
Nurses can help patients make smart decisions by educating themselves.
Takeaways:
- Nurses frequently treat patients who use or are considering using cannabis as a medicine.
- Finding and validating information can be challenging, but proper and timely research can inform clinical nursing practice.
Cannabis and healthcare: Complicated policies and laws
Cannabinoid hyperemesis syndrome explained
CANNABIS has a long history as a medicine, in spiritual use, and for recreational use. Currently, 33 states, the District of Columbia, Guam, and Puerto Rico allow medical cannabis use under specific qualifying conditions, and 11 states (and the District of Columbia) allow adult recreational use.
Nurses frequently care for patients who use or are considering using medical cannabis. In 2018, the National Council of State Boards of Nursing (NCSBN) released guidelines for nurses who care for patients who use medical cannabis, stating, “Nurses need practical information to care for the increasing number of patients who utilize cannabis…who self-administer cannabis as a treatment for various symptomatology or for recreational purposes. Individuals are using cannabis and nurses will care for these patients.” (See Cannabis: 6 essential principles.)
Because cannabis science isn’t taught in most nursing schools (except in the context of misuse), nurses must find information about cannabis on their own. And because healthcare professionals typically possess little knowledge about cannabis therapeutics, patients frequently seek information from other patients, cannabis industry workers, and the internet. However, a recent article by Boatwright and Sperry found that 90% of the information on the top 10 cannabis websites was based on low quality studies and only one website used a medical professional to write about cannabis health claims. Finding and validating information can be challenging—proper and timely research, however, can inform clinical practice for nurses.
The endocannabinoid system
The main function of the endocannabinoid system (ECS) is to maintain homeostasis, which makes it a unique target for medical applications. This molecular signaling system consists of cannabinoid receptors (CB1 and CB2 are the most common and well studied), ligands, and enzymes that regulate sleep, pain perception, memory, mood, and appetite. The receptors can be stimulated by our own endogenous cannabinoids, by plant-derived cannabinoids (phytocannabinoids), and by synthetic cannabinoids. Ligands act as chemical messengers to get cannabinoids to interact at the receptor site, while enzymes break down cannabinoids after they’ve completed their function.
Cannabinoid receptors
CB1 and CB2 are G-protein-coupled receptors. CB1 receptors are predominantly found in the central and peripheral nervous systems, in the heart, lungs, adrenal glands, kidneys, pancreas, testes, ovaries, liver, colon, and prostate. When activated, CB1 receptors can help mitigate anxiety and stress, pain and inflammation, depression, post-traumatic stress, symptoms related to multiple sclerosis, and neurodegenerative disorders. Very few CB1 receptors are found in the brainstem or the cardiorespiratory centers, making a lethal dose of cannabis impossible.
The National Council of State Boards of Nursing has identified six principles of essential knowledge about cannabis for nurses, advance practice nurses, and nursing students.
1 The nurse shall have a working knowledge of the current state of legalization of medical and recreational cannabis use.
2 The nurse shall have a working knowledge of the jurisdiction’s medical marijuana program.
3 The nurse shall have an understanding of the endocannabinoid system, cannabinoid receptors, cannabinoids, and the interactions between them.
4 The nurse shall have an understanding of cannabis pharmacology and the research associated with the medical use of cannabis.
5 The nurse shall be able to identify the safety considerations for patient use ofcannabis.
6 The nurse shall approach the patient without judgment regarding the patient’s choice of treatment or preferences in managing pain and other distressing symptoms.
CB2 receptors also are found in the brain and peripheral nervous systems, but they’re concentrated in the peripheral immune cells. In addition, CB2 receptors are located in the lungs, uterus, brainstem neurons, and microglia. When activated, they mitigate inflammation, mental health disorders (including depression, bipolar, schizophrenia, and eating disorders), and neurologic diseases such as Alzheimer’s, Parkinson’s, Huntington’s, and multiple sclerosis.
Cannabinoids
Cannabinoids are chemical compounds that can influence the cannabinoid receptors and promote the release of neurotransmitters. They include phytocannabinoids, endocannabinoids, and synthetic cannabinoids.
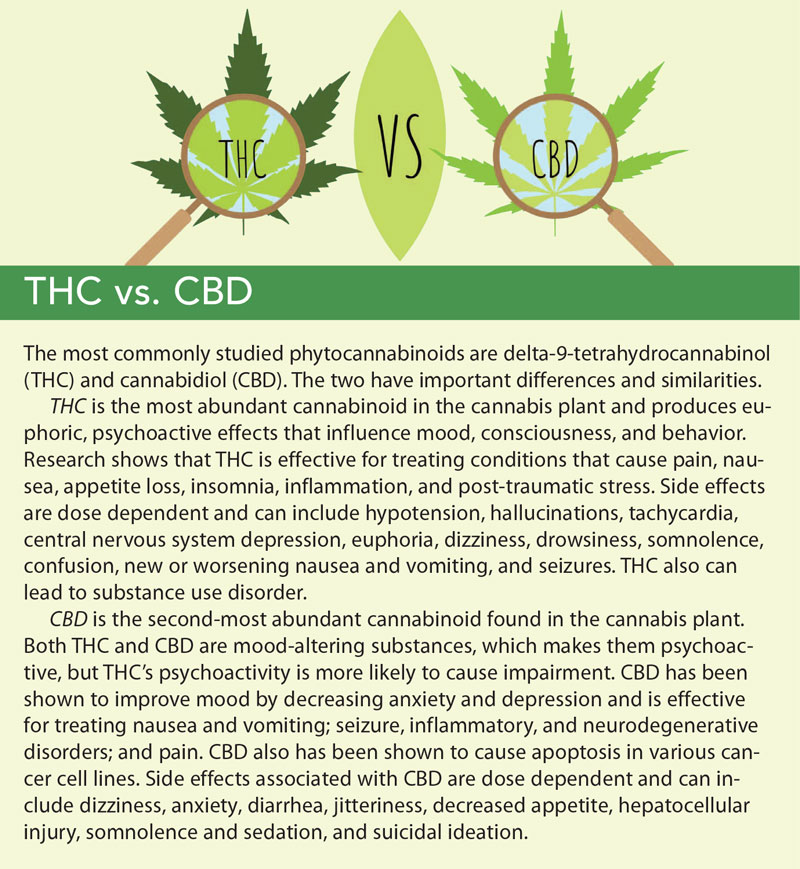 Phytocannabinoids produced by cannabis plants can activate receptors and are responsible for the medicinal and therapeutic effects of cannabis. Cannabis plants contain 100+ cannabinoids, but the most abundant and well studied are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD). Researchers hypothesize that phytocannabinoids work better together than in isolated forms of cannabinoids. For example, CBD can enhance the medicinal benefits of THC while also reducing THC’s unwanted adverse effects. (See THC vs. CBD.)
Phytocannabinoids produced by cannabis plants can activate receptors and are responsible for the medicinal and therapeutic effects of cannabis. Cannabis plants contain 100+ cannabinoids, but the most abundant and well studied are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD). Researchers hypothesize that phytocannabinoids work better together than in isolated forms of cannabinoids. For example, CBD can enhance the medicinal benefits of THC while also reducing THC’s unwanted adverse effects. (See THC vs. CBD.)
Endocannabinoids (endogenous cannabinoids) are molecules produced naturally and on demand by our own bodies. The two most researched and understood are anandamide and 2-arachidonoylglycerol.
Synthetic cannabinoids are created in the laboratory and are single, isolated molecules that contain no other components of the cannabis plant.
Cannabis options
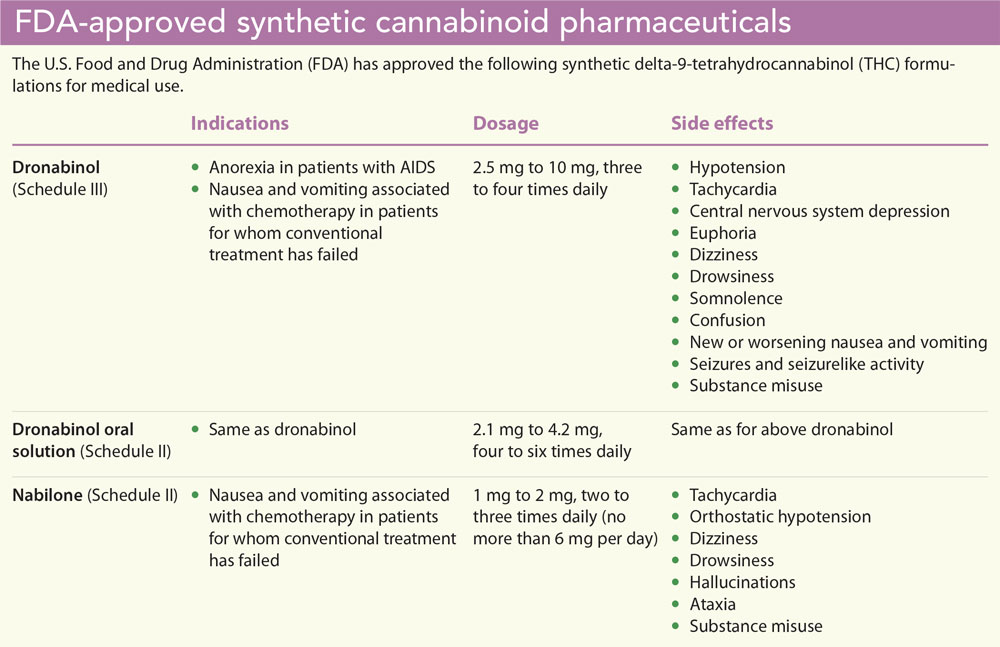
Cannabis products sold through state-licensed dispensaries can’t be prescribed in the United States. Despite widespread use around the world, cannabis was effectively taxed into prohibition by the Marihuana Tax Act of 1937 and was prohibited under federal law in 1970, when it was placed in the Controlled Substances Act Schedule I category, the most restrictive of five categories. By definition, all Schedule I drugs have no medicinal value and are highly addictive. All cannabinoids found in THC-rich cannabis plants remain in Schedule I. However, the Food and Drug Administration (FDA) has approved three synthetic cannabinoids. (See FDA-approved synthetic cannabinoid pharmaceuticals.) Despite being available by prescription for decades, synthetic cannabinoid preparations have not led to any black market or addiction treatment issues.
Epidiolex
In 2018, the FDA approved Epidiolex, an oral solution of plant-derived CBD. It’s approved for treating seizures in Lennox-Gastaut and Dravet syndromes in patients 2 years old and older. Dosages start at 2.5 mg/kg twice daily and can be titrated up to 20 mg/kg/day.
Epidiolex is approved as a Schedule V drug (the least restricted of the five categories and includes drugs with low potential for misuse). Side effects include hepatocellular injury, somnolence, sedation, and suicidal ideation.
Nabiximols
Nabiximols, a cannabis plant-derived oral mucosal spray, is a delta-9-THC and CBD 1:1 formulation (each spray is 2.7 mg THC and 2.5mg CBD). Nabiximols isn’t available in the United States, but it’s been approved in 25 countries for multiple sclerosis spasticity. Dosages range from two sprays up to 12 sprays daily. Side effects include tachycardia; transient alterations in blood pressure; dizziness; mood, memory, and coordination changes; and it has the potential for misuse.
Hemp
In December 2018, the Agricultural Improvement Act (“Farm Bill”) legalized hemp and defined it as any part of the Cannabis sativa L. plant, including cannabinoids. These changes removed hemp from restrictions under the Controlled Substances Act.
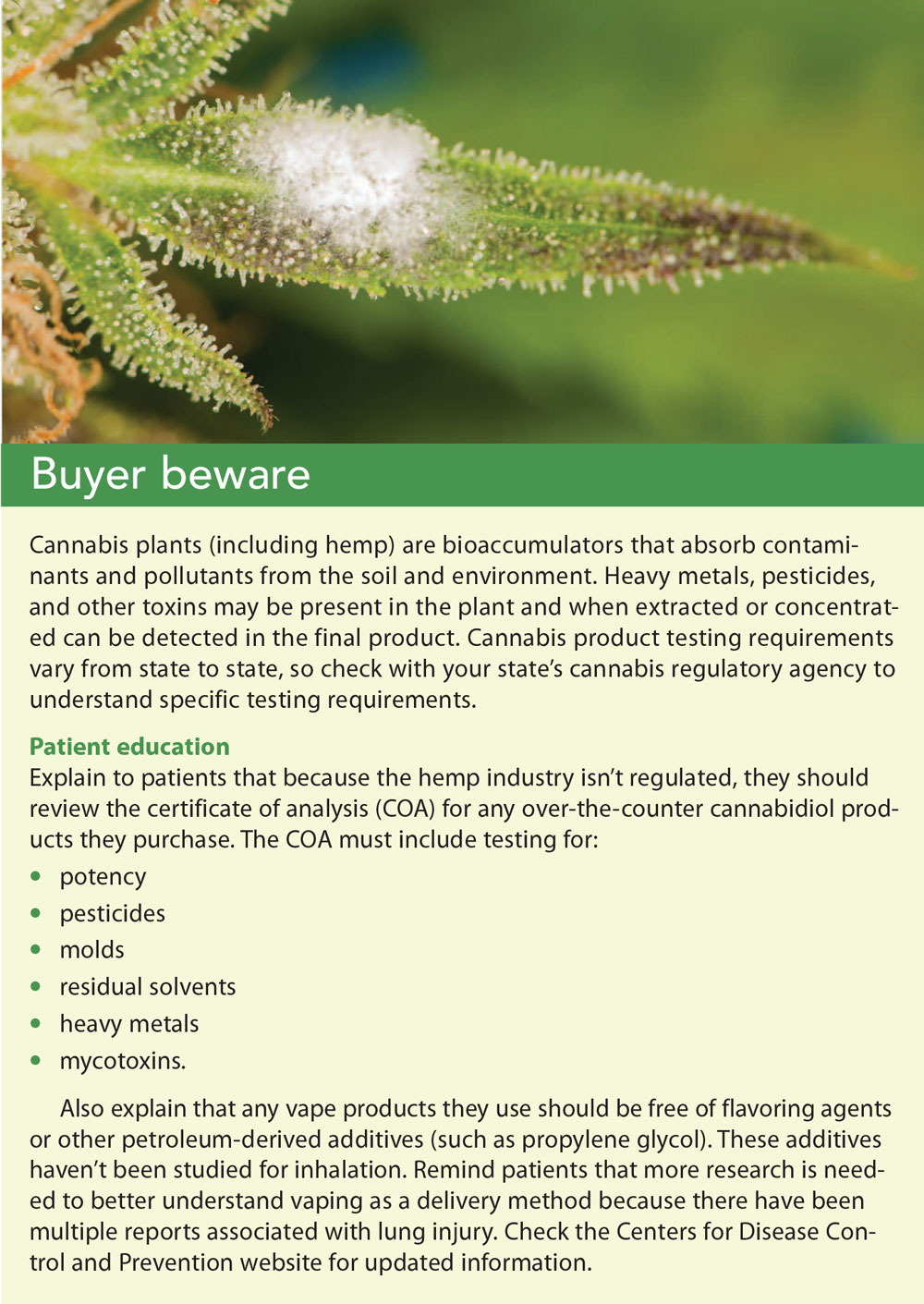 Many hemp-derived CBD products are available for purchase on the internet; in health food stores, pet food stores, and gas stations; and at many other retail locations. Conflicting federal laws have led to debate about the legality of these products; however, hemp-derived products in the United States remain unregulated. Without oversight, the products may contain toxins or be mislabeled. The Journal of the American Medical Association released a study by Bonn-Miller in 2017 that found 70% of CBD products were mislabeled. The study included vaporizer cartridges and tinctures and found that 42% contained more CBD than advertised and 26% contained less than advertised. Consumers should purchase only products with a certificate of analysis from a third-party testing facility. (See Buyer beware.)
Many hemp-derived CBD products are available for purchase on the internet; in health food stores, pet food stores, and gas stations; and at many other retail locations. Conflicting federal laws have led to debate about the legality of these products; however, hemp-derived products in the United States remain unregulated. Without oversight, the products may contain toxins or be mislabeled. The Journal of the American Medical Association released a study by Bonn-Miller in 2017 that found 70% of CBD products were mislabeled. The study included vaporizer cartridges and tinctures and found that 42% contained more CBD than advertised and 26% contained less than advertised. Consumers should purchase only products with a certificate of analysis from a third-party testing facility. (See Buyer beware.)
The U.S. Department of Agriculture doesn’t anticipate providing the regulations that oversee the Farm Bill until 2020, leaving patients and consumers with little protection and allowing product manufacturers complete autonomy when marketing their products. Consumer health and safety are at risk until these products are subject to a compliance pathway.
Cannabis administration
Cannabis products can be administered via various routes, including topical, transdermal, inhalation, sublingual, and ingestion. Understanding the onset and duration of action can help patients determine which route will effectively treat their symptoms. Unfortunately, the products available to patients depend on their state’s cannabis laws, and many state cannabis programs severely limit the product and formulary options.
Topical
Topical administration can provide quick, localized relief with little to no side effects. Unless the skin is broken, topicals typically don’t reach the bloodstream. When activated, CB1 receptors on the skin can help reduce redness and inflammation associated with conditions like atopic and contact dermatitis and psoriasis. Topical cannabis also has been shown to reduce pain and inflammation associated with arthritis. A study by Stinchcomb and colleagues reported that CBD can penetrate the skin 10 times more effectively than THC because it’s slightly more water soluble.
Patients have reported pain relief from topicals for muscle spasms and tightness, joint pain, burns, itching, and peripheral neuropathy. Onset of action generally occurs within 10 minutes and can last 2 to 3 hours. Topical cannabis products are ideal for patients who need localized relief; they might be less beneficial to patients who have more generalized conditions.
Transdermal
Transdermal cannabis products (typically patches) take effect within 1 hour and can provide between 8 and 12 hours of relief while avoiding first-pass metabolism. In patients where drug interactions or medication adherence is a concern, transdermal products can be the best administration route.
Inhalation
Inhalation provides rapid relief, reaching the bloodstream within minutes. Patients suffering from conditions that vary in intensity can benefit from this route because it provides nearly immediate relief, is the most predictable of administrations, and is the easiest to control. It also is preferable for patients who can’t ingest other forms of medications.
You must assess the patient to determine if the risks of inhalation outweigh the benefits, but an extensive review of the medical literature by the National Academies of Sciences, Engineering, and Medicine determined that smoking can nabis doesn’t lead to increases in lung, head, or neck cancers.
Sublingual
Sublingual applications can be an option for patients who can’t inhale. They take effect within 15 minutes and last 2 to 3 hours. How ever, many sublingual products are oilbased and might not absorb quickly into the mucosa, thereby following the pattern of ingestion and delaying onset by 1 to 2 hours. With oil-based sublingual products, patients should be advised to wait a full 2 hours before repeating the dose to avoid any potential adverse effects that can occur with over-ingesting cannabis.
Ingestion
Ingesting cannabis can provide longer-lasting relief than other administration methods and is ideal for patients who suffer from chronic pain, inflammation, nausea, and insomnia. A major disadvantage to ingestion is the variability in onset of action. Depending on the patient’s metabolism, genetics, gender, and food intake, the onset of action can range from 30 minutes to 2 hours (and sometimes longer). The effects, however, can last for 5 hours or more. Because of this unpredictability, patients can more easily over-consume and experience adverse effects, such as tachycardia, paranoia, hypotension, vomiting, and even hallucinations. To avoid overconsumption, patients should be advised to “start low and go slow,” waiting at least 2 hours before repeating a dose. Also, patients must know how to read the labels and understand serving sizes of the products they ingest.
Drug interactions
Although drug interactions with cannabis are rarely dangerous, review the patient’s medication and supplement list to ensure no contraindications exist before beginning cannabis therapy. Most interactions occur with ingested cannabinoids.
When taken orally, cannabinoids are metabolized by the CYP family of enzymes. THC is commonly metabolized by the CYP2C9, CYP2C19, and CYP3A4 enzymes, which convert THC into 11-hydroxy-THC (11-OH-THC). CBD is commonly metabolized by the CYP2C19 and CYP3A4 enzymes, which convert CBD into 7-hydroxy-cannabidiol (7-OH-CBD). Because most medications are metabolized by the CYP3A4 enzyme, CBD and THC can inhibit or induce other medications metabolized through that same enzyme. Also, some medications, such as warfarin, can inhibit or induce THC and CBD, increasing or decreasing cannabinoid plasma levels.
Because cannabis can produce sedative effects, it should be used with caution with other central nervous system depressants, including alcohol. Monitor patients throughout cannabis therapy to ensure safety and treatment adherence and to reduce potential interactions.
Assessment and dosing
For patients using medical cannabis, perform a systems assessment and thorough health history that includes a review of past treatments, comorbidities, previous cannabis experience, medication and supplement reconciliation, food and medication allergies, physical assessment, and risk for substance use disorder and psychiatric disorders.
Work collaboratively with the patient to determine his or her goals and encourage initially focusing on a single condition (which can decrease variables and improve adherence). Your nursing care plan should facilitate the patient’s goals while decreasing potential adverse effects and maximizing outcomes. Teaching patients how to read and understand product labels will help them better understand dosages and enable them to independently self-titrate their medicine. The more information the patient records (such as the route, dosage, time of administration, length of action, and effect), the more you can help him or her improve outcomes.
A typical cannabinoid serviing size can range from 5 mg to 10 mg (10 mg might be too high for a cannabis-naive patient), but the general cannabis protocol of “start low and go slow” is widely accepted. No established national dosage protocols exist for specific conditions. And because of federal cannabis laws, don’t recommend specific dosages to patients.
Cannabis dosing remains a challenge, but some providers have developed best practices. For example, Dustin Sulak, DO, of Healer.com provides patient education materials on tincture and inhalation dosages to guide patients on where to start. Everyone is different, so responses to cannabinoid dosages will vary from person to person, medicine. The more information the patient records (such as the route, dosage, time of administration, length of action, and effect), the more you can help him or her improve outcomes. Also, cannabis has bi phasic properties, producing one effect at a low dose and an opposite effect at a higher dose. Adverse effects from cannabis frequently depend on dose, and larger doses can exacerbate symptoms like anxiety, insomnia, and pain.
Learn more
As cannabis legalization continues to gain momentum, more patients will want to explore it as a medicine. Nurses must learn about the ECS, cannabinoids, routes of administration, potential drug interactions, and clinical implications to better serve patients.
Use these resources to learn more about medical cannabis and patient care:
• American Cannabis Nurses Association uses advocacy, collaboration, education, research, and policy development to support cannabis nursing practice.
• Americans for Safe Access is dedicated to ensuring safe and legal access to cannabis for therapeutic use and research.
• Healer is an online support community for patients using medical cannabis.
• Project CBD is a nonprofit in California dedicated to promoting and publicizing research into medical cannabidiol use.
• Society of Cannabis Clinicians provides continuing education, facilitates best practices, and conducts research related to medical cannabis.
For more resources, visit American Nurse Today.
Eloise Theisen is the chief executive officer at Radicle Health in Walnut Creek, California, and incoming president of the American Cannabis Nurses Association. Eileen Konieczny is past-president of the American Cannabis Nurses Association and author of Healing with CBD: How Cannabidiol Can Transform Your Health Without the High.
Select References
Abrams DI. Integrating cannabis into clinical cancer care. Curr Oncol. 2016;23(suppl 2):S8-14.
Agriculture Improvement Act of 2018, S.3042, 115th Cong. (2018). Congress.gov.–. June 18, 2018. congress.gov/bill/115th-congress/senate-bill/3042/text FARM BILL
Baker D, Jackson SJ, Pryce G. Cannabinoid control of neuroinflammation related to multiple sclerosis. Br J Pharmacol. 2007;152(5):649-54.
Barrus DG, Capogrossi KL, Cates SC, et al. Tasty THC: Promises and challenges of cannabis edibles. Methods Rep RTI Press. 2016.
Bhattacharyya S, Sendt KV. Neuroimaging evidence for cannabinoid modulation of cognition and affect in man. Front Behav Neurosci. 2012;6:22.
Boatwright KD, Sperry ML. Accuracy of medical marijuana claims made by popular websites [published online ahead of print December 30, 2018]. J Pharm Pract.
Bonn-Miller MO, Loflin MJE, Thomas BF, Marcu JP, Hyke T, Vandrey R. Labeling accuracy of cannabidiol extracts sold online [letter]. JAMA. 2017;318(17):1708-9.
Byars T, Theisen E, Bolton DL. Using cannabis to treat cancer-related pain. Semin Oncol Nurs. 2019;35(3):300-9.
Calabrese EJ, Rubio‐Casillas A. Biphasic effects of THC in memory and cognition. Euro J Clin Invest. 2018;48(5):e12920.
Challapalli PV, Stinchcomb AL. In vitro experiment optimization for measuring tetrahydrocannabinol skin permeation. Int J Pharm. 2002;241(2):329-39.
Chen DJ, Gao M, Gao FF, Su QX, Wu J. Brain cannabinoid receptor 2: Expression, function and modulation. Acta Pharmacol Sin. 2017;38(3):312-6.
Cravatt BF, Lichtman AH. The endogenous cannabinoid system and its role in nociceptive behavior. J Neurobiol. 2004;61(1):149-60.
de Mello Schier AR, de Oliveira Ribeiro NP, Coutinho DS, et al. Antidepressant-like and anxiolytic-like effects of cannabidiol: A chemical compound of Cannabis sativa. CNS Neurol Disord Drug Targets. 2014;13(6):953-60.
Fernández‐Ruiz J, Sagredo O, Pazos MR, et al. Cannabidiol for neurodegenerative disorders: Important new clinical applications for this phytocannabinoid? Brit J Clin Pharmacol. 2013;75(2):323-33.
Fisher T, Golan H, Schiby G, et al. In vitro and in vivo efficacy of non-psychoactive cannabidiol in neuroblastoma. Curr Oncol. 2016;23(2):S15-22.
Galiègue S, Mary S, Marchand J, et al. Expression of central and peripheral cannabinoid receptors in human immune tissues and leukocyte subpopulations. Eur J Biochem. 1995;232(1):54-61.
Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet. 2003;42(4):327-60.
Hill MN, Hillard CJ, Bambico FR, Patel S, Gorzalka BB, Gobbi G. The therapeutic potential of the endocannabinoid system for the development of a novel class of antidepressants. Trends Pharmacol Sci. 2009;30(9):484-93.
Hill MN, Patel S. Translational evidence for the involvement of the endocannabinoid system in stress-related psychiatric illnesses. Bio Mood Anxiety Disord. 2013;3(1):19.
Huestis MA. Pharmacokinetics and metabolism of the plant cannabinoids, delta 9-tetrahydrocannabinol, cannabidiol and cannabinol. Handb Exp Pharmacol. 2005(168):657-90.
Ishiguro H, Horiuchi Y, Ishikawa M, et al. Brain cannabinoid CB2 receptor in schizophrenia. Biol Psychiatry. 2010:67(10):974-82.
Jones NA, Hill AJ, Smith I, et al. Cannabidiol displays antiepileptiform and antiseizure properties in vitro and in vivo. J Pharmacol Exp Ther. 2010;332(2):569-77.
Lodzki M, Godin B, Rakou L, Mechoulam R, Gallily R, Touitou E. Cannabidiol-transdermal delivery and anti-inflammatory effect in a murine model. J Control Release. 2003;93(3):377-87.
McCarberg BH, Barkin RL. The future of cannabinoids as analgesic agents: A pharmacologic, pharmacokinetic, and pharmacodynamic overview. Am J Ther. 2007;14(5):475-83.
Minocci D, Massei J, Martino A, et al. Genetic association between bipolar disorder and 524A>C (Leu133Ile) polymorphism of CNR2 gene, encoding for CB2 cannabinoid receptor. J Affect Disord. 2011;134(1-3):427-30.
Morales P, Hurst DP, Reggio PH. Molecular targets of the phytocannabinoids: A complex picture. Prog Chem Org Nat Prod. 2017;103:103-31.
Musty RE, Rossi R. Effects of smoked cannabis and oral Δ9-tetrahydrocannabinol on nausea and emesis after cancer chemotherapy: A review of state clinical trials. J Cannabis Thera. 2001;1(1):29-56.
Nagarkatti P, Pandey R, Rieder SA, Hegde VL, Nagarkatti M. Cannabinoids as novel anti-inflammatory drugs. Future Med Chem. 2009;1(7):1333-49.
National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. 2017; Washington, DC: National Academies Press.
National Council of State Boards of Nursing. Nursing care of the patient using medical marijuana. J Nurs Reg. 2018;9(2):S23-7.
National Council of State Boards of Nursing. The NCSBN National Nursing Guidelines for Medical Marijuana. J Nurs Reg. 2018;9(2). ncsbn.org/The_NCSBN_National_Nursing_Guidelines_for_Medical_Marijuana_JNR_July_2018.pdf
Onaivi ES, Ishiguro H, Gong JP, et al. Discovery of the presence and functional expression of cannabinoid CB2 receptors in brain. Ann N Y Acad Sci. 2006;1074:514-36.
Onaivi ES, Ishiguro H, Gong JP, et al. Brain neuronal CB2 cannabinoid receptors in drug abuse and depression: From mice to human subjects. PLoS one. 2008;3(2):e1640.
Pacher P, Mechoulam R. Is lipid signaling through cannabinoid 2 receptors part of a protective system? Prog Lipid Res. 2011;50(2):193-211.
Palazuelos J, Davoust N, Julien B, et al. The CB(2) cannabinoid receptor controls myeloid progenitor trafficking: Involvement in the pathogenesis of an animal model of multiple sclerosis. J Biol Chem. 2008;283(19):13320-9.
Parker LA, Rock EM, Limebeer CL. Regulation of nausea and vomiting by cannabinoids. Br J Pharmacol. 2011;163(7):1411-22.
Patel S, Hillard CJ. Pharmacological evaluation of cannabinoid receptor ligands in a mouse model of anxiety: Further evidence for an anxiolytic role for endogenous cannabinoid signaling. J Pharmacol Exp Ther. 2006;318(1):304-11.
Price DA, Martinez AA, Seillier A, et al. WIN55,212-2, a cannabinoid receptor agonist, protects against nigrostriatal cell loss in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinson’s disease. Euro J Neurosci. 2009;29(11):2177-86.
Ramírez BG, Blázquez C, Gómez del Pulgar T, Guzmán M, de Ceballos ML. Prevention of Alzheimer’s disease pathology by cannabinoids: Neuroprotection mediated by blockade of microglial activation. J Neurosci. 2005;25(8):1904-13.
Resstel LB, Tavares RF, Lisboa SF, Joca SR, Corrêa FM, Guimarães FS. 5‐HT1A receptors are involved in the cannabidiol‐induced attenuation of behavioural and cardiovascular responses to acute restraint stress in rats. Br J Pharmacol. 2009;156(1):181-8.
Russo EB. Current therapeutic cannabis controversies and clinical trial design issues. Front Pharmacol. 2016;7:309.
Russo E, Guy GW. A tale of two cannabinoids: The therapeutic rationale for combining tetrahydrocannabinol and cannabidiol. Med Hypotheses. 2006;66(2):234-46.
Russo EB, Marcu J. Cannabis pharmacology: The usual suspects and a few promising leads. Adv Pharmacol. 2017;80:67-134.
Sagredo O, González S, Aroyo I, et al. Cannabinoid CB2 receptor agonists protect the striatum against malonate toxicity: Relevance for Huntington’s disease. Glia. 2009;57(11):1154-67.
Sánchez C, Galve-Roperh I, Canova C, Brachet P, Guzmán M. Delta 9‐tetrahydrocannabinol induces apoptosis in C6 glioma cells. FEBS Lett. 1998;436(1):6-10.
Schwitzer T, Schwan R, Angioi-Duprez K, et al. The cannabinoid system and visual processing: A review on experimental findings and clinical presumptions. Eur Neuropsychopharmacol. 2015;25(1):100-12.
Schwope DM, Karschner EL, Gorelick DA, Huestis MA. Identification of recent cannabis use: Whole-blood and plasma free and glucuronidated cannabinoid pharmacokinetics following controlled smoked cannabis administration. Clin Chem. 2011;57(10):1406-14.
Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: A randomized controlled trial. CMAJ. 2010;182(14):E694-701.
Zendulka O, Dovrtelová G, Nosková K, et al. Cannabinoids and cytochrome P450 interactions. Curr Drug Metab. 2016;17(3):206-26.

















8 Comments.
Very good article. How do I get my CEUs?
Good article
I enjoyed the article. I would like to submit for the ceu’s. How can I do that?
Really enjoyed this article. Very educational
It is so good to see an article that summarizes the science and research about cannabis, rather than the all-too-familiar Reefer Madness. The American Cannabis Nurses Assn. is a trusted resource for i\cannabis info.
Good article. Could have used more info.
I enjoyed the article. How can i earn the ceus?
I found the article very informative . It explained the different types of cannabis and the different implications for use. It explained the several different modes of administration & the risks, side effects of each. I truly hope this is addressed more fully in nursing curriculum.