
It’s 8:00 am and time for your 83-year-old patient, Virginia Johnson*, to take her oral medication. She was admitted with a left femoral fracture following a fall. After the initial surgery, she developed a urinary tract infection, and this morning she is disoriented and confused. As Mrs. Johnson takes the first pill, you notice she takes a long time to swallow and then coughs immediately after. You recognize that Mrs. Johnson may have dysphagia and that she’s at risk for developing aspiration pneumonia.
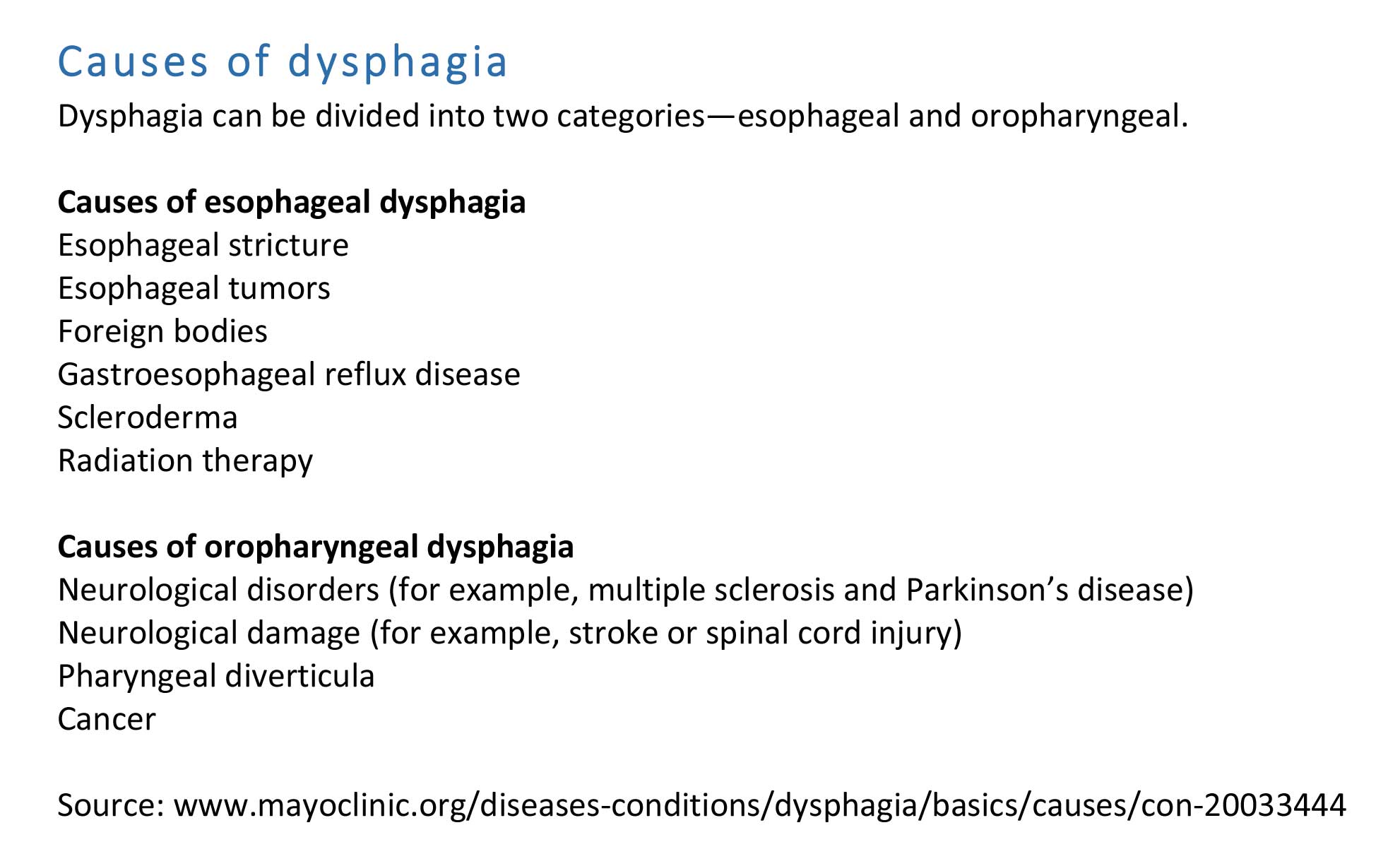
As the population ages, hospital clinicians see more patients with dysphagia resulting from stroke, dementia, and Parkinson’s disease. (See Causes of dysphagia.) Patients with dysphagia are at high risk for developing aspiration pneumonia as a result of food, liquid, or oral bacteria going into the lungs. Other complications include dehydration, malnutrition, and airway obstruction. Through consistent patient interaction and using a simple assessment technique, nurses can recognize dysphagia early and make referrals to help prevent complications, decrease hospital stay, and contribute to the health and safety of patients.
Bedside assessment
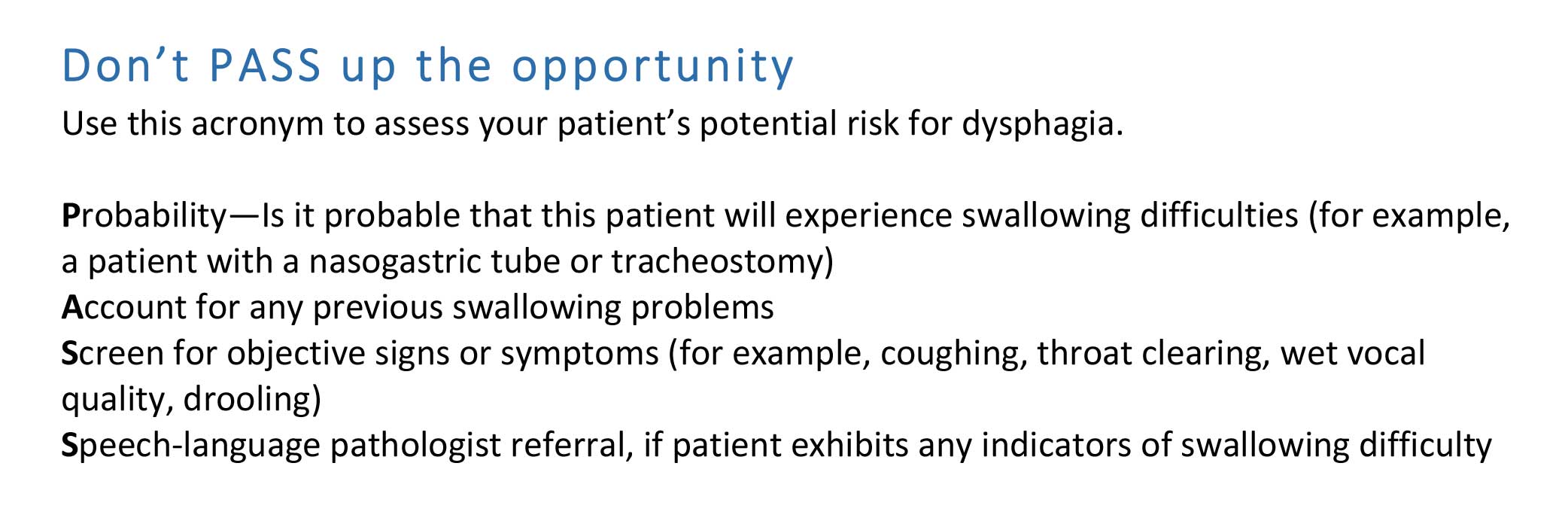
Use the PASS acronym to determine your patient’s risk for dysphagia (See Don’t PASS up the opportunity.) Start by asking if it’s probable that the patient will have difficulty swallowing. For example, intubated patients and those with feeding tubes are at risk for dysphagia. Next, ask for an account or history of previous swallowing problems, which may indicate future problems and the need for additional or immediate intervention.
The third step is to screen your patient for observable symptoms such as drooling, coughing, or change of voice or speech. Your observation doesn’t need to be formal; simply watch the patient while he or she is eating or taking medications. However, to ensure accuracy, make the following preparations:
- Ensure that the patient is seated as upright as he or she can tolerate without significant discomfort or pain.
- Make sure the patient is fully awake and alert.
- Note patient behaviors when eating or taking medication. For example, does the patient appear impulsive or anxious?
Any of the following signs or symptoms may indicate the need for an immediate referral to a speech-language pathologist (SLP) for dysphagia assessment:
- coughing or throat clearing before, during, or after swallowing
- wet, gurgling voice before, during, or after swallowing
- shortness of breath after swallowing
- drooling or loss of liquid from the mouth
- holding food or liquid in mouth for extended time without swallowing
- complaining of food or liquid feeling stuck.
Patients with risk indicators should also be referred for assessment by an SLP. Making a referral may not require input from a provider, but check your organization’s policy.
Interdisciplinary referral
Collaboration between speech pathology and nursing can help reduce complications related to poor swallowing. The SLP, after careful assessment, can adjust the patient’s diet related to the degree of swallowing difficulty. In addition, the SLP may prescribe the following exercises:
- neck muscle exercises
- tongue and oral exercises
- coughing exercises
- pursed lip breathing
- effortful swallowing.
Nursing considerations
Poor oral function can lead to an increase in gram-negative anaerobic bacteria and masticated food residue in the mouth, both of which increase the patient’s risk of developing upper respiratory infections and aspiration pneumonia. And in patients with decreased mobility, compromised respiratory status, or reduced cognition, poor oral hygiene may increase the risk of bacterial infections secondary to aspiration of secretions, food, or liquid into the lungs.
To prevent these complications secondary to dysphagia, ensure good oral hygiene. Provide consistent oral care, at least three times a day, including cleaning the tongue, palate, and teeth with a brush or swab. You or the SLP also can train patients, nursing assistants, and family members to provide oral care. It’s best to choose a consistent time, such as lunch, for reminding and encouraging the patient to perform swallowing exercises prescribed by the SLP
To ensure consistency of care, document all nursing interventions, including aspiration precautions, education, and patient understanding.
Stop complications before they start
Your early and accurate detection of dysphagia helps reduce patient complications. Using the PASS bedside swallowing assessment is an easy way to identify at-risk patients, make appropriate referrals, and stop the complications of dysphagia before they start.
After recognizing Mrs. Johnson’s difficulty swallowing, you notify her physician and make a referral to the SLP, reporting your PASS observations. After completing the swallowing evaluation, the SLP informs you that Mrs. Johnson appears safe for nectar thickened liquids and requests that her pills be administered crushed in puree. By working as a team, you and the SLP adjusted Mrs. Johnson’s plan of care, thus avoiding potential complications and ensuring Mrs. Johnson an uneventful recovery.
Carel Mountain is director of nursing at Sacramento City College in Sacramento, California. Kimberlee Golles is a speech-language pathologist at Kaiser Permanente Medical Center in Walnut Creek, California.
*Name is fictitious.
Selected references
Campbell G, Carter T, Kring D. Nursing bedside dysphagia screen: is it valid? J Neurosci Nurs. 2016;48(2):75-9.
Canham M. Looking into oropharyngeal dysphagia in older adults. Nursing. 2016;46(6):36-42.
Hines S, Kynoch K, Munday J. Nursing interventions for identifying and managing acute dysphagia are effective for improving patient outcomes: a systematic review. J Neurosci Nurs. 2016;48(4):215-23.
Park Y, Oh S, Chang H, Bang, H. Effects of the evidence-based nursing care algorithm of dysphagia for nursing home residents. J Gerontol Nurs. 2015;41(11):30-9.
Seedat J, Penn C. Implementing oral care to reduce aspiration pneumonia amongst patients with dysphagia in a South African setting. S Afr J Comm Disorders. 2016;63(1).


















{kind=link}
{kind=link}
1 Comment.
I was unaware that those who had strokes were more likely to develop dysphagia. My grandmother has dementia and recently broke her neck, so now I’m worried about her; she refused to eat the meat in her soup after saying she couldn’t swallow it. What kind of doctor should we take her to to check for dysphagia?