Quick action prevents a negative outcome.
Takeaways:
- Cirrhosis of the liver causes scaring, shrinking, and hardening.
- Complications of cirrhosis include portal hypertension, esophageal varices, hepatic encephalopathy, jaundice, renal failure, and splenomegaly.
- Esophagogastroduodenoscopy is the gold standard for diagnosing and grading esophageal varices.
Darrel,* a 60-year-old man with acute onset of confusion, is admitted to the telemetry unit. His family had found him disheveled and rambling incoherently with dried vomit on his face.
History and assessment
Darrel has been drinking 1 pint of whiskey each day for 35 years. He worked in construction until he was terminated for absenteeism. His family reports that he’s reclusive, depressed, and hasn’t sought medical care for many years.
During your admission assessment, Darrel’s BP is 180/100 mmHg; HR, 106 beats per minute (bpm); RR, 24 breaths per minute; and temperature, 98.6° F (37° C). An ECG shows sinus tachycardia. Darrel is drowsy but arousable, incoherent, and restless. His sclera and skin are jaundiced, and you observe ascites, asterixis, decreased leg and arm muscle mass, finger clubbing, and rhonchi lung sounds. You detect hepatomegaly when you palpate Darrel’s right upper abdomen. He has an I.V. of 0.9% normal saline running at 75 mL/hr, and he’s on oxygen at 2 L by nasal cannula.
Lab results include hemoglobin 10 g/dL, platelets 126 × 103/µL, and significantly elevated liver enzymes (ALT and AST). The provider orders telemetry and for vital signs to be checked every 30 minutes. As a precaution, you set up suction in Darrel’s room.
Over the next 3 hours, Darrel’s HR rises to 154 bpm and his RR increases to 32 breaths per minute. He remains in sinus tachycardia, his O2 saturation is 89%, and his BP drops to 100/40 mm Hg. Darrel becomes more restless and agitated. He vomits 75 mL of coffee-colored emesis and his skin is pale. You activate the rapid response team (RRT).
On the scene
As the team arrives, Darrel yells out loudly and then vomits copious amounts of bright red blood. His skin is ashen, and he becomes unresponsive. You use a 16-gauge needle to start another I.V. in his right antecubital so you can infuse a wide open normal saline bolus of 250 mL and prepare to administer blood. Darrel begins responding to painful stimuli and is maintaining his airway, but you have an oropharyngeal airway at the bedside in case you need it. You evaluate his vital signs every 5 minutes.
Blood work shows that Darrel’s hemoglobin has dropped from 10 to 8.5 g/dL, with other values unchanged. Arterial blood gases show hypoxemia with PaO2 72 mmHg and SaO2 82%.
Darrel is transferred to the ICU, where he continues to bleed, passing large amounts of melena and hematemesis. The provider orders an initial I.V. bolus of octreotide 50 mcg with a continuous I.V. infusion of 50 mcg/hr.
Outcomes
Darrel is diagnosed with esophageal varices caused by decompensated end-stage liver disease. He undergoes emergent esophageal banding and ultimately recovers. Before discharge, he’s referred to a case manager who helps connect him with an addiction specialist.
Education
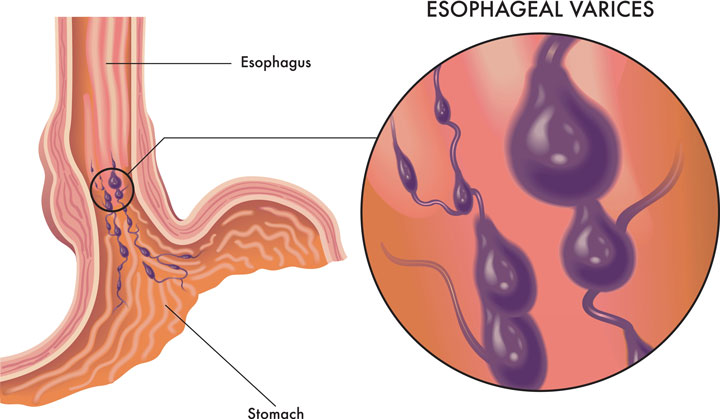
Cirrhosis of the liver increases portal hypertension, which can lead to esophageal varices—dilated submucosal veins in the esophagus. If left untreated, varices can cause life-threatening bleeding. Treatment includes vasodilator and vasoconstrictor medications, sclerotherapy, and endoscopic ligation with banding. Fluid volume resuscitation should be used to achieve and maintain a hemoglobin of 7 to 8 g/dL; however, aggressive fluid resuscitation may increase the portal pressure and cause rebleeding. To decrease the pressure, a transjugular intrahepatic portosystemic shunt can be used to reroute blood.
Patients should be referred to addiction specialists and should see a gastroenterologist for continued evaluation.
*Name is fictitious.
Donna Purviance is an assistant professor at Indiana State University in Terre Haute.
References
Ahmed Z, Ahmed U, Walayat S, et al. Liver function tests in identifying patients with liver disease. Clin Exp Gastroenterol. 2018;11:301-7. doi: 10.2147/CEG.S160537
De Franchis R, Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):743-52. doi:10.1016/j.jhep.2015.05.022
Fischbach FT, Fischbach MA. Fishbach’s A Manual of Laboratory and Diagnostic Tests. 10th ed. Philadelphia, PA: Wolters Kluwer; 2017.
Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2017;65(1):310-35. doi:10.1002/hep.28906
Hwang JH, Shergill AK, Acosta RD, et al. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 2014;80(2):221-7. doi:10.1016/j.gie.2013.07.023
Kothari HG, Gupta SJ, Gaikwad NR, Sankalecha TH, Samarth AR. Role of non-invasive markers in prediction of esophageal varices and variceal bleeding in patients of alcoholic liver cirrhosis from central India. Turk J Gastroenterol. 2019;30(12):1036-43. doi:10.5152/tjg.2019.18334
Lesmana CRA, Raharjo M, Gani RA. Managing liver cirrhotic complications: Overview of esophageal and gastric varices. Clin Mol Hepatol. 2020;26(4):444-60. doi:10.3350/cmh.2020.0022
Rockey DC, Elliott A, Lyles T. Prediction of esophageal varices and variceal hemorrhage in patients with acute upper gastrointestinal bleeding. J Investig Med. 2016;64(3):745-51. doi:10.1136/jim-2015-000047
Sanyal AJ. Primary and pre-primary prophylaxis against variceal hemorrhage in patients with cirrhosis. UpToDate. December 23. 2019. uptodate.com/contents/primary-and-pre-primary-prophylaxis-against-variceal-hemorrhage-in-patients-with-cirrhosis
Sanyal AJ, Bajaj JS. Prevention of recurrent bleeding from esophageal varices in patients with cirrhosis. UpToDate. December 15, 2020. uptodate.com/contents/prevention-of-recurrent-bleeding-from-esophageal-varices-in-patients-with-cirrhosis

















