The nurse’s role at each point of care
Takeaways:
- Central vascular access devices (CVADs) can be essential to accomplishing patient therapeutic regimens.
- Nurses must be able to recognize signs and symptoms of CVAD-related complications at any juncture in the life of the device and be prepared to intervene during insertion, management, and removal.
- All vascular access devices are subject to complications that may cause patient harm, impair a patient’s quality of life, and increase morbidity and mortality.
Editor’s note: This article was developed in partnership with the Infusion Nurses Society. The Infusion Therapy Standards of Practice, published in the Journal of Infusion Nursing (2016), were used as a guiding reference. Please see the September issue of American Nurse Today for an article on complications of peripheral vascular access devices.
APPROXIMATELY 5 million central vascular access devices (CVADs) are inserted into U.S. patients every year, and at least 85% of hospitalized patients receive some form of I.V. therapy. The widespread use of CVADs presents considerable challenges for nurses when managing associated complications.
 Vascular access device (VAD) complications may delay treatment, damage vessels, limit options for future vascular access, cause pain and illness, decrease or impair quality of life, and increase morbidity and mortality, length of stay, and medical costs. All VAD types are subject to complications that may occur throughout the life of the device. Risk factors for CVAD-associated complications include disease state, concurrent infection, presence of immunosuppression or immunodeficiency, therapeutic regimen and type of infusate, prolonged hospitalization, and age- related or developmental-stage factors (such as fragile skin, changes in cognition/orientation, dexterity, and ability to communicate/learn) that might impact the ability to maintain and use the VAD safely.
Vascular access device (VAD) complications may delay treatment, damage vessels, limit options for future vascular access, cause pain and illness, decrease or impair quality of life, and increase morbidity and mortality, length of stay, and medical costs. All VAD types are subject to complications that may occur throughout the life of the device. Risk factors for CVAD-associated complications include disease state, concurrent infection, presence of immunosuppression or immunodeficiency, therapeutic regimen and type of infusate, prolonged hospitalization, and age- related or developmental-stage factors (such as fragile skin, changes in cognition/orientation, dexterity, and ability to communicate/learn) that might impact the ability to maintain and use the VAD safely.
The Infusion Nurses Society (INS) states that patient safety requires clinicians to be competent at recognizing signs and symptoms of VAD-related complications during insertion, management, and removal, and to intervene appropriately. This article presents an overview of CVAD terminology and common complications and discusses the nurse’s role during insertion; care, use and maintenance; and discontinuation.
Terminology
Before managing CVAD complications, nurses must understand the relevant terminology.
Common CVADs
Peripherally inserted central catheters (PICCs) are inserted through arm or neck veins in adults and children; in infants, they may be inserted through scalp or leg veins. Regardless of insertion site, the catheter tip is located in the superior or inferior vena cava, preferably at its junction with the right atrium.
Nontunneled CVADs can be vascular or nonvascular. They’re inserted by puncture directly through the skin and into the intended location. None of the devices should remain in a subcutaneous tract.
Tunneled cuffed catheters have a segment of the catheter lying in a subcutaneous tunnel, where tissue grows into the cuff for securement. The skin and vein exit sites are separated by the tunnel.
Implanted vascular access ports are surgically placed in a vessel, body cavity, or organ attached to a reservoir located under the skin. They have no external lumen until it’s accessed for use with a noncoring needle that has an integral extension set.
CVAD duration
The INS doesn’t recommend a specific VAD dwell time duration. Instead, the Infusion Therapy Standards of Practice state:
• Standard 44.2 VADs are removed if a complication can’t be resolved, at discontinuation of infusion therapy, or when they’re no longer deemed necessary.
• Standard 44.3 VADs aren’t removed based solely on length of dwell time because no known optimum dwell time exists.
Aseptic vs. sterile
Aseptic technique is a primary infection prevention method for keeping objects and areas free from micro-organisms using sterile supplies, barriers, and absolute separation of items that are sterile from those that aren’t. Dressing changes are performed using aseptic technique.
Sterile means that an environment is free from living organisms. It’s achieved by destroying both good and bad organisms. Although the method used for dressing changes is often referred to as “sterile technique,” this is a misnomer because a patient’s skin can’t be sterilized.
Insertion complications
Common insertion-related CVAD complications include infection, catheter malposition, and nerve injury. Patient disease state and physical condition may increase risk factors for complications, but with swift recognition and intervention, nurses can help prevent further patient harm. (See Insertion-related complications.)

Infection
Infection is perhaps the most prevalent, yet preventable, CVAD complication. Infections may be localized at the CVAD site or be systemic. To prevent these complications, CVAD insertion must be performed by a skilled clinician who adheres to infection prevention protocols including using a central line bundle with the following interventions:
- Perform hand hygiene before and at appropriate intervals during the procedure.
- Perform skin antisepsis using > 0.5% chlorhexidine in alcohol solution (use chlorhexidine with caution in premature infants or those under 2 months; consider using povidone-iodine instead).
- Use maximal sterile barrier precautions.
- Avoid the femoral vein as an insertion site in adults.
A second clinician trained in
CVAD insertion must observe the procedure and complete a standardized checklist. The observer’s roles and responsibilities include stopping the insertion if aseptic technique is breached.
Malposition
CVAD malposition occurs when the catheter tip is located in an aberrant position and no longer located in the original vena cava or cavoatrial junction. Malpositions are categorized as extravascular (catheter tip is located outside of the vein in nearby anatomic structures such as mediastinum, pleura, pericardium, or peritoneum) or intravascular (catheter tip is located in a suboptimal or aberrant position inside a vein). Intravascular CVAD malpositions are further categorized as either primary or secondary. Primary CVAD malposition occurs during the insertion procedure; secondary CVAD malposition may occur at any time during the catheter dwell time and is commonly referred to as tip migration. Using visualization technologies may prevent primary CVAD malposition.
Nerve injury
Nerve injuries during CVAD insertion frequently are attributed to inadvertent puncture of nerve structure near the insertion site or along the intended catheter tract. Clinicians should be aware of this potential complication and respond immediately if the patient complains of unusual pain or discomfort during insertion. Prompt intervention can mitigate or prevent permanent nerve damage. Collaborate with the patient’s provider to determine the best intervention.
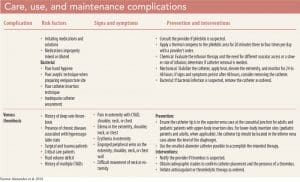
Care, use, and maintenance complications
CVADs must be regularly assessed for local complications, the most common of which are air embolism, bacteremia and septicemia, occlusions, venous thrombus, phlebitis, and catheter malposition. The nurse should assess the CVAD site visually to observe skin color and comparative extremity size and use palpation to detect swelling, warmth, pain, tenderness, and drainage. To identify systemic complications, the nurse should assess the patient for changes in temperature, heart rate, blood pressure, and patient reports of unusual discomfort, pain, or sensation. The CVAD must be assessed for patency, integrity and function, and malposition or migration. (See Care, use, and maintenance complications.)

Air embolism
Although primarily associated with CVAD discontinuation, air embolism can occur during care, use, and maintenance (for example, inadvertent disconnection of the administration set, failure to remove air from the set before use, or catheter fracture). Air embolism occurs when a bolus of air enters the vascular system, creating an intracardiac airlock at the pulmonic valve and preventing blood ejection from the right side of the heart. The force of right ventricular contractions increases, and small air bubbles break loose and enter the pulmonary circulation, obstructing forward blood flow, which results in tissue hypoxemia.
Bacteremia and septicemia
Bacteremia (microorganisms in the blood as identified by positive blood cultures) is considered catheter-related when the same organisms are isolated from both the catheter and the blood. Most catheter-related bloodstream infections are considered preventable. Prevention measures include performing hand hygiene before and after conducting interventions; disinfecting needleless connectors with alcohol wipes, alcohol chlorhexidine wipes, or alcohol caps before accessing; maintaining aseptic technique during all infusion therapy administrations and during all CVAD dressing changes; changing administration sets and addon devices at appropriate intervals; maintaining a closed infusion system; and discontinuing CVADs when they’re no longer necessary.
Occlusion
CVAD occlusions, which may increase the risk of catheter-related infection, are defined as partial or complete obstructions of the catheter lumens that restrict blood aspiration or fluid injection into the catheter. Occlusions may occur in response to catheter twisting or kinking, medication precipitate, the presence of a fibrin sheath, thrombus at the catheter tip, or positioning against the vessel wall. Interventions for catheter clearance should be performed as soon as possible when an occlusion is detected.
Venous thrombus
Although the CVAD is the primary contributing factor in catheter-related venous thrombosis, other multifactorial conditions may contribute, including the presence of a chronic disease that creates a hypercoagulable state, genetic abnormalities affecting coagulation factors, immobility, pregnancy, surgery, a history of multiple CVAD use, and age-related factors associated with the very young or very old.
Phlebitis
Phlebitis may be accompanied by pain, erythema, edema, streak formation, and/or a palpable cord. It’s caused by endothelial cell inflammation of the vessel and classified as chemical (chemicals in the infusate), mechanical (presence of the catheter in the vessel, catheter movement, inadequate vein-to-catheter ratio, or traumatic insertion), or bacterial (infection and inflammation affecting the vein wall).
Catheter malposition
As previously noted, CVAD malposition is the unintended placement of the catheter tip either internal or external to the vascular system. In CVADs, if the catheter tip doesn’t terminate in the lower third of the superior vena cava, the catheter is considered malpositioned. Extravascular malposition may cause infiltration/extravasation of the infusate in the mediastinum, hemothorax or pleural effusion if in the pleura, or pericardial effusion or cardiac tamponade if in the pericardium. Catheter malpositioning may occur during insertion but can occur during the care, use, and maintenance phase as well.
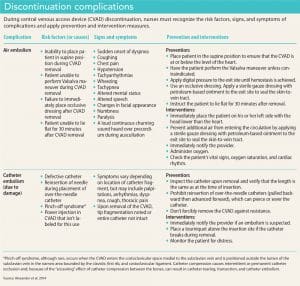
Discontinuation complications
Primary complications associated with CVAD discontinuation are air embolism, excessive bleeding, insertion site infection, and catheter embolism (catheter embolism can occur when a portion of the catheter separates or breaks off and remains in the patient after the CVAD is removed). Air and catheter embolism present the greatest risk for mortality or significant injury. Clinicians must be prepared to initiate emergency measures if necessary. Standard nursing protocol for all CVAD discontinuation must be followed to ensure patient safety. (See Discontinuation complications.)
Diligent nursing care
CVAD-associated complications are serious patient safety events that can prolong illness, cause permanent physical damage, increase healthcare costs, extend length of stay, or lead to death. Diligent nursing assessment and intervention is instrumental at CVAD insertion, care, use, maintenance, and discontinuation to prevent and detect the onset of CVAD-associated complications and to initiate corrective action and therapeutic management when complications occur.
The authors work at the Infusion Nurses Society in Norwood, Massachusetts. Dawn Berndt is the clinical education and publications manager, and Marlene Steinheiser is the director of clinical education.
To take the post-test for this course, please download the PDF copy of this article post.
Selected references
Alexander M, Corrigan A, Gorski LA, Phillips L. Core Curriculum for Infusion Nursing. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
Infusion Nurses Society. Infusion therapy standards of practice. J Infus Nurs. 2016;39 (suppl 1):S1-S159.
Joint Commission, The. Preventing Central Line–Associated Bloodstream Infections. A Global Challenge, A Global Perspective. Oak Brook, IL: Joint Commission Resources; 2012. jointcommission.org/assets/1/18/CLABSI_Monograph.pdf
Takashima M, Schults J, Mihala G, Corley A, Ullman A. Complication and failures of central vascular access device in adult critical care settings. Crit Care Med. 2018;46(12):1998-2009.
Ullman AJ, Marsh N, Mihala G, Cooke M, Rickard CM. Complications of central venous access devices: A systematic review. Pediatrics. 2015;136(5):e1331-44.

















1 Comment.
This was a very good review of CVAD.