Gain insight into prognosis and potential treatment plans.
- Nurses can better surveil and educate COVID-19 patients with an understanding of biomarker trends specific to the disease.
- Treatment-altering that influence course of treatment include blood gas measures, coagulation tests, and procalcitonin.
- Health status biomarkers that indicate health improvement or decline include inflammatory markers, liver function tests, and white blood cell differentiation counts.
More than 3 years of data and research have helped us understand that COVID-19 affects the body in many ways. The impact on the lungs is arguably the most infamous, but the disease also affects nearly every major organ including the kidneys, liver, GI tract, heart, and brain. This multisystem involvement makes evaluating patient recovery difficult.
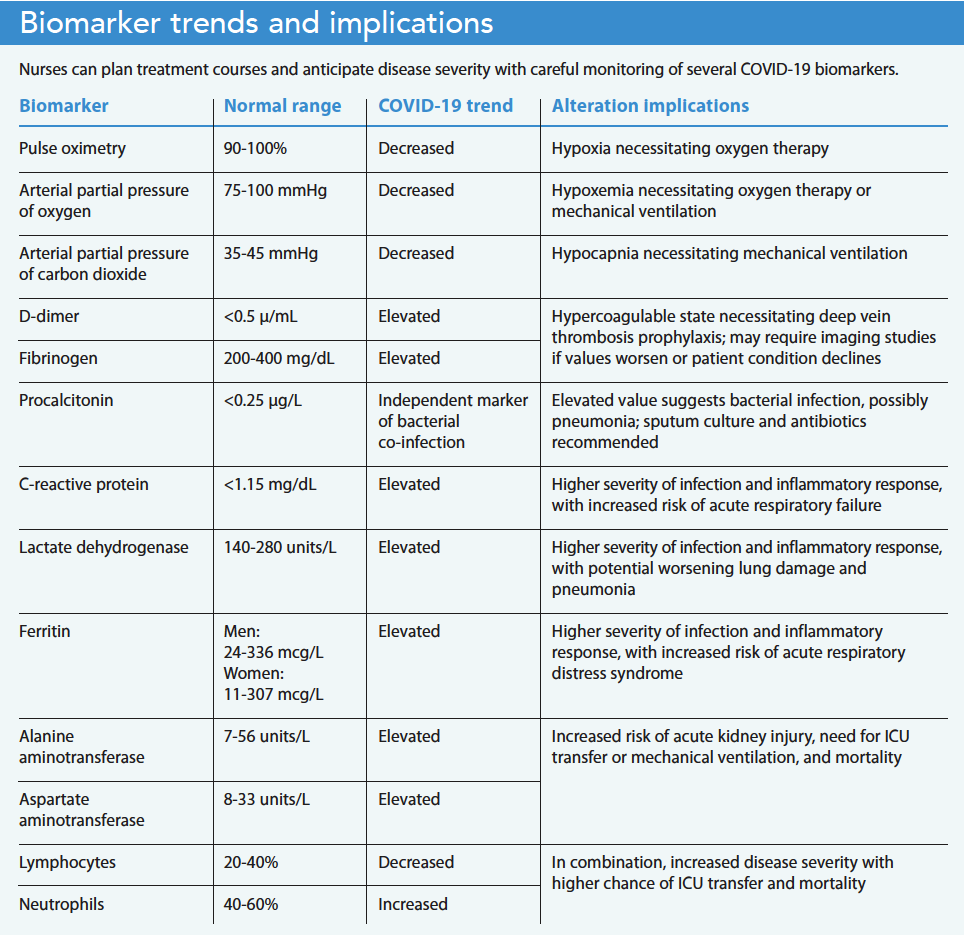
Beyond physical symptoms, COVID-19 also results in altered biomarkers, which can be measured on a molecular level to monitor many body systems affected by the disease, with severe disease states causing more notable imbalances. However, these tests are helpful only if we understand how to interpret them. Some biomarkers help determine the course of treatment, while others help gauge patient prognosis. Equipped with knowledge about COVID-19 biomarkers, nurses can anticipate changes in treatment plans, recognize evidence of a patient’s improvement or decline, and educate patients about their disease progression. (See Biomarker trends and implications.)
Treatment-altering biomarkers
Treatment-altering COVID-19 biomarkers include tests that measure blood gases, coagulation, and procalcitonin (PCT). They provide insight into the disease’s effects on the respiratory, cardiovascular, and immune systems.
Blood gases
Shortness of breath due to COVID-19 frequently leads to hospital admission. Unfortunately, patients with COVID-19 and pneumonia may have substantial damage to their lungs by the time they seek medical treatment as a result of silent hypoxia (a combination of low oxygen levels and lack of shortness of breath). The virus attacks the lungs at a cellular level, causing the alveoli to collapse and reduce oxygen absorption into the bloodstream. However, because it takes time for the lungs to fill with fluid from COVID-19, patients can still expel carbon dioxide, which prevents them from experiencing air hunger or shortness of breath.
Measuring pulse oximetry helps to ensure patients receive enough oxygen throughout the body; a low oxygen level suggests a patient requires a higher dose of supplemental oxygen. If COVID-19 progresses to pneumonia, the lungs fill with fluid and patients experience shortness of breath. In addition to oxygen deficiency, patients also experience a buildup of carbon dioxide trapped in the bloodstream. Checking arterial blood gas levels provides clinicians with a comprehensive view of the level of carbon dioxide and oxygen in the bloodstream, and whether the body has compensated effectively via respiratory or renal measures. Low partial pressures of oxygen or carbon dioxide suggest a need to change oxygen therapy and delivery, to slow the rate of breathing, and to increase the oxygen concentration of air entering the lungs.
Respiratory alkalosis, the most common arterial blood gas interpretation used with a patient who has COVID-19, suggests a need to increase both carbon dioxide and oxygen perfusion with mechanical ventilation. As a nurse, you can talk to patients about the reasons behind their changing oxygen demands and the equipment upgrades that will meet those demands.
Coagulation
COVID-19 can cause a hypercoagulable state, with many hospitalized patients experiencing complications such as deep vein thrombosis and pulmonary embolism; some also have experienced cerebral vascular attacks. As a result, providers place many patients with COVID-19 on prophylactic, low-dose anticoagulants.
Anticoagulation studies help monitor for and predict the risk of blood clots. COVID-19 can raise D-dimer and fibrinogen levels. Researchers and healthcare providers have found that elevation of both tests indicates more severe COVID-19 disease; however, a standardized demarcation between severe and non-severe cases hasn’t been established.
Monitoring these values can help you predict blood clots and patient decline. Providers frequently prescribe heparin (unfractionated or low molecular weight) prophylactically for hospitalized patients with COVID-19. If a patient requires supplemental oxygen and has an elevated D-dimer level, a higher therapeutic dose of heparin is recommended for the duration of the hospital stay. For patients reluctant to receive blood thinner injections, you can explain the increased risk of blood clots with COVID-19, and that the healthcare team is monitoring for blood clots using blood tests.
If coagulation tests continue to climb without an increased need for oxygen, the provider may order an ultrasound of the lower extremities to check for deep vein thromboses. If coagulation tests increase along with an increase in oxygen demand, the healthcare provider may order a chest computed tomography angiography to check for pulmonary embolism.
PCT
A bacterial infection can trigger the release of PCT within 12 hours of the infection taking hold. For patients with COVID-19, an elevated PCT level may indicate that an underlying bacterial infection is complicating the pneumonia already present as a result of the COVID-19 virus. Healthcare providers can start empiric antibiotics while waiting to identify a specific microbe via sputum culture. Using PCT as an indicator of bacterial infection prevents the overuse of antibiotics in patients with COVID-19 who wouldn’t benefit from these medications while fighting a virus.
When the healthcare provider orders antibiotics in response to a high PCT level or discontinues them due to a low PCT, explain to the patient and family the rationale for the treatment change.
Biomarkers that indicate recovery or decline
Various inflammatory markers, liver function tests, and white blood cell (WBC) differentiation counts help to monitor disease progression, with worsening values frequently predicting an increase in disease severity and sometimes a need for a higher level of care. Improving values may indicate a move toward recovery and potential treatment de-escalation.
Inflammatory markers
Several inflammatory markers can help predict recovery or decline in patients with COVID-19. These markers include C-reactive protein (CRP), lactate dehydrogenase (LDH), and ferritin.
As part of the body’s inflammatory response, the liver releases CRP. Patients with severe COVID-19 will have a noticeably elevated CRP value, indicating a stronger inflammatory response and an increased risk for acute respiratory failure. The mean CRP value tends to be significantly higher in severe cases (46 mg/L) compared to non-severe cases (23 mg/L). Typically, higher COVID-19 infection severity translates to a longer recovery period inside and outside the hospital and a higher likelihood of requiring mechanical ventilation. Monitoring this protein allows you to know whether a patient’s infection is improving or worsening.
Glucose metabolism includes the enzyme LDH, which also indicates an inflammatory response causing tissue damage. Similar to CRP, an elevated LDH level in patients with COVID-19 signals a stronger inflammatory response and a more severe infection. Of the five LDH isoenzymes found in different tissue types, COVID-19 has shown to increase the isoenzyme LDH-3, which is located in lung tissue. A correlation has been established between high LDH-3 levels in patients with COVD-19 and worsening lung damage and pneumonia. Monitoring this enzyme allows you to know whether a patient’s infection is improving or worsening, and whether more aggressive treatment measures for pneumonia and lung damage are recommended.
Ferritin, a protein traditionally known for its role in iron storage, also serves as an inflammatory marker. Low ferritin levels may indicate iron-deficiency anemia; high ferritin levels may suggest autoimmune diseases, chronic inflammatory conditions, and acute infections. In patients with COVID-19, elevated ferritin levels indicate more severe disease and increased risk for acute respiratory distress syndrome (ARDS). Monitor this protein to determine a patient’s progress in disease recovery and, when warranted, take additional precautionary measures against ARDS. Explain ferritin, LDH, and CRP test results to help patients understand how they’re progressing in their recovery.
Liver function tests
Elevated liver enzymes (especially alanine aminotransferase and aspartate aminotransferase) have been linked to COVID-19. Patients with COVID-19 who have elevated liver enzymes have higher rates of intensive care unit (ICU) admissions, acute kidney injury, need for mechanical ventilation, and mortality. When a patient with COVID-19 presents with elevated liver enzymes, be wary of other organ damage, including to the lungs and kidneys, and recognize the potential need for higher levels of care.
WBC differentiation counts
An overall WBC count doesn’t reliably gauge disease severity in hospitalized patients with COVID-19, especially when steroids are part of the standard medication regimen. Instead, review differential WBC counts, which examine five cell types: neutrophils, eosinophils, basophils, monocytes, and lymphocytes. In patients with COVID-19, a combination of decreased lymphocyte levels and increased neutrophil levels has been correlated with higher disease severity, rate of ICU admissions, and mortality. These counts can help you anticipate a decline in a patient’s condition and the need for more aggressive treatment.
Insight and empowerment
COVID-19 biomarkers provide nurses with insight into a patient’s disease progression. You can use these biomarkers to provide hope and empowerment by educating patients about how they’re being monitored and treated.
Holly Kreis is an inpatient telemetry nurse at Summa Health System’s Akron Campus in Akron, Ohio.
American Nurse Journal. 2023; 18(5). Doi: 10.51256/ANJ052344
References
Akdogan D, Guzel M, Tosun D, Akpinar O. Diagnostic and early prognostic value of serum CRP and LDH levels in patients with possible COVID-19 at the first admission. J Infect Dev Ctries. 2021;15(6):766-72. doi:10.3855/jidc.14072
Ali N. Elevated level of C-reactive protein may be an early marker to predict risk for severity of COVID-19. J Med Virol. 2020;92(11):2409-11. doi:10.1002/jmv.26097
Elshazli RM, Toraih EA, Elgaml A, et al. Diagnostic and prognostic value of hematological and immunological markers in COVID-19 infection: A meta-analysis of 6320 patients. PLoS One. 2020;15(8). doi:10.1371/journal.pone.0238160
Guler U, Costanzo I, Sen D. Emerging blood gas monitors: How they can help with COVID-19. IEEE Solid-State Circuits Magazine. 2020;12(4):33-47. doi:10.1109/MSSC.2020.3021839
Iba T, Levy JH, Connors JM, Warkentin TE, Thachil J, Levi M. The unique characteristics of COVID-19 coagulopathy. Crit Care. 2020;24(1):360. doi:101186/s13054-020-03077-0
Mahroum N, Alghory A, Kiyak Z, et al. Ferritin – from iron, through inflammation and autoimmunity, to COVID-19. J Autoimmun. 2022;126. doi:10.1016/j.jaut.2021.102778
Mondal S, Das TK, Bhattacharya S, Banerjee S, Hazra D. Blood gas analysis among COVID-19 patients: A single centre retrospective observational study. J Clin Diagn Res. 2021;15(8). doi:10.7860/JCDR/2021/49835.15185
National Institutes of Health. Antithrombotic therapy in patients with COVID-19. December 1, 2022. covid19treatmentguidelines.nih.gov/therapies/antithrombotic-therapy
Peters C, Williams K, Un EA, et al. Use of procalcitonin for antibiotic stewardship in patients with COVID-19: A quality improvement project in a district general hospital. Clin Med. 2021;21(1):e71-6. doi:10.7861/clinmed.2020-0614
Piano S, Dalbeni A, Vettore E, et al. Abnormal liver function tests predict transfer to intensive care unit and death in COVID‐19. Liver Int. 2020;40(10):2394-2406. doi:10.1111/liv.14565
Rostami M, Khoshnegah Z, Mansouritorghabeh H. Hemostatic system (fibrinogen level, D-dimer, and FDP) in severe and non-severe patients with COVID-19: A systematic review and meta-analysis. Clin Appl Thromb Hemost. 2021;27. doi:10.1177/10760296211010973
Key words: COVID-19, biomarkers, blood gases, coagulation, procalcitonin, inflammatory markers, liver function


















