
Equipment accessibility and multifunctionality help ensure program success.
Editor’s note: This is an early release of a web exclusive article for the March 2021 issue of American Nurse Journal.
Takeaways:
- Safe patient handling and mobility programs that effectively reduce injuries require patient-lift equipment.
- Meaningful injury reduction can be achieved only if caregivers are willing and able to use the equipment.
- Research indicates that overhead ceiling lifts are more beneficial than floor-based and portable lifts.
Patient-lift equipment is an essential contributor to effective safe patient handling and mobility (SPHM) programs because it helps reduce injuries. However, to achieve a meaningful reduction, caregivers must be willing and able to use the equipment. Organizations wanting to implement an SPHM program need to understand that success depends on how well it can ensure caregiver access to and use of equipment.
The essentials
SPHM programs must combine three separate but similar implementation requirements, all of which align with the American Nurses Association’s Implementation Guide to the Safe Patient Handling and Mobility Interprofessional National Standards:
Standard 2: Implement and sustain an SPHM program.
Standard 4.1.5: Identify technology that matches tasks.
Standard 4.1.5: Place unit or discipline-specific technology as near as possible to the task.
These standards are essential to improving caregiver willingness and ability to consistently apply patient-lift technology (equipment) in place of manual patient handling practices.
Why caregivers choose not to use equipment
When caregivers are asked why they choose not to use mechanical patient-lift devices, many say using them is too time-consuming. Lee and Lee reported that out of 4,674 California worker compensation cases related to patient handling, 82% were the result of employees choosing not to use patient-lift equipment even though it had been provided by their employers. This same study also concluded that within those incidents, patient-lift equipment was overlooked because it wasn’t readily available when the caregiver needed it. Studies by Lee and Lee and the LCWA Research Group concluded that only one-third of nurses with access to patient-lift equipment used it to perform patient-handling tasks. These studies indicated that simply owning patient-lift equipment wouldn’t guarantee employees would use it consistently.
Throughout my own nursing training and on-the-job experience, I found that much of what nurses were taught about patient care at the bedside focused on effectively managing time. Many nursing skills, including manual patient lifting, consider expedience as equal to competence. Consequently, many nurses consider patient-lift equipment too time-consuming and view it as either impeding their responsiveness to other patients or perhaps even challenging their professional competence. To reduce the too-time-consuming perception, patient-lift equipment must be readily available at the point-of-care. This is fundamental to constructing effective SPHM programs.
Patient-lift technology and time efficiency
Because nurses are more likely to use patient-lift equipment when it’s consistently and readily available within the immediate patient care workspace, facilitating its use is more closely related to addressing equipment proximity rather than convincing them that it’s helpful or beneficial. In other words, to reduce patient handling injuries, choose patient-lift devices that can be housed in patient-care workspaces.
When modifying patient-care areas to include patient-lift equipment, choices are limited. Common portable patient-lift challenges include finding storage, selecting devices whose wheels or castors can fit under hospital beds, and finding equipment that can maneuver in tight spaces around chairs or other bedside furniture. Portable patient-lifts have their place in SPHM programs, but they best serve as supplemental equipment.
Lateral transfer patient-handling devices, such as friction reduction or slide sheets and air-assisted lateral transfer devices aren’t ideal as primary SPHM program equipment; they’re more suited for short-term solutions in outpatient settings such as radiology or diagnostic departments. Friction reduction sheet material complicates laundering because of its sensitivity to heat and hot water. Air-assisted devices require a mat and air supply canister to work properly. Because nurses may have to leave the bedside to retrieve these items, they frequently revert to manual patient handling to save time. And although these tools are excellent for addressing horizontal or lateral patient-handling tasks, they can’t be used for vertical lifting or vertical transferring.
A comprehensive SPHM program that implements patient-lift devices that perform multiple tasks and are readily available at the point of care as an organizational standard for lifting and moving all patients, not just heavy patients, can help reduce staff injury significantly. Overhead ceiling lifts address both of these points: They can be permanently installed in patient care areas (without creating clutter) for easy accessibility, and they can be used to execute a variety of tasks, consistently eliminating risky patient-handling practices.
Overhead ceiling lifts
Overhead ceiling lifts, in addition to providing easy accessibility and multifunctionality, can help simplify staff education and training because they only have to learn to use one device. This also improves patient-lift equipment use by reducing confusion associated with differentiating among multiple patient-lifts and their associated slings. More importantly, overhead ceiling-lifts’ characteristics address caregivers’ concerns about time efficiency. Research supports staff beliefs that ceiling lifts are more beneficial to patient care than floor-based or portable lifts.
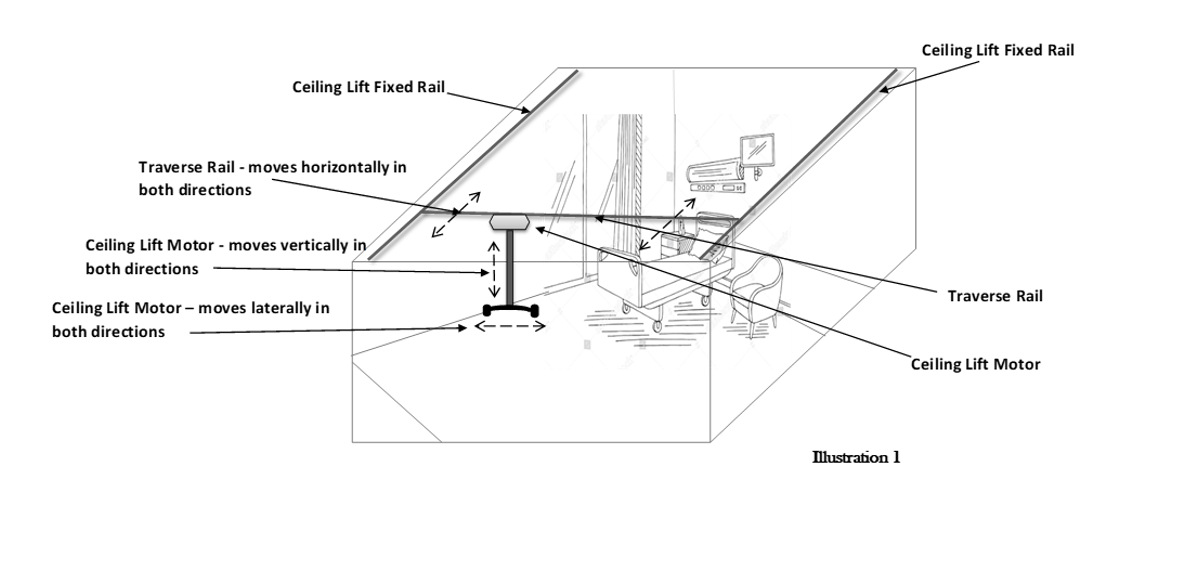
H-track ceiling lifts. H-track (also called XY-track) ceiling lifts have a traverse rail that’s centrally affixed between two stationary parallel rails. They can move laterally on the traverse rail and horizontally along the parallel rails in both directions. The attachment bar can be lowered to the floor, which allows staff to lift patients vertically, providing total patient-lift coverage over the room’s entire direct patient care workspace. Using these lifts, nurses can transfer patients from stretcher to bed, wheelchair to bed, and bed to bedside commode. The lifts also can be used to turn and reposition patients in bed, move them up in the bed, perform wound care or dressing changes, change linens and sheets, lift a fallen patient from the floor, and help patients walk around the room. This overhead ceiling-lift system can help nurses accomplish common patient care tasks safely that would otherwise require manual handling and lifting. (See H-track systems.)
H-track systems
This overhead diagram illustrates an H-track traverse track full inpatient hospital room system. The two stationary rails run parallel to one another and are located on opposite sides of the room to cover most of the patient care area.
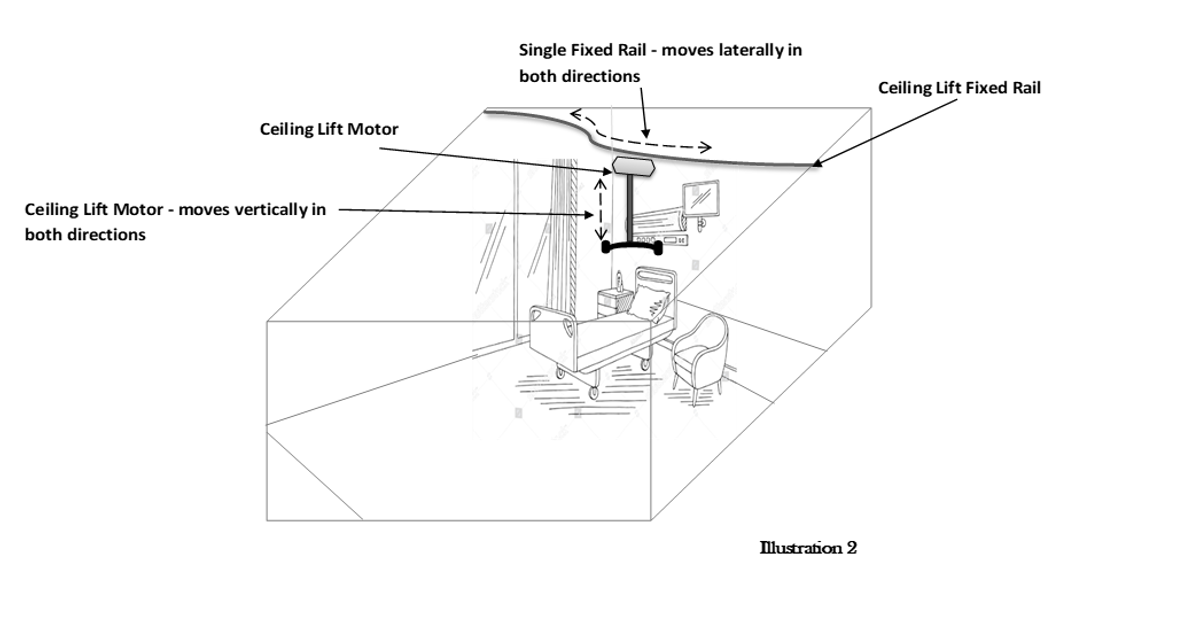
Single-rail or linear-track ceiling lifts. Single- or linear-track ceiling lifts have limitations that don’t allow nurses to use them to perform some common patient care tasks. The device’s hoist is limited to back-and-forth linear movement along the track’s path, which restricts the caregiver to using the ceiling-lift only within the space directly beneath the track. For example, if a patient needs to be transferred from a wheelchair or motorized scooter to a hospital bed, using a linear-track ceiling lift system requires aligning the wheelchair and bed under the single rail track. If a patient falls and has to be lifted from the floor, staff have to manually move the patient beneath the track. To turn and reposition a patient in bed, staff must move the bed to align it with the system. In an intensive care unit, using a linear system requires staff to maneuver around equipment, such as ventilators and pumps. (See Linear systems.)
Linear systems
Because linear track systems can move only back and forth along a single track, all patient care tasks must occur directly below the track, requiring manually moving patients or equipment.
These limitations and environmental barriers frequently lead staff to manually handle patients rather than taking the time to rearrange the room to use this system. Some perceive linear-track systems as more esthetically appealing than other systems, but the investment doesn’t yield the same return as H-track systems, negating the primary purpose of an SPHM program: reducing caregiver patient-handling injuries to caregivers.
The best approach
A direct correlation exists between SPHM program success and the type of patient-lift devices selected. Understanding the work routines of bedside nurses and other caregivers is the best way to determine what patient-lift devices are needed. Addressing caregivers’ willingness to use patient-lift devices and ensuring consistent equipment availability is the best approach to establishing and sustaining SPHM programs.
References
American Nurses Association. Safe Patient Handling and Mobility: Interprofessional National Standards Across the Continuum. Silver Spring, MD: American Nurses Association; 2013.
Enos L. The role of ceiling lifts in a safe patient handling and mobility program. Int J SPHM. 2018;8(1):25-45.
Gallagher S. Implementation Guide to the Safe Patient Handling and Mobility Interprofessional National Standards. Silver Spring, MD: American Nurses Association; 2013.
Lee S-J, Faucett J, Gillen M, Krause N. Musculoskeletal pain among critical-care nurses by availability and use of patient lifting equipment: An analysis of cross-sectional survey data. Int J Nurs Stud. 2013;50(12):1648-57. doi:10.1016/j.ijnurstu.2013.03.010
Lee S-J, Lee JH. Safe patient handling behaviors and lift use among hospital nurses: A cross-sectional study. Int J Nurs Stud. 2017;74:53-60. doi:10.1016/j.ijnurstu.2017.06.002
Nelson A, Motacki K, Menzel N. The Illustrated Guide to Safe Patient Handling and Movement. New York City, NY: Springer Publishing Company; 2009.
Roric P. Hawkins is the founder and president of The RP Hawkins Group (www.therphawkinsgroup.com) and the safe patient handling and mobility coordinator at Michael E. DeBakey VAMC in Houston, Texas.


















{kind=link}
{kind=link}