthcare-associated infections in acute care hospitals: 2014 updates. Infect Control Hosp Epidemiol. 2014;35(8):967-77. doi:10.1086/677216
Zhu S, Kang Y, Wang W, Cai L, Sun X, Zong Z. The clinical impacts and risk factors for non-central line-associated bloodstream infection in 5046 intensive care unit patients: An observational study based on electronic medical records. Crit Care. 2019;23(1):52. doi:10.1186/s13054-019-2353-5
Key words: aseptic technique, anesthesia I.V. medication, peripheral intravenous catheter, central I.V. lines, hand hygiene, healthcare-associated bloodstream infections, scrub-the-hub


















1 Comment. Leave new
I take these for CEU & usually read the information that I don’t usually have exposure in my work. I learn something all the time. Thanks, Lorraine