
Shining a light to reduce hospital workplace violence.
Takeaways:
- Healthcare workers are more likely to be victims of serious violence than those working in the private sector.
- Almost half of violent events that occur in the emergency are related to drug or alcohol use.
- Behavioral evaluation and addiction management nurse practices can be implemented to reduce workplace violence and improve quality of care for patients with substance use disorders.
Workplace violence isn’t part of the nursing job description, but according to the Occupational Safety and Health Administration, healthcare workers are four times more likely to experience violence than other workers in the private sector. A 2017 systematic review and meta-analysis found that 45% of emergency department (ED) violent events were related to drug or alcohol use. The Joint Commission and the American Nurses Association have issued calls to action to develop and implement strategies to protect hospital nurses and other employees from workplace violence. In addition, solutions that focus on treating and managing substance use disorder are needed.
Providence Mission Hospital, a 375-bed, Level II trauma center in Southern California, developed a nurse-led behavioral evaluation and addiction management (BEAM) team as part of its strategy to reduce workplace violence specifically related to patients with behavioral aggression and substance use disorders.
Measuring violence
In 2019, to better understand the prevalence of workplace violence at Mission Hospital, we conducted an anonymous online survey of all bedside RNs (30% responded). Violence was measured by frequency of personal experience, sources of violence (patients, coworkers, visitors), and types of violence. We also asked nurses if they completed a formal violence incident report. Of the 291 nurses who completed the survey, 86% had experienced workplace violence from a patient (67%), a patient family member (44%), or a visitor (26%). Most events (64%) were nonphysical and included name-calling, yelling, cursing, or verbal intimidation. Physical violence resulting in harm (36%) included hitting, kicking, and pushing. Although most of the respondents (65%) said they had been instructed to report abuse regardless of severity, 73% reported that they didn’t report the incident.
Beginning in 2018, nurses throughout the hospital reported difficulty caring for patients experiencing drug and alcohol withdrawal. Rapid response nurses reported an increase in the volume of patients with substance use disorders who required transfers to higher levels of care. Despite in-person education about the use of the Clinical Institute Withdrawal Assessment for Alcohol (CIWA) and the Clinical Opiate Withdrawal Scale (COWS), some nurses had difficulty managing patients experiencing aggression and agitation during acute withdrawal syndrome. Even when CIWA protocols were indicated, they weren’t consistently implemented. In addition, some physicians were unfamiliar with the COWS and with medication management for patients with opioid use disorder.
At shared governance meetings, nurses voiced concerns about
- existing policies and procedures that failed to decrease or prevent workplace violence
- using security guards to de-escalate violence rather than pre-emptive and therapeutic strategies
- the lack of knowledge for managing patients with opioid use disorder
- inconsistent and delayed use of interventions based on the CIWA protocol.
After some local substance rehabilitation centers and a sober living home began offering treatment without providing medical care, the number of ED visits by patients with acute withdrawal syndrome increased. Unidentified or unreported substance use disorders in patients admitted for a primary medical condition, elective surgery, or trauma frequently resulted in aggressive, disruptive behavior and threats to leave before completing treatment. Security personnel and psychiatric emergency team activation was ineffective for verbally de-escalating combative or violent patients. The organization needed new strategies that focused on better monitoring patients in withdrawal while safely providing care and decreasing workplace violence.
BEAM: Spotlight on solutions
The BEAM team project began with a literature review by the nurse director and nurse manager of the chemical dependency unit (CDU). The review included a study by Weinstein and colleagues stating that one-quarter of all hospitalized patients have a substance use disorder and that the practice of using security guards to de-escalate patients with behavioral issues doesn’t effectively address the underlying cause long-term. The CDU nurse director and nurse manager proposed the concept of a team of nurses trained in substance use disorder. The team would respond to behavioral escalations (Code Greys) and pre-emptively round on all in-patients at risk for drug and alcohol withdrawal.
In April 2019, a multidisciplinary team (an addiction medicine physician, critical care nurses, a tele-sepsis nurse, and clinical nurse specialists) was developed with the goal of designing and executing an evidence-based project (creating BEAM nurse qualifications, standardizing procedures, educating staff about the BEAM team, and developing process metrics and outcome measures) aimed at improving the care of patients with behavioral emergencies and substance use disorders.
Initial trial
Nurse leaders and ED staff met to prioritize educational and clinical strategies. They began with a trial placement of a CDU nurse in the ED to help identify patients with substance use disorders. During the trial, the CDU nurse educated staff about patient assessments, early interventions, and management, as well as how to facilitate patient transfers to inpatient chemical dependency programs. The CDU nurse also provided the ED nurses with educational sessions about drug and alcohol withdrawal management.
Team qualifications and education
A successful 4-month pilot with the CDU nurse led to the hospital administration’s support of a trial implementation of the nurse-led BEAM team. This specialty team of nurses trained in substance use disorder would work collaboratively with the physician director of the CDU, providing expertise to nursing staff throughout the hospital. BEAM nurse qualifications include a minimum of 5 years’ experience as a licensed RN, 2 years’ experience in chemical dependency or addiction nursing, and certification from the International Nurses Society on Addictions.
Role-specific education includes a review of BEAM nurse standardized procedures (patient assessments and appropriate protocols and interventions) to ensure all interventions are within the scope of nursing practice. California’s nurse practice act authorizes nurses to initiate certain medications, including nicotine replacement therapy (gum, lozenge, patch) and naloxone.
Team role
BEAM nurses, who have expertise in de-escalation techniques, respond to calls for assistance with combative or aggressive individuals and those who have substance use disorder and exhibit risky behaviors. These patients may demand pain medications or threaten to leave against medical advice. The team members also provide treatment referrals and suggest community resources such as Alcoholics Anonymous, Narcotics Anonymous, AL-ANON, and crisis hotlines.
BEAM nurses attend daily charge nurse huddles to identify patient consultations. All patient consultation and intervention data are logged and tracked daily. In addition, BEAM nurses work alongside nursing staff to provide coaching and ensure timely initiation of CIWA and opioid and nicotine withdrawal protocols.
Working with staff nurses
A promotional campaign announcing the BEAM team program included fliers, note pads, and pens with contact and consultation information. Patient consultations and significant interventions for behavioral issues and substance use withdrawal were quickly integrated into practice. BEAM nurses provided real-time staff education about CIWA and COWS protocols, including accurately scoring alcohol or opiate withdrawal to help decrease symptoms and reduce patient discomfort and delirium tremens.
BEAM interventions included appropriate medications, triggers for titrating medications, withdrawal symptom management, and reassurance about safe benzodiazepine dosing. As nurses were educated, they began recognizing the signs and symptoms of withdrawal sooner and promptly implementing protocols.
The BEAM effect
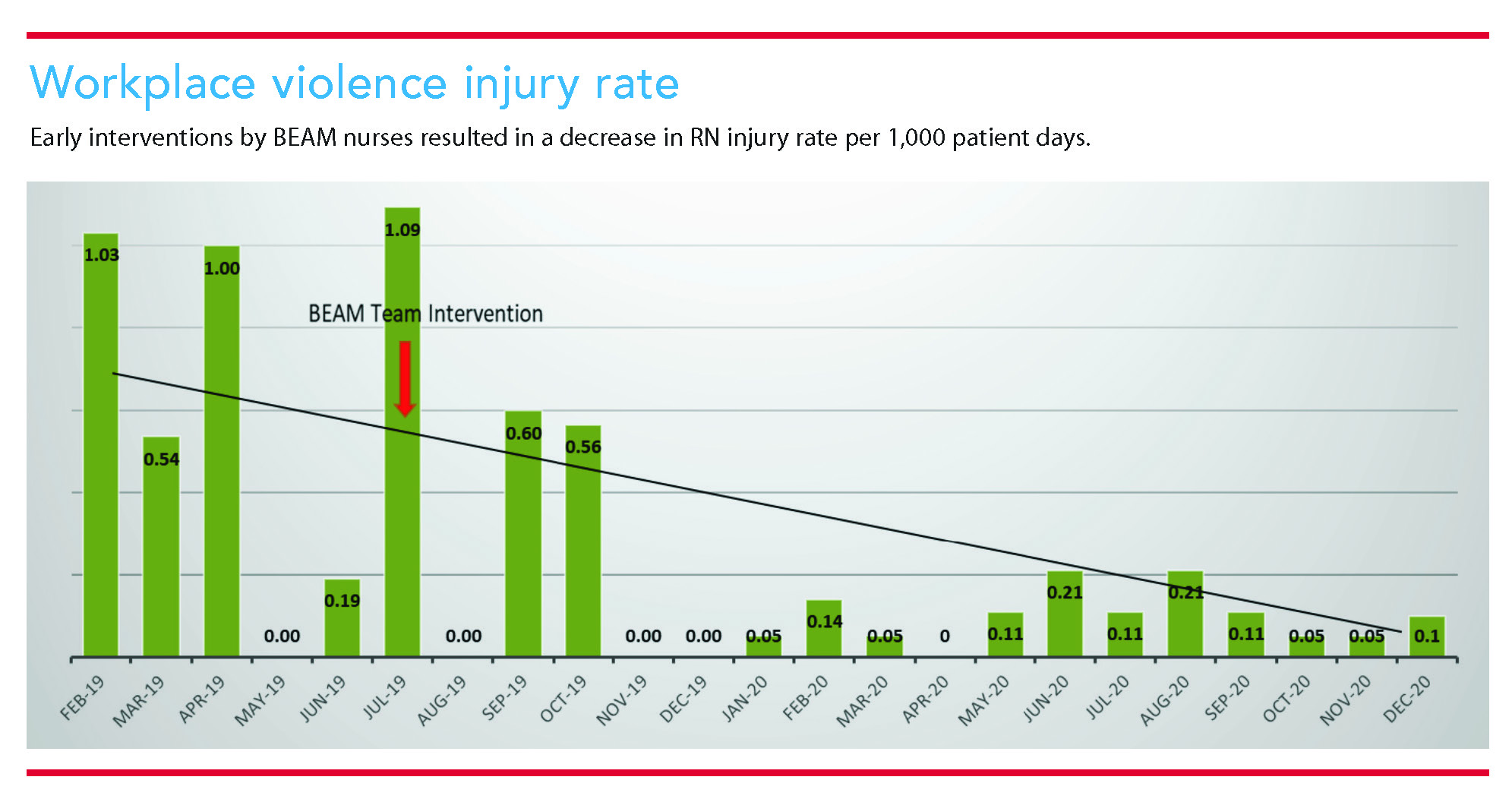
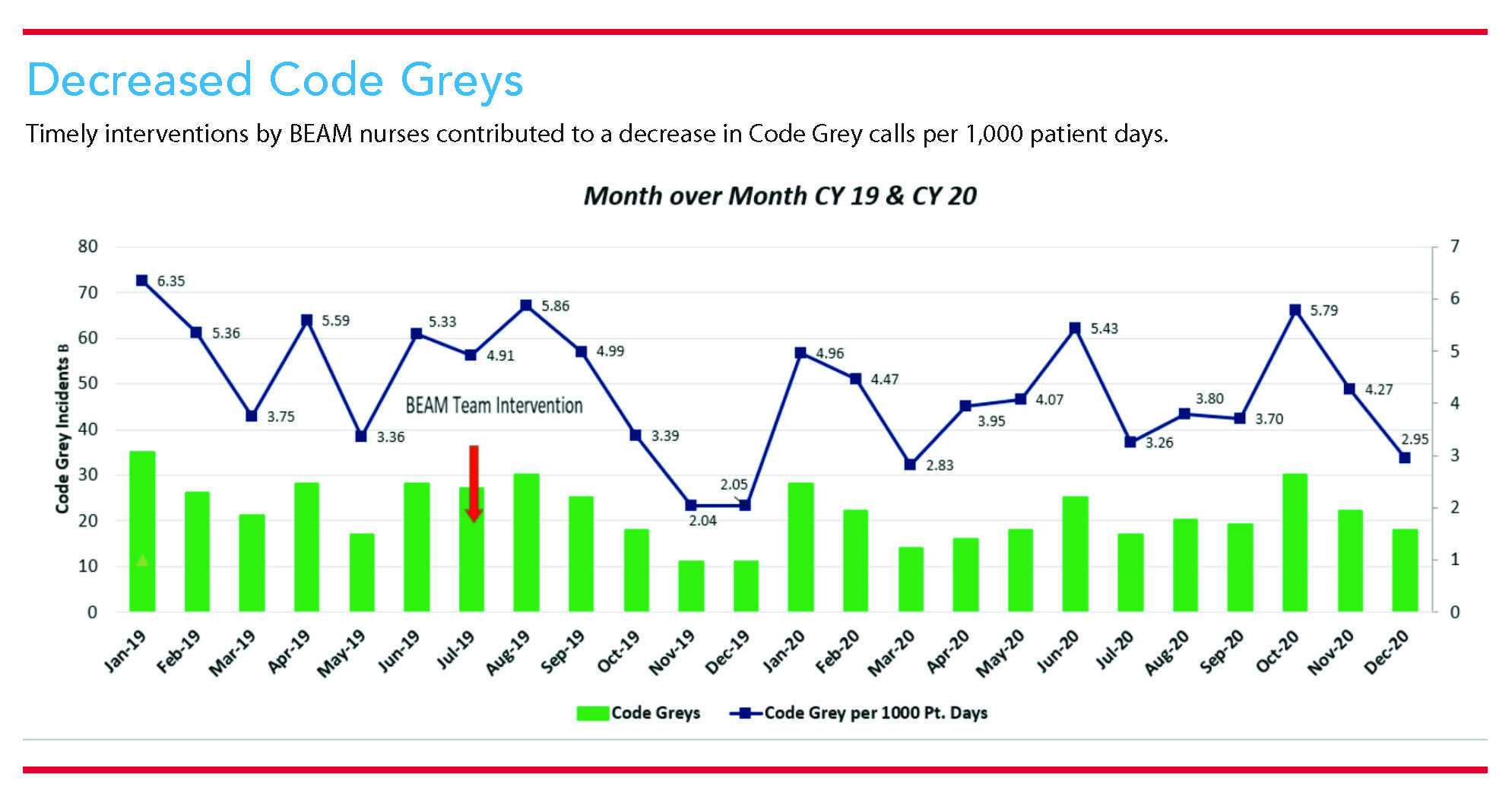
The BEAM intervention has significantly improved patient management and reduced unnecessary patient transfers to higher levels of care. The program also has improved workplace safety outcomes for clinical nurses, which supports an overall safety strategy for the hospital. The RN workplace injury rate per 1,000 patient days has decreased, as has the Code Grey rate. Increased referrals to the hospital inpatient chemical dependency program for substance use disorders have helped provide more patients with seamless and comprehensive treatment. (Access additional outcomes data at myamericannurse.com/?p=258409)
A pre- and post-intervention staff nurse survey of perceived comfort in caring for patients with behavioral and substance use disorders showed significant improvement after BEAM team program implementation. Many nurses (48.25%) reported higher levels of comfort in caring for these patients in just 3 months after implementation, compared to a baseline of 13.5%. Before program implementation, surveyed nurses reported that only 34% of patient’s substance use withdrawal symptoms were addressed during a Code Grey. After implementation, that percentage rose to 67%.
Open-ended survey responses indicated confidence and optimism about the BEAM team:
- “The BEAM RN has helped us get the medications we needed from the MD to manage the patient’s withdrawal symptoms.”
- “The implementation has reduced staff anxiety in caring for these patients and reduced workplace violence in my department.”
- “I feel more confident in managing patients with withdrawal.”
Light the way
Addressing workplace violence related to patients with substance use disorder or withdrawal requires expertise and dynamic solutions. The BEAM team provides an effective strategy for decreasing violence and consistently improving care for these patients. Other organizations can use similar programs to light the way to a safer workplace. (See Take steps to reduce workplace violence and improve care.) AN
Take steps to reduce workplace violence and improve care
Nurses and organizations can take these steps to improve the care of patients with substance use disorder and reduce the risk of workplace violence.
- Measure and report workplace violence.
- Identify patients in acute withdrawal.
- Treat patients with alcohol withdrawal syndrome using evidence-based protocols.
- Update the workplace violence prevention plan and assaultive behavior management policy, and review it at least annually.
- Identify and monitor changes that have been implemented to improve practice for patients with substance use disorders.
- Provide behavioral evaluation and addiction management training for nurses and physicians.
- Support clinical, educational, and research opportunities to prevent workplace violence and improve safe and transparent clinical practices.
- Present case studies and reviews for multidisciplinary teams.
- Report workplace violence data to hospital committees.
- Provide de-escalation training with a certified instructor.
Deanne Niedziela is the director of nursing at Providence Mission Hospital Laguna Beach in Laguna Beach, California. Diane Drake is a nurse research scientist at Providence Mission Hospital in Mission Viejo, in Mission Viejo, California. Deirdre Fitzpatrick is the chief operating officer at Hired Power in Huntington Beach, California. Jill Donaldson is a surgical clinical nurse specialist at Providence Mission Hospital Mission Viejo.
References
American Nurses Association. American Nurses Association Position Statement on Incivility, Bullying and Workplace Violence. July 22, 2015. nursingworld.org/~49d6e3/globalassets/practiceandpolicy/nursing-excellence/incivility-bullying-and-workplace-violence–ana-position-statement.pdf
Englander H, Weimer M, Solotaroff R, et al. Planning and designing the Improving Addiction Care Team (IMPACT) for hospitalized adults with substance use disorder. J Hosp Med. 2017;12(5):339-42. doi:10.12788/jhm.2736
Farrell ML. Substance use disorders: A curriculum response. OJIN. 2020;25(1). doi:10.3912/OJIN.Vol25No01PPT69
Glann JK, Carman M, Thompson J, et al. Alcohol withdrawal syndrome: Improving recognition and treatment in the emergency department. Adv Emerg Nurs J. 2019;41(1):65-75. doi:10.1097/TME.0000000000000226
Kleissl-Muir S, Raymond A, Aziz Rahman M. Incidence and factors associated with substance abuse and patient-related violence in the emergency department: A literature review. Australas Emerg Care. 2018;21(4):159-70. doi:10.1016/j.auec.2018.10.004
Nikathil S, Olaussen A, Gocentas RA, Symons E, Mitra B. Review article: Workplace violence in the emergency department: A systematic review and meta analysis. Emerg Med Australas. 2017;29(3):265-75. doi:10.1111/1742-6723.12761
Occupational Safety and Health Administration. Workplace violence. osha.gov/SLTC/workplaceviolence
Occupational Safety and Health Administration. Workplace violence in healthcare. osha.gov/healthcare/workplace-violence
Sforza T, Saavedra T, Schwebke S, et al. How some Southern California drug rehab centers exploit addiction. Orange County Register. November 5, 2018. ocregister.com/2017/05/21/how-some-southern-california-drug-rehab-centers-exploit-addiction
Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health. August 2019. samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHNationalFindingsReport2018/NSDUHNationalFindingsReport2018.pdf
U.S. Bureau of Labor Statistics. Nonfatal occupational injuries and illnesses. August 4, 2020. www.bls.gov/iif/soii-overview.htm
Virkstis K, Herleth A, Langr M. Cracks in the foundation of the care environment undermine nurse resilience. J Nurs Adm. 2018;48(12):597-9. doi:10.1097/NNA.0000000000000687
Weinstein ZM, Wakeman SE, Nolan S. Inpatient addiction consult service: Expertise for hospitalized patients with addiction problems. Med Clin North Am. 2018;102(4):587-601. doi:10.1016/j.mcna.2018.03.001
Zicko JM, Schroeder RA, Byers WS, Taylor AM, Spence DL. Behavioral emergency response team: Implementation improves patient safety, staff safety, and staff collaboration. Worldviews Evid Based Nurs. 2017:14(5):377-84. doi:10.1111/wvn.12225


















1 Comment.
I am a RN who has spent most of my nursing career in the Operating Room. In recent years I have become increasingly interested in learning about and becoming involved in Addiction and Mental Health. I have thought about lobbying in VA, but do not know much about it. What educational opportunities do you recommend for me to learn more?
I strongly believe we need more mental health care providers, better access to treatment and education to the public. I see addiction and mental health issues seen in a negative manner in our country and many with addictions and mental health issues end up in our criminal and do not receive the treatment they need. Once released back into society their problems remain as they are not addressed in the criminal system. These people need help and we don’t provide enough.
Thank you for your assistance and advice,
Lynn Robertson, MSN, BSN, CNOR