
Treatment risks and how to manage them
Takeaways:
- Some cancer treatments can have cardiotoxic effects.
- Cardiotoxic effects include decreased heart function, chest pain, arrhythmias, palpitations, edema, hypertension, vascular disease, or shortness of breath.
- Cardio-oncology providers and nurses provide assessment and treatment for patients experiencing cardiotoxic effects from their cancer treatment.
 AS PATIENTS with cancer live longer, they face increased risk of developing secondary cardiac events linked to the treatments they received. All nurses who care for patients receiving cancer treatment should be familiar with potentially cardiotoxic cancer medications and treatments, recognize the signs and symptoms of cardiotoxicity, and know when to refer patients to cardio- oncology for further assessment and treatment. (See What’s cardiooncology?)
AS PATIENTS with cancer live longer, they face increased risk of developing secondary cardiac events linked to the treatments they received. All nurses who care for patients receiving cancer treatment should be familiar with potentially cardiotoxic cancer medications and treatments, recognize the signs and symptoms of cardiotoxicity, and know when to refer patients to cardio- oncology for further assessment and treatment. (See What’s cardiooncology?)
Cardiotoxicity
Cancer treatments such as radiation and chemotherapy can be toxic to the heart, resulting in cardiovascular abnormalities in conduction pathways (arrhythmias), vasculature (hypotension, hypertension, and Raynaud phenomenon), and coronary arteries (unstable angina, acute myocardial infarction), as well as cardiomyopathy and pericardial fluid accumulation. Symptoms of cardiotoxicity can include dyspnea, arrhythmias, cardiac dysfunction, fatigue, edema, chest pain, and ECG changes.
Potentially cardiotoxic medications
Some chemotherapy medications can cause short-term side effects that occur during treatment but stop when treatment ends, while other medications can lead to longterm effects that need ongoing management. The symptoms of shortand long-term side effects may be similar; the medication itself determines whether the side effects are reversible and how to proceed with treatment. (See Chemotherapy agents and potential cardiotoxicities.) The following categories of medications contain examples of cardiac side effects from specific drugs. Not all drugs in each category will have the same effect.
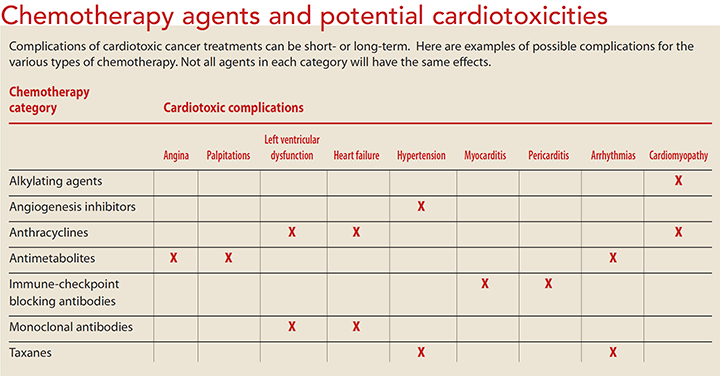
Alkylating agents. Cyclophosphamide is used to treat cancers of the GI tract, bone marrow, testicles, and ovaries. It can cause cardiomyopathy, plueral effusions, and myocarditis. Treatment includes relieving dyspnea and fatigue.
Angiogenesis inhibitors. Bevacizumab is used to treat kidney, colorectal, and lung cancers; sunitinib is used for kidney cancer. Other angiogenesis inhibitors are prescribed for kidney, lung, colorectal, thyroid, and stomach cancers, as well as multiple myeloma. Cardiac dysfunction has been reported with bevacizumab and sunitinib. Vascular endothelial growth factor receptor inhibitors (which are a type of angiogenesis inhibitor), such as sunitinib and sorafenib, block several tyrosine kinase receptors, making it difficult to identify which targets mediate cardiotoxicity. Tyrosine kinase inhibitors (which also are a type of angiogenesis inhibitor) have been associated with hypertension, and nilotinib and ponatinib specifically have been associated with thrombotic events.
Antimetabolites. Fluorouracil (5-FU), used to treat solid tumors, can cause angina and palpitations. Stopping the medicine frequently relieves symptoms.
Anthracyclines. Doxorubicin, which is used to treat breast cancer, solid tumors, sarcomas, lymphoma, and lung cancer, may cause cardiomyopathy and decreased heart function. Monitor heart function before and during treatment and manage symptoms as needed. Teach patients and families how to recognize the signs and symptoms of these conditions.
Immune-checkpoint blocking antibodies. Ipilimumab, nivolumab, and pembrolizumab, which are used to treat melanoma, non-small cell lung cancer, and renal cell cancer, can cause myocarditis and pericarditis. Treatment and management of the symptoms of these conditions (hypertension and peripheral vascular disease) include beta blockers, angiotensin-converting enzyme (ACE) inhibitors, and statins. Patients with known cardiac conditions prior to treatment should be closely monitored and treated quickly for declining heart function when taking these medications.
Monoclonal antibody. Trastuzumab is used to treat breast, lung, head and neck, stomach, colorectal, and prostate cancer, as well as Hodgkin’s lymphoma and melanoma. It can cause left ventricular dysfunction and congestive heart failure. Discontinuing the medication will reverse the symptoms, but it may take weeks for them to subside.
Taxanes. Paclitaxel and docetaxel, which are used to treat breast, lung, and ovarian cancers, may cause hypertension and arrhythmias, such as supraventricular tachycardia. Symptoms may resolve with cessation of the treatment.
Be aware that 5-FU, sunitinib, and some taxanes may cause QT prolongation. Treatment includes stopping cancer therapy and ECG monitoring until QT returns to baseline.
Assessing for cardiotoxicity
Patients receiving cancer treatment should be monitored for dyspnea, peripheral edema, and decreased heart function. The provider may order an echocardiogram or multigated acquisition (MUGA) scan to evaluate the patient’s baseline ejection fraction and to detect early signs of cardiotoxicity. If the ejection fraction is less than 40%, chemotherapy may be discontinued or reduced. Some patients may develop decreased ejection fraction during treatment, while others may not experience it until months or years after treatment. Echocardiography and MUGA scans also may be ordered to evaluate patients with complaints of increased dyspnea and peripheral edema.
ECG can be used to monitor heart function during and after cancer treatment. And advances in echo cardiography and strain imaging allow for early identification of decreased cardiac function so that the provider can make necessary treatment changes.
Any patient experiencing cardiac symptoms should be referred to cardio-oncology. The cardio-oncologist can prescribe medications to help control symptoms and continue to manage and monitor the patient. If a cardio-oncologist is not available, refer to a cardiologist experienced in managing oncology patients. (See Other considerations.)
Patient education
Educating patients about the potential cardiotoxic effects of cancer therapy is essential to successful treatment. Explain to patients and their families that potential side effects can occur during treatment or may not occur for years after. Emphasize the importance of following up with providers after treatment is completed and that all providers should be told about the cancer treatment so they can monitor for cardiotoxicity. (See Lifestyle changes and follow-up.)
Good outcomes
Caring for patients with cancer includes monitoring for and managing the effects of treatment. Cardiotoxicity symptoms can emerge well after treatment has ended, so thorough assessment and patient education is essential to good quality of life. And if your organization has a cardio-oncology team, use their expertise to improve your patients’ chances of a good outcome.
Bernadette Shields is a cardio-oncology nurse coordinator at Moffitt Cancer Center in Tampa, Florida.
Selected references
American Cancer Society. Coping with radiation treatment. October 26, 2017. cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation/radiation-therapy-guide/radiation-to-chest.html
Barros-Gomes S, Herrmann J, Mulvagh SL, Lerman A, Lin G, Villarraga HR. Rationale for setting up a cardio-oncology unit: Our experience at Mayo Clinic. Cardio-Oncology. 2016;2:5. cardiooncologyjournal.biomedcentral.com/articles/10.1186/s40959-016-0014-2
Curigliano G, Cardinale D, Dent S, et al. Cardiotoxicity of anticancer treatments: Epidemiology, detection, and management. CA Cancer J Clin. 2016;66(4):309-25.
Heinzerling L, Ott PA, Hodi FS, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J Immunother Cancer. 2016;4:50.
Myatt R. Cardiac dysfunction as a result of can cer treatment. Br J Cardiac Nurs. 015; 10(2):86-92.
Petek BJ, Greenman C, Herrmann J, Ewer MS, Jones RL. Cardio-oncology: An ongoing evolution. Future Oncol. 2015;11(14):2059-66.
Polovich M, Olsen M, LeFebvre KB. Chemotherapy and Biotherapy Guidelines and Recommendations for Practice. 4th ed. Pittsburgh, PA: Oncology Nursing Society; 2014.
Steingart RM, Yadav N, Manrique C, Carver JR, Liu J. Cancer survivorship: Cardiotoxic therapy in the adult cancer patient; cardiac outcomes with recommendations for patient management. Semin Oncol. 2013;40(6):690-708.
Toro-Salazar OH, Gillan E, Ferranti J, et al. Effect of myocardial dysfunction in cardiac morbidity and all cause mortality in childhood cancer subjects treated with anthracycline therapy. Cardio-Oncology. 2015;1(1). cardiooncologyjournal.biomedcentral.com/articles/10.1186/s40959-015-0005-8

















