Learn how to identify this frequently misdiagnosed condition.
Takeaways:
- Cannabinoid hyperemesis syndrome is a growing but poorly understood healthcare concern within the rising number of chronic, habitual cannabis users in the United States.
- Cannabinoid hyperemesis syndrome is a three-phase cyclical syndrome characterized by periods of intense nausea and vomiting, frequently relieved with hot water bathing, that poses many diagnosis and treatment challenges.
- Treatment modalities are still being studied, but include using nontraditional antiemetic medications and abdominal capsaicin cream application. The most important treatment is supportive care to aid in cannabis use cessation.
Beer potomania and hyponatremia
Marijuana use could hurt the heart and blood vessels
Medical Cannabis: What Nurses Need to Know
Cannabis use in the United States continues to increase. With the legalization of recreational cannabis in 11 states and Washington, DC, as well as medical legalization in 33 states, a record number of Americans are consuming cannabis. According to a recent poll, approximately 34 million American adults use cannabis on a regular basis (at least twice monthly). With this rise in use comes a new set of challenges for healthcare professionals, including an increase in cannabinoid hyperemesis syndrome (CHS), a poorly understood condition that affects habitual cannabis users.
Signs and symptoms
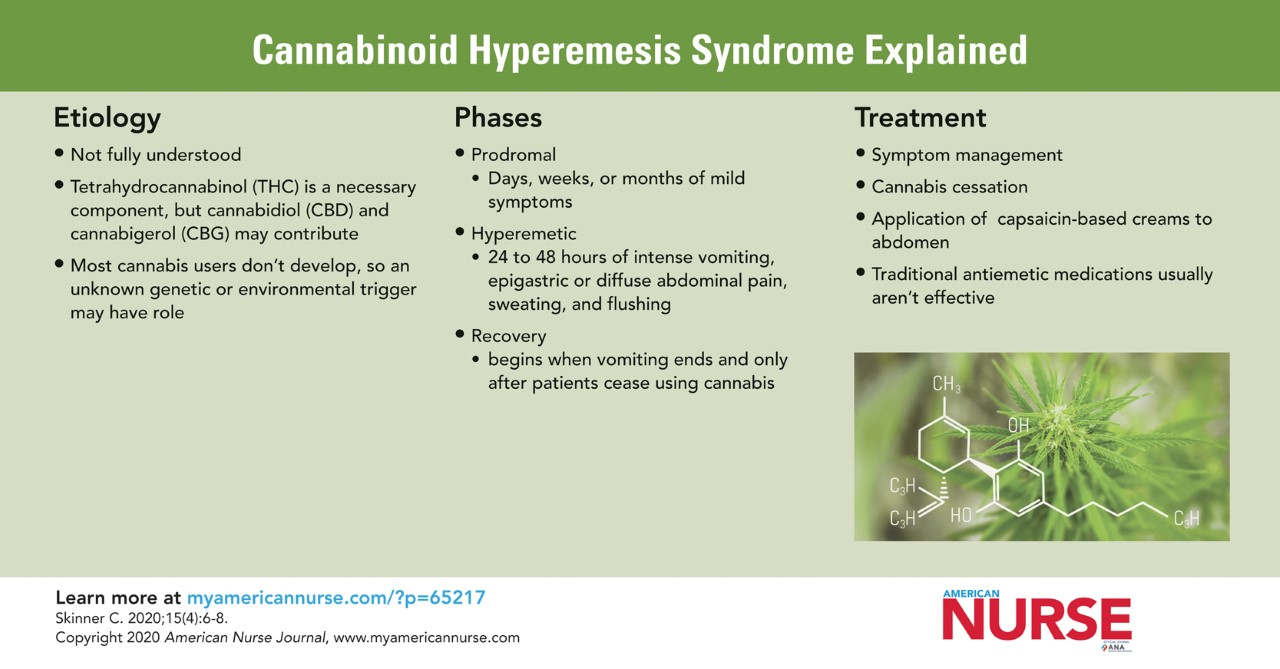
CHS is a cyclical three-phase (prodromal, hyperemetic or vomiting, and recovery) syndrome.
Prodromal phase
The prodromal phase is characterized by days, weeks, or months of mild symptoms. Researchers frequently describe them as similar to the “aura” of migraines because they precede an intense worsening of symptoms. In this phase, patients experience nausea, mild GI discomfort, and anxiety or restlessness. Symptoms are more commonly experienced in the morning but may be felt throughout the day. Patients’ eating habits are unchanged, and weight loss and vomiting are minimal or absent. Many patients continue or increase their cannabis use because they believe it will ease symptoms; they don’t make the connection between their symptoms and cannabis use because the symptoms don’t occur immediately after consumption.
Hyperemetic phase
The hyperemetic phase is characterized by 24 to 48 hours of intense vomiting, epigastric or diffuse abdominal pain, sweating, and flushing. Vomiting occurs as frequently as four or more times per hour. Nausea and vomiting in this phase are refractory to antiemetic medications. Weight loss and dehydration are common. Most patients in this phase cease cannabis use because of the intensity of their symptoms. When patients learn—usually by accident—that hot showering and bathing relieves symptoms, the behavior may become compulsive; some patients take up to 12 hot showers or baths per day during this phase. Many patients say that the hotter the water, the greater their relief, and some describe it as “washing away” their nausea.
Recovery phase
The recovery phase begins when vomiting ends and only after patients cease using cannabis. During this phase, patients are relatively symptom free; their eating habits return to normal, they gain weight, and they stop compulsively showering or bathing. Many patients resume cannabis use because they’re unable or unwilling to make the connection between it and their illness. In all studied cases, resumption of cannabis use caused symptoms to recur. This recurrence is compelling evidence that cannabis is the root cause of CHS, making a history of cannabis use essential for diagnosis.
 Presentation and diagnosis
Presentation and diagnosis
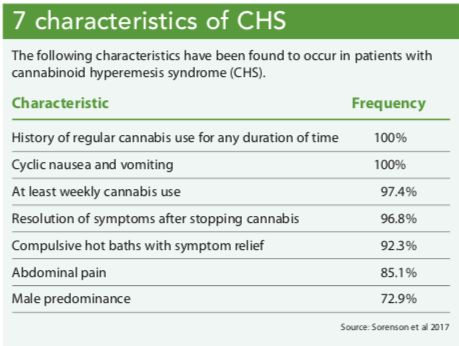
Most patients with CHS present in the hyperemetic phase, complaining of intense nausea, vomiting, and abdominal pain. The patient’s hair may be wet because of compulsive showering or bathing. The differential diagnosis list for nausea, vomiting, and abdominal pain is long, but seven characteristics identified in people with CHS may aid in diagnosis. (See 7 characteristics of CHS.)
Imaging (X-rays and computed tomography scans) is negative for findings in patients with CHS. And despite the intense GI symptoms and epigastric pain, endoscopy also is negative. Laboratory studies may reveal dehydration and subsequent electrolyte imbalance or acute renal failure, but will otherwise be unremarkable.
Within primary care settings, patients may report a history of emergency department (ED) visits and/or hospitalizations related to nausea, vomiting, and dehydration. They also may have a documented history of cannabis use. Consider CHS in patients with a reported or documented history of cyclical nausea and vomiting, negative imaging and lab studies, and known cannabis use.
Etiology
The cause of CHS isn’t fully understood, but it may be related to the effects of three components of cannabis: tetrahydrocannabinol (THC), cannabidiol (CBD), and cannabigerol (CBG). These chemical components work in the brain and the gut, where a host of cannabinoid receptors (CB1 and CB2) reside. (See The endocannabinoid system.) In the central nervous system (CNS), THC, CBD, and CBG have a variety of effects, one of which is potent antiemetic properties; THC has thermoregulatory effects within the hypothalamus.
In the enteric system, THC, CBD, and CBG actually have proemetic effects, but they’re thought to be “overridden” by the antiemetic actions of these chemicals in the brain, resulting in a net antiemetic effect. However, when cannabis is chronically and frequently used, its CNS effects may be overcome by the proemetic effect in the gut (perhaps due to tolerance), resulting in CHS.
In addition, THC is lipid-binding and can be stored within the body’s fat cells to potentially toxic levels with repeated, frequent use. In times of stress or illness, the stores of THC may be released from fat as it’s metabolized by the body, triggering or perpetuating CHS symptoms. The thermoregulatory effects of THC on the hypothalamus may be why hot baths and showers become a learned compulsion for symptom management.
Most cannabis users don’t develop CHS. Possibly an unknown genetic or environmental trigger is an underlying contributor for those who do develop it. And although CBD and CBG may contribute to CHS, THC is a necessary component of the syndrome. CBD in the absence of THC, for example, hasn’t been linked to CHS. More research is being conducted to understand the connection between genetics and the environment in CHS.
The body’s endocannabinoid system consists of cannabinoid receptors (CB1 and CB2 are the most common), ligands, and enzymes.
- Receptors can be stimulated by endogenous or exogenous (plant-derived or synthetic) cannabinoids.
- Ligands act as chemical messengers to get cannabinoids to interact at the receptor site.
- Enzymes break down cannabinoids after they’ve completed their function.
Source: Theisen and Konieczny 2019
Treatment
CHS treatment revolves around symptom management and cannabis cessation. In the hyperemetic phase, expect the patient to require I.V. fluids, rest, and monitoring for complications of dehydration. Inpatient care may be required, especially for patients with electrolyte imbalances or acute renal failure secondary to dehydration.
Traditional antiemetic medications such as ondansetron, promethazine, prochlorperazine, and metoclopramide generally aren’t effective in CHS. New research has shown some effectiveness with dopamine antagonists (such as haloperidol and ziprasidone) and benzodiazepines in inpatient and outpatient settings, although more studies are needed. Opioid analgesics provide little to no change in patients’ abdominal pain and have the potential to worsen nausea and vomiting. Patients should be allowed to bathe or shower, when appropriate, for symptom relief.
Applying capsaicin-based creams to the abdomen may relieve the nausea and vomiting associated with CHS. Capsaicin, a chili-pepper derivative commonly used in topical creams to treat musculoskeletal pain, is thought to cause vasodilation and disrupt the impaired thermoregulatory processes contributing to the patient’s symptoms; it’s considered a substitute to hot water bathing. In a study by Graham and colleagues, 13 adolescents with CHS were treated with capsaicin cream applied topically to their abdomens during the hyperemetic phase; 100% of the participants reported complete resolution or a significant decrease in their symptoms. (See A topical solution.)
The only cure for CHS is the complete cessation of cannabis and its derivatives, but this may be challenging for patients with cannabis use disorder. This complex and multifaceted psychological and physiological disorder may be accompanied by other conditions—such as anxiety, depression, chronic pain, post-traumatic stress disorder, and insomnia—that complicate cessation efforts. Patients will need counseling, medications, and other support services.
Capsaicin-based cream applied to the abdomen has been show to relieve symptoms of cannabinoid hyperemesis syndrome. Follow these instructions for use.
- Verify the order using the five rights of medication administration.
- Explain the application process to the patient and tell him or her about the potential side effects, which include a burning sensation and redness or irritation at the application site. Instruct the patient to avoid touching the cream with bare hands and to avoid transferring it to the eyes, mouth, and genitals.
- Perform hand hygiene and don gloves.
- Apply a thin layer of the cream (about 1 mm thick) to the patient’s entire abdomen.
- Instruct the patient not to touch the application site and to leave it exposed until the cream is fully absorbed into the skin.
- Remove gloves carefully to avoid accidental transfer to skin, clothes, and the environment.
- Reapply the cream as ordered, which may be up to four times daily.
Challenges
Diagnosing and treating CHS presents a number of unique challenges. Some patients may be misdiagnosed with cyclical vomiting syndrome or other GI disorders, especially if they’re not forthcoming about their cannabis use. The result may be years of suffering, unnecessary tests, and recurrent ED visits and hospitalizations. Studies show that people with CHS may visit the ED three to 11 times before diagnosis. Suggest the provider order a urine drug screen for patients with a history of cyclical nausea and vomiting that’s relieved with hot water bathing but who deny cannabis use.
Some patients may not make the connection between their symptoms and cannabis use. The widely known antiemetic properties of cannabis make the paradoxical symptoms of CHS difficult for many patients to accept, especially if they have cannabis use disorder. Communicate in a way that fosters patient trust in the healthcare team to encourage early diagnosis and treatment. Be factual and straightforward when explaining CHS to patients, and advocate for necessary supportive measures to aid cannabis cessation.
Stay up-to-date
CHS remains a poorly understood complication of habitual cannabis consumption. With the rise of cannabis use in the United States, nurses must remain up-to-date on the diagnosis, treatment, and challenges associated with CHS, and keep in mind that communication is critical to caring for patients with this debilitating syndrome.
Charlotte Skinner is a staff RN at St. Peter’s Hospital in Helena, Montana.
References
Graham J, Barberio M, Wang GS. Capsaicin cream for treatment of cannabinoid hyperemesis syndrome in adolescents: A case series. Pediatrics. 2017;140(6):e20163795.
Iacopetti CL, Packer CD. Cannabinoid hyperemesis syndrome: A case report and review of pathophysiology. Clin Med Res. 2014;12(1-2):65-7.
Lu ML, Agito MD. Cannabinoid hyperemesis syndrome: Marijuana is both antiemetic and proemetic. Cleve Clin J Med. 2015;82(7):429-34.
McCarberg B, D’Arcy Y. Target pain with topical peripheral analgesics. Nurse Pract. 2007;32(7):44-9. nursingcenter.com/pdfjournal?AID=728767&an=00006205-200707000-00014&Journal_ID=54012&Issue_ID=728736n
Marist Poll. Yahoo News/Marist Poll: Weed & The American Family. Marist College Institute for Public Opinion. April 17, 2017. maristpoll.marist.edu/wp-content/misc/Yahoo%20News/20170417_Summary%20Yahoo%20News-Marist%20Poll_Weed%20and%20The%20American%20Family.pdf
McNamara A. These states now have legal weed, and which states could follow suit in 2020. CBS News. January 1, 2020. cbsnews.com/news/where-is-marijuana-legal-in-2020-illinois-joins-10-other-states-legalizing-recreational-pot-2020-01-01
Solis-Garcia G, González-Martínez F, Urbiola E, et al. Cannabinoid hyperemesis in adolescents: A poorly diagnosed syndrome. J Paediatr Child Health. 2019;55(10):1264-6.
Sorensen CJ, DeSanto K, Borgelt L, Phillips KT, Monte AA. Cannabinoid hyperemesis syndrome: Diagnosis, pathophysiology, and treatment—a systematic review. J Med Toxicol. 2017;13(1):71-87.
Theisen E, Konieczny E. Medical cannabis: What nurses need to know. Am Nurse J. 2019;14(11):6-11.


















5 Comments.
We think my son has it he has been really bad but he has not smoked cannabis now for 2 days but he still has bad symptoms. He has been to the hospital 3 times here in England and 1 doctor did think he had CHS. But they haven’t given him anything. He has just gotta ride it out. It was only that I read this on line I thought it could be CHS.
Thank you, thank you for this article. My HCP advised me CHS may be my issue but left me completely in the dark regarding my education. Thank you again
I was diagnosed with CHS. Quit now
I have RA and used cannabis for 7-8 years at night only to help me sleep with the pain. I have suffered for the past 2 years with GI issues that worsened to the point in the past six months that I was deathly ill and no doctor could tell me what was going on. They could see damage in my stomach lining and issues with my kidneys but they could not tell what was causing it. In fact a couple of my doctors recommended using more cannabis to help with the nausea. Things got exponentially worse. Within two days of stopping all cannabis use I immediately felt better. It has been weeks now and I have not had one symptom. I have not felt this good for two years. I wish more doctors knew about this and more doctors could help their patients. It was hell what I lived through in the past six months: exhausted all the time, 4-5 days of feeling ok, 2-3 of severed stomach flu symptoms. Over and over.
Thank you for this article.
By stopping Cannibus. I feel Better. I was Suffering as well. Don’t mess with CHS