Our hospital systems’ journey to obtain Magnet® recognition led to an excellent opportunity: the chance to revamp and improve our nursing orientation program as part of the effort to achieve excellence in nursing practice. Our system consists of three hospitals that historically held separate nursing orientations—we combined them into a single, standardized orientation program.
But we didn’t just standardize our practices. We took the leap from using a passive learning lecturestyle approach to implementing active, innovative learning strategies—giving our nurses a better chance to succeed at patient care.
Finding solutions
We were two nurse educators responsible for three hospitals. Together, we identified challenges to combining resources and standardizing the orientation program, then brainstormed ways to address these challenges.
To coordinate multiple schedules at three different locations, we created a master orientation schedule and designated one educator as the main contact for scheduling. We selected the main campus as the location for orientation since the simulation lab, guest speakers, and majority of newly hired nursing staff were based there.
As the project progressed, we addressed scheduling glitches and the need for more instructors. We also enhanced coordination between departments. For example, based on feedback from new hires, we combined a half-day class in patient handling taught by the physical therapy department with a half-day class in electronic health records taught by the informatics department into a 1-day session. This helped decrease costs associated with travel and time spent in orientation.
We discovered that hospitals in our system didn’t always schedule time for nursing staff to attend orientation. We worked with human resources and nursing leadership to help make orientation for new hires standard practice across the health system.
Life after death by PowerPoint
Once we completed plans for combining all three hospitals’ orientation programs, we reviewed the curriculum for the 2-day nursing orientation. We wanted to change the orientation format from lecture—death by PowerPoint—to a learner-centered approach.
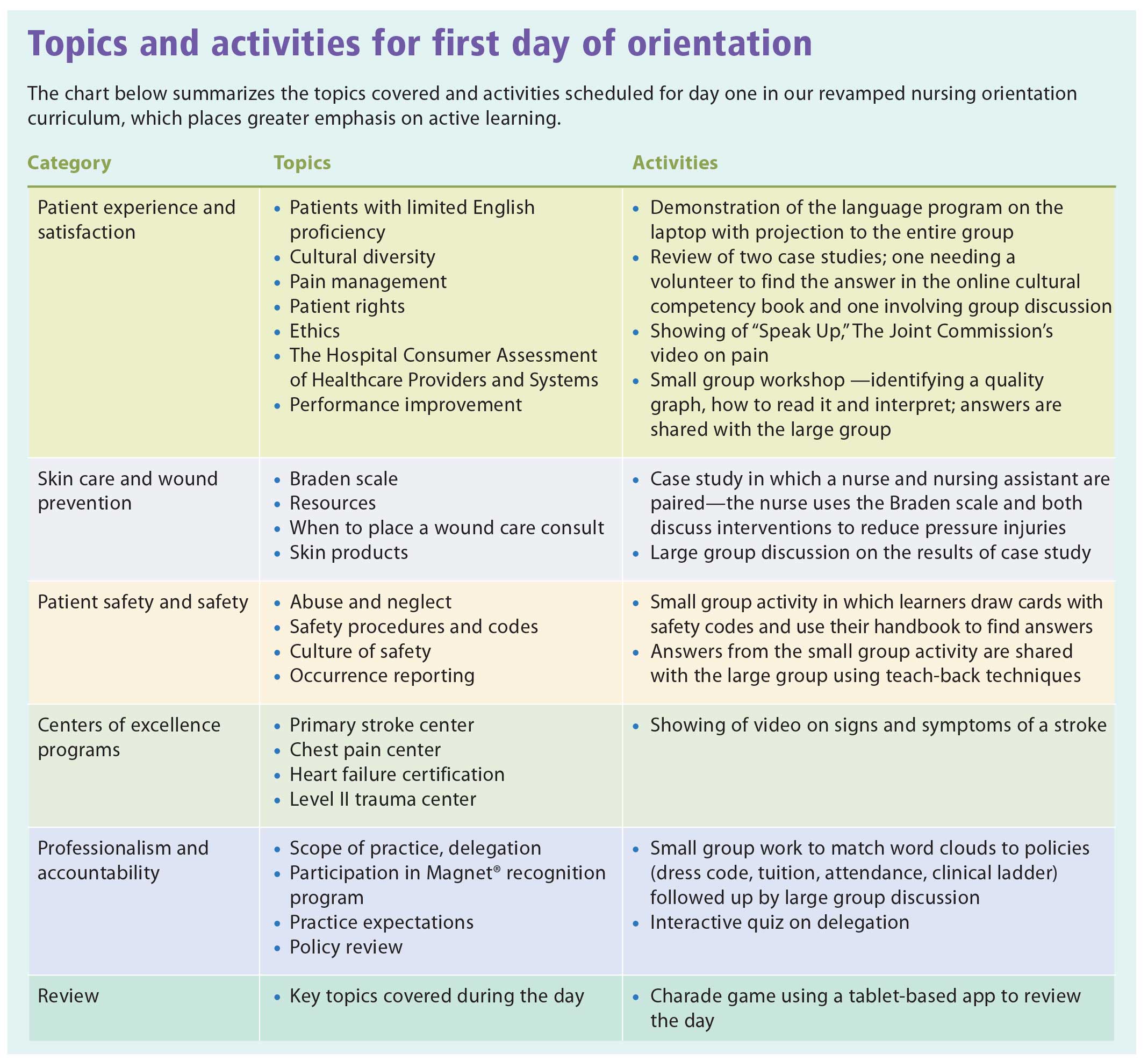
We reviewed all three hospitals’ orientation programs to determine what content was shared in common. Our goal was to develop one or more active-learning strategies for each topic category identified. Research shows that active learning strategies can increase retention of information and satisfaction with the learning experience and strengthen learner engagement. (See Topics and activities for first day of orientation.)
For example, in keeping the millennial generation’s love of technology, we incorporated a tabletbased game into the review at the end of the first day’s session. We made use of three tablets allocated for nursing education. An app guided a charadestyle game in which learners had to describe a topic covered during orientation without saying the actual name in their description. If the app displayed the words “bedside report,” the nurse could say, “informing the next shift about the patient in the room.” Nurses responded positively to this active approach to learning.
Simulation reinforces patient safety
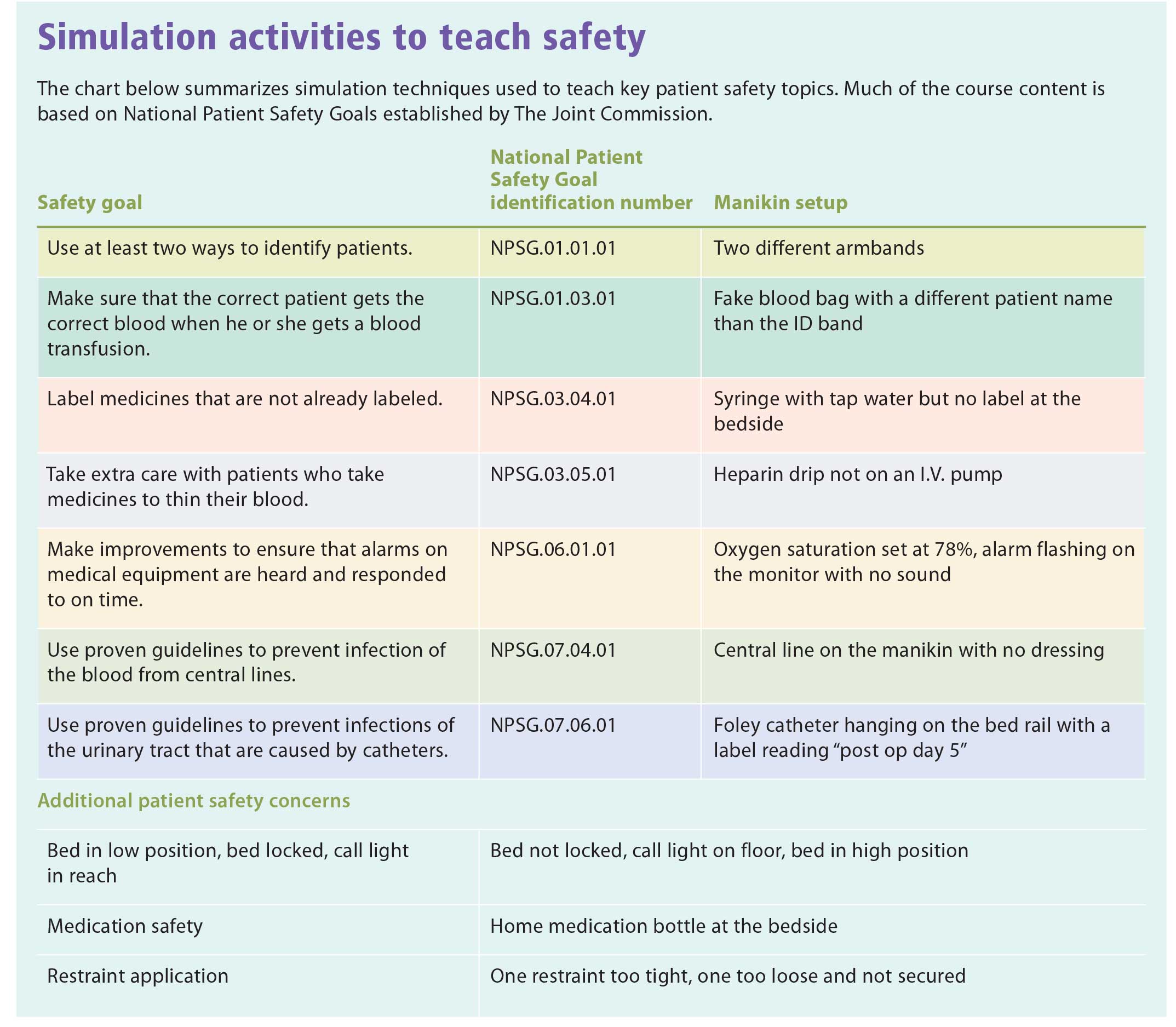
For the second day of orientation, we used simulation techniques to teach key patient safety topics. Simulation-based education engages the learner in hands-on activities, providing a safe but effective learning environment and creating fresh opportunities to improve communication and build knowledge and skills.
Course content was based on National Patient Safety Goals established by The Joint Commission to help healthcare organizations address issues related to patient safety. A manikin was used to simulate unsafe situations. (See Simulation activities to teach safety.)
Overview of the safety curriculum
Instructors present nurses with a patient care scenario using the manikin. Nurses must observe and identify what they find unsafe, as if participating in a scavenger hunt for clinical insights. In the discussion that follows, nurses gain insight into the relationship between their observations and safety goals.
The next activity reinforces expectations for customer service, defined in our health system’s standards for critical moments of service. Each nurse selects a card inscribed with a critical moment of service standard. He or she then has to demonstrate delivering care according to that standard as part of a simulation experience using a high-fidelity manikin operated by the instructor.
The group then takes a break. During the break, instructors use the manikin to set up a patient fall scenario. When nurses return from break, they must simulate the appropriate response to the fall. The instructor then leads a discussion on proper fall investigation procedures and interventions to prevent future falls.
Next, nurses practice donning and doffing basic personal protective equipment, included in the curriculum as part of heightened awareness of highly contagious infections. The instructor asks the nurses to peer review a partner and correct any mistakes to reinforce proper procedures.
Other topics are I.V. therapy, during which nurses complete hands-on practice with an I.V. pump, and code blue procedures, including a basic review of the crash cart monitor and how to activate a code.
The need for ongoing innovation
We implemented evaluation procedures to ensure that our new orientation program meets nurses’ needs and effectively prepares them to deliver safer care. We send a survey to nurses soon after they attend. Feedback indicates that most find learnercentered orientation effective and engaging.
Nursing orientation at our health system is now more streamlined, more efficient, and, most important, relies more heavily on active learning. We continue to monitor for barriers to effective learning to ensure continued success of the orientation program and make sure the learning experience remains optimal. Ongoing innovation in orientation is needed to give nurses new to our organization the best chance to succeed in practice.
Stephanie A. Walton is education coordinator lead at Mercy Hospital and Trauma Center in Janesville, Wisconsin. Deb Sitter is medical/surgical and ICU supervisor at Mercy Walworth Hospital and Medical Center in Lake Geneva, Wisconsin.
Selected references
Aldridge MD. How can nurse educators perform patient simulation efficiently? Teaching and Learning in Nursing. 2016;11(1):8-14.
American Nurses Credentialing Center. Pathway benefits.
Billings DM, Halstead JA. Teaching in Nursing: A Guide for Faculty. 5th ed. St. Louis, MO: Saunders; 2015.
Jeffery AD, Jarvis RL. Staff Educator’s Guide to Clinical Orientation: Onboarding Solutions for Nurses. Indianapolis: Sigma Theta Tau International; 2014.
Joint Commission, The. 2017 Hospital National Patient Safety Goals. The Joint Commission website. 2016.
Kennedy JM, Nichols AA, Halamek LP, et al. Nursing department orientation: Are we missing the mark? J Nurses Staff Dev. 2012;28(1):24-26.


















{kind=link}
{kind=link}