
A family-centered approach to neonatal opioid withdrawal syndrome
- Eat Sleep Console, a new model of care for infants with opioid withdrawal syndrome, focuses on the functional well-being of infants.
- First-line treatment includes nonpharmacologic interventions, such as skin-to-skin care, rooming-in, breastfeeding support, and parent education.
- Successful outcomes requires parental and family presence and engagement with the healthcare team.
THE OPIOID EPIDEMIC represents a public health challenge in the United States with significant impact on various populations, including those of childbearing age. When people experience opioid use disorder (OUD) in pregnancy, the fetus has prolonged exposure to the opioid. At birth, abrupt cessation of this exposure may lead to infant withdrawal symptoms, traditionally known as neonatal abstinence syndrome (NAS). Patrick and colleagues define NAS as withdrawal symptoms from various prenatal exposures; however, neonatal opioid withdrawal syndrome (NOWS) more accurately denotes cessation of prenatal opioid exposure.
Opioid use or misuse during pregnancy may lead to significant adverse outcomes, including maternal death, preterm birth, and stillbirth; infants exposed to opioids may experience low birth weight and postnatal health issues including NOWS. Providing counseling and treatment (with either methadone or buprenorphine) for pregnant people with OUD improves adherence with prenatal care and outcomes.
Neonatal abstinence syndrome: A quality improvement initiative
Caring for infants and families affected by neonatal abstinence syndrome
Medication treatment benefits include a stabilized environment for the fetus and reduced risk of severe NOWS symptoms. The Substance Abuse and Mental Health Services Administration notes that although medication for OUD leads to improved pregnancy outcomes, infants still may experience NOWS from prenatal exposure to methadone or buprenorphine.
To optimize health outcomes for infants with NOWS and their mothers, ongoing support includes coordinated holistic approaches to care. In 2017, Grossman and colleagues presented the Eat, Sleep, Console (ESC) model of care, which focuses on the functional well-being of the infant, an emphasis on nonpharmacologic interventions to manage NOWS symptoms, and empowerment of the mother and family to optimize nonpharmacologic care for the infant. (See ESC process of care.)
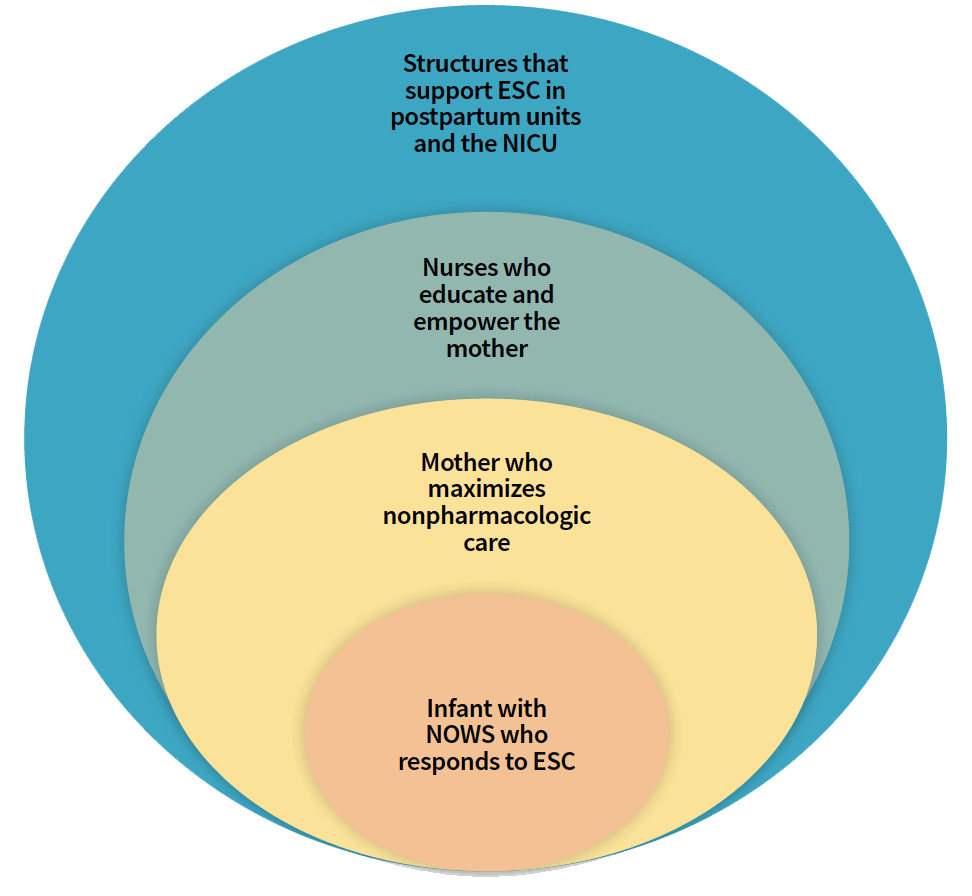
ESC process of care
The Eat, Sleep, Console (ESC) model of care involves various levels of support and collaboration.
NOWS symptoms
According to Patrick and colleagues, neonates experiencing NOWS have longer hospital stays than nonaffected neonates. Their central nervous system symptoms may include high-pitched crying, tremors, decreased sleep, a hyperactive Moro reflex, and seizures. Signs of autonomic nervous system activation include sweating, tachypnea, fever, nasal stuffiness, and increased yawning and sneezing. Infants also may experience GI symptoms, such as feeding difficulty, vomiting, and loose stools.
Some neonates experience few or mild withdrawal symptoms, while others develop more severe and persistent symptoms, which may prolong hospital stays. According to Patrick and colleagues, additional in-utero exposures (for example, to alcohol, tobacco, or benzodiazepines) may exacerbate NOWS symptom severity. The timing of NOWS symptom presentation varies, but onset typically occurs within 24 to 72 hours of birth. Inpatient monitoring of exposed neonates for a minimum of 4 days is required to assess for withdrawal symptoms.
Traditionally, NOWS assessment involved the use of a tool to score the severity of physiologic withdrawal symptoms, such as vomiting, tachypnea, yawning, and excessive sucking. Higher scores indicate more severe symptoms. Grossman and colleagues report that with this traditional method of assessment, repeated elevated scores frequently led to administering morphine, regularly dosed through a lengthy weaning process over several days to weeks, and monitoring in the neonatal intensive care unit (NICU). This approach often resulted in separation of the mother and infant.
ESC implementation
The ESC model of care includes assessing the infant’s functional well-being every 3 hours between feedings. If they can effectively breastfeed for at least 10 minutes (or take in an appropriate amount of formula), sleep at least 1 hour between feedings, and be consoled within 10 minutes using nonpharmacologic interventions, the healthcare team can consider NOWS symptoms well-managed. (See ESC functional assessment.)
ESC functional assessment
Nurses’ functional assessments of infants with neonatal opioid withdrawal syndrome, conducted every 3 hours, focus on the ability of the infant to eat, sleep, and be consoled. The nurse asks the following:
- Can the infant breastfeed effectively for at least 10 minutes or take an appropriate amount of formula from a bottle?
- Can the infant sleep undisturbed for at least 60 minutes?
- Can the infant be consoled with nonpharmacologic interventions within 10 minutes?
In addition, nurses offer the following:
- Optimization of nonpharmacologic interventions, including skin-to-skin care, a low-stimulation environment, gentle handling, clustered care, and breastfeeding support
- Ongoing coaching and messages of empowerment
Source: Grossman et al
If the infant can’t meet these assessment criteria, the healthcare team (including the bedside nurse) should huddle with the family to discuss how to maximize nonpharmacologic measures and then reassess functional criteria. If the infant continues to struggle to meet any one of the functional criteria, the provider should order an as-needed dose of morphine and continue nonpharmacologic strategies. Several sources (Achilles and colleagues, Grossman and colleagues, and Shuman and colleagues) recommend admission to the NICU or pediatric inpatient unit for close monitoring after administering morphine.
NICU and postpartum unit structures
Structures of care for hospital units implementing the ESC model include protocols for rooming-in, skin-to-skin practices, breastfeeding support, an ESC guideline/policy, and standardized parent education. (See Nonpharmacologic interventions.)
Nonpharmacologic interventions
Nurses educate and support families in their efforts to provide nonpharmacologic care to infants with neonatal opioid withdrawal syndrome.
- Rooming-in
- Mother–infant dyad maintained
- Continuous nonpharmacologic care
- Skin-to-skin care
- Feeding on demand
- Naked baby (except for diaper) held upright on awake mother’s bare chest
- Breastfeeding
- Lactation support
- Contraindications may include HIV+ status or current illicit substance use
- Low-stimulation
- Limited noise environment
- Low lighting
- Clustered care, assessments, and vital signs
- Soothing and consoling
- Holding
- Gentle handling
- Rocking
Sources: Achilles and Castaneda-Lovato, Grossman et al
Rooming-in. According to Grossman and colleagues, keeping the mother and infant in the same hospital room (rooming-in) promotes feeding on demand, maternal–infant bonding, and optimization of nonpharmacologic care practices. Others (Achilles and Castaneda-Lovato, Grossman and colleagues, Patrick and colleagues) note the association between rooming-in and improved breastfeeding rates and decreased lengths of hospital stay for infants with NOWS.
Skin-to-skin care. McGlothen-Bell and colleagues describe the postpartum practice of skin-to-skin care or kangaroo care as holding the naked baby, except for the diaper, upright on the mother’s bare chest. Skin-to-skin contact promotes maternal–infant bonding, encourages breastfeeding, and aids consoling.
Breastfeeding support. Several studies (by Achilles and Castaneda-Lovato, Grossman and colleagues, and others) report that infants with NOWS experience fewer physiologic symptoms of withdrawal when breastfeeding. Wu and Carre report that many infants with NOWS who breastfeed don’t require pharmacologic treatment for their withdrawal symptoms and have shorter hospital stays.
Providers should encourage mothers treated for OUD with methadone or buprenorphine and not actively using illicit substances to breastfeed. Promoting breastfeeding or breast milk feeding includes education about its benefits and support for mothers before and after birth of the infant..
Parent education. Knowing about ESC, nonpharmacologic care practices, and what to expect in the postpartum period prepares families to care for infants with NOWS. Support includes early identification of OUD in pregnancy as well as education about the ESC approach to care and expected length of hospital stay. Ongoing support and education about nonpharmacologic care practices promote maternal agency and positive outcomes for infants.
Standardized nonpharmacologic care. In addition to rooming-in, skin-to-skin care, feeding on demand, and gentle handling, many infants benefit from a low-stimulation environment. Keep lighting subdued, limit noise, cluster care, and provide a pacifier for nonnutritive sucking.
Empowered parents. Grossman and colleagues note that a holistic, family-centered approach to care facilitates positive health outcomes for infants with NOWS. The ESC model of care emphasizes a collaborative relationship and encourages a proactive role for parents. The healthcare team can offer motivational messages, such as, “You’re the treatment for your infant,” and “Your presence and care are what’s most important for your infant.” In addition, the team can provide coaching on the use of nonpharmacologic interventions.
According to Recto and colleagues, pregnant and parenting people with OUD can experience stigma and discrimination during the perinatal period, which may impact their role in the care of their infant with NOWS. Supporting family engagement in the ESC model of care requires decreasing this stigma and bias. Initial steps include nurse education and training to understand and recognize the harmful impact of stigma among those with OUD, such as being shamed or ostracized. Ongoing nonjudgmental support for the maternal–infant dyad and their families facilitates care practices aimed at improving newborn outcomes.
Medication as needed
When infants don’t respond to nonpharmacologic interventions, providers may order an as-needed dose of medication, which frequently requires admission to the NICU or inpatient pediatric unit. Patrick and colleagues report that morphine remains the most common medication for managing NOWS, but providers also may order methadone or buprenorphine. Second-line treatment may include clonidine and phenobarbital. If the infant requires repeated doses of as-needed medication, the healthcare team may elect to initiate a daily weaning dose of medication.
Discharge planning
The infant’s primary care provider should closely monitor for growth and development, any ongoing NOWS symptoms, and offer support and anticipatory guidance for the family. Other aspects of discharge planning include assessment of a safe sleep environment, a proper car seat, a secure home setting, and robust family support. The infant and family also may require community health nurse visits and early intervention services.
Family-centered care
Achilles and Castaneda-Lovato, Grossman and colleagues, and Patrick and colleagues support a holistic family-centered approach to care for opioid-exposed mother–infant dyads. Partnering with parents to optimize nonpharmacologic care of the newborn with NOWS is key to the ESC model’s success. For example, care team huddles that include pediatric providers, nurses, and parents enhance communication. The healthcare team also must address barriers to care, including their own biases about OUD in pregnant and parenting people as well as family fear of criminal justice system and child protective services involvement.
Many pregnant people with OUD are impacted by social determinants of health (SDOH), which the World Health Organization defines as the conditions in which people are born, grow, live, work, and age, as well as additional forces such as lack of transportation, food insecurity, interpersonal violence, unsafe neighborhoods, and unstable housing. SDOH also include societal inequities such as structural biases, discrimination, and racism. These conditions contribute to maternal–infant health and are important to address for opioid-exposed mother–infant dyads.
As reported by Salameh and Polivka, hospital unit processes that support family-centered care include education for nurses and providers about SDOH, opioid addiction, stigma related to OUD in pregnant and parenting people, and trauma-informed care. This education increases healthcare team member understanding of various contributors to OUD and decreases barriers to care for this vulnerable population. (See Trauma-informed care.)
Trauma-informed care
Salameh and Polivka describe trauma-informed care as the avoidance of retraumatizing individuals with a history of trauma. Healthcare teams that practice trauma-informed care know the signs and impact of trauma and respond with an approach that builds trust and collaboration. When caring for pregnant people with opioid use disorder (OUD), the team prevents re-traumatization by avoiding stereotypes and biases and providing a safe environment as they care for their infant with neonatal opioid withdrawal syndrome (NOWS). In 2018, the Substance Abuse and Mental Health Services Administration advised healthcare professionals to view OUD in pregnancy as a chronic condition requiring treatment and support.
When caring for pregnant people with OUD and whose infants have NOWS, healthcare teams should consider the following:
- Many pregnant and parenting people with OUD experience bias and discrimination, which may discourage them from seeking prenatal care. Eliminating barriers to care and addressing bias can help increase the use of prenatal care.
- Shared decision-making between the family and the healthcare team improves the chances for continued treatment and management of OUD.
- Recto and colleagues describe how co-morbidities, such as depression or anxiety, may exacerbate behavioral symptoms of OUD. Healthcare teams can provide appropriate referrals and treatment.
- Approaching OUD as a chronic health condition and not a moral failing increases the likelihood of consistent prenatal care and of unbiased interactions in the postpartum period.
Empathy and engagement
Postpartum and NICU nurse knowledge of trauma-informed care and the role of SDOH on the well-being of pregnant patients with OUD helps to reduce stigma and bias and supports engagement in the care of infants with NOWS. Recognizing the effects of toxic stress on mothers with OUD may lead to improved prenatal care adherence and perinatal outcomes. In addition, lower nurse-to-patient ratios aid success of the ESC model of care.
ESC depends on parental presence and engagement with the healthcare team to impact outcomes for infants with NOWS. According to Shuman and colleagues, strategies for engagement include nonjudgmental care. Grossman and colleagues recommend individual education about NOWS, ESC, and nonpharmacologic care; support of breastfeeding or breast milk feeding; and use of empowering messages and coaching in infant care. Engaging families with empathy promotes the delivery of the nonpharmacologic care that infants with NOWS need.
Michelle Slymon is an assistant professor of nursing at St. John Fisher University in Rochester, New York.
References
Achilles JS, Castaneda-Lovato J. A quality improvement initiative to improve the care of infants born exposed to opioids by implementing the Eat, Sleep, Console assessment tool. Hosp Pediatr. 2019;9(8):624-31. doi:10.1542/hpeds.2019-0144
Grossman MR, Berkwitt AK, Osborn RR, et al. An initiative to improve the quality of care of infants with neonatal abstinence syndrome. Pediatrics. 2017;139(6): e20163360. doi:10.1542/peds.2016-3360
Kroelinger CD, Rice ME, Cox S, et al. State strategies to address opioid use disorder among pregnant and postpartum women and infants prenatally exposed to substances, including infants with neonatal abstinence syndrome. MMWR Morb Mortal Wkly Rep. 2019;8(36):777-83. doi:10.15585/mmwr.mm6836a1
McGlothen-Bell K, Recto P, McGrath J, Brownell E, Cleveland L. Recovering together: Mothers’ experiences providing skin-to-skin care for their infants with NAS. Adv Neonatal Care. 2021;21(1):16-22. doi:10.1097/ANC.0000000000000819
Patrick SW, Barfield WD, Poindexter BB. Neonatal opioid withdrawal syndrome. Pediatrics. 2020;146(5):e2020029074. doi:10.1542/peds.2020-029074
Recto P, McGlothen-Bell K, McGrath J, Brownell E, Cleveland LM. The role of stigma in the nursing care of families impacted by neonatal abstinence syndrome. Adv Neonatal Care. 2020;20(5):354-63. doi:10.1097/ANC.0000000000000778
Salameh TN, Polivka B. Knowledge of and perceived competence in trauma-informed care and attitudes of NICU nurses toward mothers of newborns with neonatal abstinence syndrome. J Obstet Gynecol Neonatal Nurs. 2020;49(4):373-87. doi:10.1016/j.jogn.2020.05.003
Shuman CJ, Weber A, VanAntwerp K, Wilson R. Engaging mothers to implement nonpharmacological care for infants with neonatal abstinence syndrome: Perceptions of perinatal and pediatric nurses. Adv Neonatal Care. 2020;20(6):464-72. doi:10.1097/ANC.0000000000000812
Substance Abuse and Mental Health Services Administration. Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and Their Infants. 2018. store.samhsa.gov/sites/default/files/sma18-5054.pdf
World Health Organization. Social determinants of health. who.int/health-topics/social-determinants-of-health#tab=tab_1
Wu D, Carre C. The impact of breastfeeding on health outcomes for infants diagnosed with neonatal abstinence syndrome: A Review. Cureus. 2018;10(7),e3061. doi:10.7759/cureus.3061
Key words: Eat Sleep Console, neonatal abstinence syndrome, neonatal opioid withdrawal syndrome, family-centered care


















