Self-management education is the foundation of osteoarthritis care.
Takeaways:
· Osteoarthritis is a chronic disorder of the joints that is painful, prevalent, costly, and a leading cause of disability.
· Management of osteoarthritis is multifaceted and includes nonpharmacologic, pharmacologic, and surgical interventions.
· Nurses are ideally positioned to promote evidence-based management of osteoarthritis in primary care settings as well as in specialty rheumatology and orthopedic surgery settings.
OSTEOARTHRITIS (OA) is a painful, chronic joint disorder that primarily affects the hands, knees, hips, and spine. It affects the entire joint, including the cartilage, subchondral bone beneath the cartilage, synovium or joint lining, ligaments and menisci, and muscles around the joint. Biomechanical risk factors associated with OA, such as obesity, muscle weakness, joint injury, and malalignment, result in chemical changes within the joint, which thin and erode the cartilage and result in a narrowed joint space, osteophytes, or bone spurs at joint margins. The synovium becomes inflamed, ligaments become lax, menisci in the knee degenerate, and the muscles become weak and atrophy. These structural changes contribute to pain and impaired function. (See OA facts and figures.)
OA management and patient education—including self-management and pharmacologic and non-pharmacologic recommendations— requires that nurses stay up-to-date with evidence-based practice.

Risk factors
OA risk factors can be categorized as personal and joint-related. Personal factors include genetics, increasing age, female gender, obesity, bone mineral density, and diet. Joint-related factors include a history of joint injury, muscle weakness, malalignment, unequal leg length, bone/joint defects, vigorous physical activity or sports, and occupations requiring squatting, kneeling, lifting, standing, or repetitive motions. Several conditions, such as metabolic disorders (hyperparathyroidism or hemochromatosis), hypermobility syndromes (Ehlers-Danlos syndrome or Marfan syndrome), and crystal arthritis can predispose individuals to OA. Many of these risk factors aren’t modifiable, but reducing obesity, preventing joint injury, and changing occupational exposure can reduce the likelihood of developing OA, decrease its symptoms, and slow its progression.
Signs and symptoms
OA symptoms vary and usually progress slowly. They include pain, stiffness, and impaired function specific to the affected joint. Pain is related to using the joint and can worsen during the day. Morning stiffness lasts less than 30 minutes; stiffness also may occur after inactivity and is called gelling. Signs of OA are crepitus or a crackling sound with joint movement, joint swelling, reduced joint range of motion, limited movement, bony enlargement of the joint, and joint instability. (See Joint by joint.)
Joint by jointSigns and symptoms of osteoarthritis (OA) are joint specific. Hands Typically, OA affects several joints in both hands, with bony enlargement related to the involved joints. For example, when the distal interphalangeal joints are affected, the bony enlargement is referred to as Heberden’s nodes; Bouchard’s nodes refer to bony enlargement of the proximal interphalangeal joints. When the first carpometacarpal (CMC) joint (the joint at the base of the thumb) is involved, hand function is limited. The first CMC joint may appear squared because of osteophytes.  Knees Patients with knee OA report pain, stiffness, and difficulty with activities such as walking, transferring, and stair climbing. They may report that their knee feels unstable, which may result in a fear of falling. Crepitus, bony tenderness, and bony enlargement are found on physical examination. Severe disease can lead to joint malalignment. A varus deformity occurs when the distal part of the leg below the knee deviates inward (bow-legged) and a valgus deformity occurs when it deviates outward (knock-kneed). 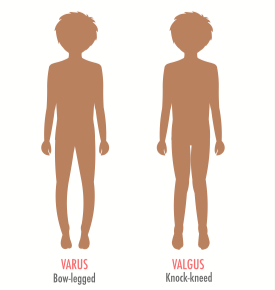 Hips Patients with hip OA report groin pain, although discomfort in the thigh, buttock, low back, and knee also may occur. Patients have difficulty with activities such as walking, transferring from sitting to standing, climbing stairs, and bending. Physical examination shows limited internal hip rotation. With severe disease, patients experience reduced range of motion, hip flexion contracture, and hip deformity. 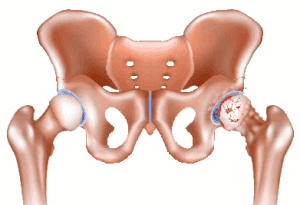 Spine Patients experience pain in the region affected by spine OA. In cervical spine OA, pain is felt in the neck, which may radiate down the arms. If cervical spine nerves are compressed, patients may report weakness or abnormal sensations in their arms. Low back pain is the hallmark of lumbosacral spine OA, and osteophytes and disc space narrowing may compress the sciatic nerve, resulting in pain, numbness, and leg weakness. 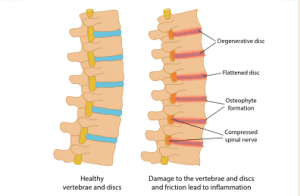 |
Pain and impaired function can adversely affect employment, mood, and participation in social activities. Depression and anxiety are common comorbidities in patients with OA. A meta-analysis by Stubbs and colleagues reported that the prevalence of depression and anxiety symptoms in patients with OA was 19.9% and 21.3%, respectively. Machado and colleagues noted significant positive correlations between physical symptoms of OA and depression symptoms (r=0.48), activity limitations (r=0.53), and social and leisure participation restrictions (r=0.55).
Depression and activity limitations act as mediators between physical symptoms of OA and participation restrictions. Agarwal and colleagues found that a greater pro- portion of patients with OA and co-morbid depression reported fair or poor perceived physical health (42.8% vs. 20.9%), fair or poor perceived mental health (32.7% vs. 8.6%), and anxiety (26.7% vs. 9.4%) compared with patients with OA without depression.
OA management
The focus of OA management is on promoting self-management, reducing pain, improving function, and modifying the disease process and its effects. An interdisciplinary team approach can include self-management education, psychosocial assessment and interventions to man- age depression and anxiety, dietary therapy, physical and occupational therapy, pharmacotherapy, and surgical interventions.
Published clinical guidelines provide recommendations for managing hand, knee, and hip OA, including nonpharmacologic and pharmacologic interventions. Recommendations for managing spine OA aren’t published, but the American College of Rheumatology provides some strategies for living well with cervical (bit.ly/2tI3k88) and lumbosacral OA (bit.ly/2tFWXlR) that nurses can share with patients.
The American College of Rheumatology offers the following strong and conditional recommendations for hand, knee, and hip OA, which nurses can use to guide care. The strength of a recommendation as strong or conditional is based on the quality of the current evidence supporting the intervention and the degree to which the benefits outweigh the risks.
Hands
Conditional nonpharmacologic recommendations: Assess activities of daily living (ADLs) and teach patients about joint-protection strategies (such as avoid pinching and gripping, balance rest and activity, change positions) and how to use thermal therapies to manage pain. Recommend ADL assistive devices, including grabbers, key turners, jar openers, button aids, zipper pulls, sock aids, and long-handled shoehorns. Providers may order a splint for patients with first carpometacarpal joint OA.
Conditional pharmacologic recommendations: Topical capsaicin (the active component in chili peppers), oral and topical nonsteroidal anti-inflammatory drugs (NSAIDs), and tramadol (a synthetic opioid agonist). Opioid analgesics and intraarticular injections with corticosteroids or hyaluronates should not be used.
Knees
Strong nonpharmacologic recommendations: Aquatic, aerobic, and resistance exercises are recommended based on individual patient ability and preference. Weight loss is recommended for patients who are overweight.
Conditional nonpharmacologic recommendations: Encourage patients to participate in self-management education programs, including psychosocial interventions and tai chi classes. Patients can use thermal therapies and manual physical ther- apy in conjunction with exercise supervised by a physical therapist. Walking aids and medially directed patellar taping can be used, if indicated. A cane can decrease joint loading, but it should be properly fitted by a physical therapist and instructions provided for its use. (The cane is held in the hand contralateral to the affected limb and moves together with the affected limb. When ascending stairs, the contralateral limb leads; when descending, the affected limb and cane lead.)
Depending on the knee compartment affected, insoles can be used. Patients with lateral compartment OA (valgus knee OA) can wear medially wedged insoles and those with medial compartment OA (varus knee OA) can wear laterally wedged subtalar strapped insoles. Traditional Chinese acupuncture and transcutaneous electrical nerve stimulation (TENS) are conditionally recommended only when patients have chronic moderate to severe pain and are unwilling or unable to undergo total knee replacement surgery.
Conditional pharmacologic recommendations: Acetaminophen, oral and topical NSAIDs, tramadol, and intraarticular corticosteroid injections. Currently, no evidence supports using topical capsaicin or nutritional supplements (such as chondroitin sulfate and glucosamine).
Hips
Strong nonpharmacologic recommendations: Nonpharmacologic recommendations include aquatic, aerobic, and/or resistance exercises, based on the patient’s ability and preference. Weight loss is recommended for patients who are overweight.
Conditional nonpharmacologic recommendations: Encourage patients to participate in self-management education programs, which may include psychosocial interventions. Patients can use thermal therapies and manual physical therapy in conjunction with exercise supervised by a physical therapist. Walking aids can be used, if indicated.
Conditional pharmacologic recommendations: Acetaminophen, oral NSAIDs, tramadol, and intraarticular corticosteroid injections. Nutritional supplements, such as chondroitin sulfate and glucosamine, should not be used.
Medication precautions
Age, concomitant medications, medication contraindications, and medication side effects play important roles in pharmacologic recommendations.
Acetaminophen: When providers recommend that patients take the full dose of 4,000 mg/day of acetaminophen, explain to patients that they should avoid taking other medications with acetaminophen (including cold remedies and combination medications with acetaminophen) to prevent acetaminophen-related hepatotoxicity.
Topical capsaicin: Instruct patients to wear gloves when applying topical capsaicin to affected joints and to avoid touching their eyes and mucous membranes with the medication. Common adverse reactions of capsaicin are local burning and skin irritation.
NSAIDs: Contraindications to oral NSAIDs include severe chronic renal disease and cardiovascular comorbidities. The recommendation for patients with a history of upper-GI ulcer but no upper-GI bleeding in the last year is either a cyclooxygenase 2 (COX-2) selective inhibitor or a nonselective NSAID plus a proton-pump inhibitor. For patients with a history of an upper-GI ulcer and bleeding in the last year, a COX-2 selective inhibitor plus a proton-pump inhibitor is recommended.
Patients who are taking low-dose aspirin (≤ 325 mg/day) should start with a nonselective NSAID other than ibuprofen plus a proton-pump inhibitor. Ibuprofen interacts with low-dose aspirin to reduce its effectiveness in preventing strokes and myocardial infarctions.
Teach patients taking NSAIDs to monitor and report side effects including stomach distress or bleeding, protein in the urine, high cholesterol, high blood pressure, edema, chest pain, shortness of breath, weakness in one part or side of the body, slurred speech, and rashes. Patients 75 years and older should use topical rather than oral NSAIDs.
Intraarticular corticosteroid injections: These injections of methylprednisolone or triamcinolone can be given up to three times per year by trained healthcare providers to manage painful knee and hip OA flare-ups. When injected into the joint space, these medications temporarily relieve pain by reducing the cells and fluid involved in the inflammatory process. Hip joint injections may require ultrasound or fluoroscopy guidance.
Opioids: For patients with pain not controlled by nonpharmacologic and pharmacologic interventions and who are unwilling or unable to undergo total joint replacement, duloxetine (a serotonin-norepinephrine reuptake inhibitor) and opioid analgesics are recommended. However, follow the American Pain Society/American Academy of Pain Medicine guidelines for using opioid analgesics to manage chronic noncancer pain.
Thermal therapies
Thermal (cold and superficial heat) therapies can be used alone or as adjuncts to physical therapy and exercise. Cold reduces pain and swelling associated with inflammation by constricting blood flow in the joint and surrounding tissues and slowing nerve conduction. It can be applied for 10 to 30 minutes using ice packs, cold baths, or vapor-coolant sprays. Superficial heat increases the pain threshold, reduces muscle spasm, and decreases pain at free nerve endings. It can be applied for about 20 minutes and includes hot packs, paraffin baths, hydrotherapy, and radiant heat.
Exercise
Patients with knee or hip OA can be referred to a physical therapist for evaluation and exercise supervision, including therapeutic exercises for flexibility and strengthening and for aerobic exercises. Exercise reduces the risk of cardiovascular disease and obesity and improves aerobic fitness, which benefits adults with OA who are at risk for other comorbidities. It helps maintain joint flexibility and reduces pain and joint swelling.
For patients with knee OA, exercise improves quadricep muscle strength on the anterior thigh, which helps to stabilize the knee joint and promotes physical function. Exercise also can help reduce depression symptoms. Despite these benefits, about half of adults with knee OA are physically inactive.
Aerobic exercise
Aquatic exercise, stationary cycling, and walking are safe and effective activities that don’t cause undue joint stress. Instruct sedentary patients to gradually increase physical activity duration to avoid aggravating OA symptoms. They can slowly advance their physical activity goals to meet the national guideline of 30 minutes of moderate-intensity physical activity on most days of the week.
Some patients may be motivated by wearing a step counter that registers steps taken, either on the device itself or through a smartphone app.
Self-management education
OA patients benefit from self-management education, but according to Healthy People 2020, only 11.4% of adults with arthritis received evidence-based arthritis education in 2014. This interactive intervention builds skills such as goal setting, decision-making, self-monitoring, and problem-solving. Self-management programs are led by healthcare professionals, sometimes along with nonprofessional lay leaders, who have received comprehensive in-person training to deliver the program content using a detailed manual. These programs can be provided to patients and their families in clinical or community settings. More recently, Spanish-language, online, and self-study versions have become available.
Target behaviors for self-management education include physical activity, communication with healthcare providers, cognitive symptom management, problem-solving, and action planning. The most widely studied arthritis-related self-management education interventions, the Arthritis Self-Management Program (2 hours per week for 6 weeks), and the Chronic Disease Self-Management Program (2.5 hours per week for 6 weeks), have shown positive outcomes in self-efficacy (confidence that the behavior of interest can be performed under certain conditions); self-rated health; aerobic exercise; cognitive symptoms management; and patient-reported outcomes for pain, function, fatigue, and mood. (See Evidence-based resources.)
Evidence-based resourcesEvidence-based activity and self-management education programs can help pa- tients manage osteoarthritis. The Centers for Disease Control and Prevention has designated the following programs as recommended or promising. Physical activity programs Recommended
Promising
Self-management education programs Recommended
Promising
Source: cdc.gov/arthritis/interventions/physical-activity.html |
Psychosocial assessment and interventions
Depression and anxiety can negatively affect social and leisure participation in patients with OA. Items from the National Institutes of Health’s Patient-Reported Outcomes Measurement Information System (healthmeasures.net/explore-measurement-systems/promis) can be used as part of your assessment. For example, ask patients how often in the past 7 days they felt cheerful and if they’re satisfied with their current level of social activity. The answers can help identify psychological distress.
Psychosocial interventions can help patients manage pain, reduce depression and anxiety, and improve social and leisure participation. These interventions, provided by trained nurses, social workers, and psychologists, educate patients about the important role thoughts and behaviors play in managing pain and mood, and show patients how to use coping skills, such as relaxation, imagery, activity-rest cycling, and cognitive restructuring.
Surgical interventions
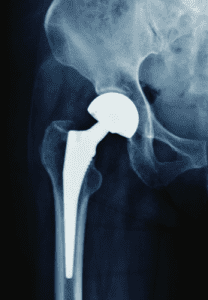
Most patients with OA will not need a total joint replacement, which is indicated for patients with knee or hip OA who have pain at night that does not respond to NSAIDs, have difficulty performing ADLs, and have significant problems with mobility and working. Total joint replacements have positive results in many patients. (See Hip replacement.) The American Academy of Orthopaedic Surgeons provides extensive online information about total knee (orthoinfo.aaos.org/en/treatment/total-knee-replacement) and hip replacement (orthoinfo.aaos.org/en/treatment/total-hip-replacement).
Evidence-based care
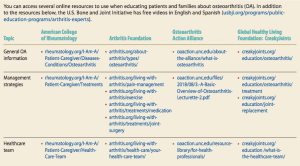
OA management is multifaceted and includes nonpharmacologic, pharmacologic, and surgical interventions. As evidence grows, clinical guidelines will be updated. Nurses should stay alert for updates so that they can incorporate the latest recommendations along with their clinical expertise in conjunction with patient values and preferences to provide evidence-based patient care. (See OA resources.)
OA resources
The authors work at the University of Pittsburgh school of nursing in Pittsburgh, Pennsylvania. Elizabeth A. Schlenk is an associate professor and Xiaojun Shi is a PhD student.
Selected references
Agarwal P, Sambamoorthi U. Healthcare expenditures associated with depression among individuals with osteoarthritis: Post-regression linear decomposition approach. J Gen Intern Med. 2015;30(12):1803-11.
Arthritis, osteoporosis, and chronic back conditions. Office of Disease Prevention and Health Promotion. healthypeople.gov/2020/topics-objectives/topic/Arthritis-Osteoporosis-and-Chronic-Back-Conditions/objectives
Bitton R. The economic burden of osteoarthritis. Am J Manag Care. 2009;15(suppl 8):S230-5.
Brady T. Strategies to support self-management in osteoarthritis: Five categories of interventions, including education. Orthop Nurs. 2012;31(2):124-30.
Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009; 10(2):113-30.
Cisternas MG, Murphy L, Sacks JJ, Solomon DH, Pasta DJ, Helmick CG. Alternative methods for defining osteoarthritis and the impact on estimating prevalence in a US population-based survey. Arthritis Care Res. 2016; 68(5):574-80.
Deshpande BR, Katz JN, Solomon DH, et al. Number of persons with symptomatic knee osteoarthritis in the US: Impact of race and ethnicity, age, sex, and obesity. Arthritis Care Res. 2016;68(12):1743-50.
Dunlop DD, Song J, Semanik PA, et al. Objective physical activity measurement in the osteoarthritis initiative: Are guidelines being met? Arthritis Rheum. 2011;63(11):3372-82.
Fernandes L, Hagen KB, Bijlsma JW, et al. EULAR recommendations for the non- pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72(7):1125-35.
Geenen R, Overman CL, Christensen R, et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77(6):797-807.
Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012;64(4):465-74.
McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014;22(3):363-88.
Machado GP, Gignac MA, Badley EM. Participation restrictions among older adults with osteoarthritis: A mediated model of physical symptoms, activity limitations, and depression. Arthritis Rheum. 2008;59(1):129-35.
Management of Osteoarthritis of the Hip: Evidence-based Clinical Practice Guideline.American Academy of Orthopaedic Surgeons. March 13, 2017. aaos.org/uploadedFiles/PreProduction/Quality/Guidelines_and_Reviews/OA%20Hip%20CPG_11.1.17.pdf
Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: The chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin Arthritis Rheum. 2014;43(6):701-2.
Nelson AE, Jordan JM. Clinical features of osteoarthritis. In: Firestein GS, Budd RC, Gabriel SE, McInnes IB, O’Dell JR, eds. Kelley and Firestein’s Textbook of Rheumatology. 10th ed. Philadelphia, PA: Elsevier; 2017:1705-18.
Neogi T, Zhang Y. Epidemiology of osteoarthritis. Rheum Dis Clin North Am. 2013; 39(1):1-19.
Osteoarthritis. Arthritis Foundation. arthritis.org/about-arthritis/types/osteoarthritis
Osteoarthritis. National Institute of Arthritis and Musculoskeletal and Skin Diseases. May 30, 2016. niams.nih.gov/health-topics/osteoarthritis
Stubbs B, Aluko Y, Myint PK, Smith TO. Prevalence of depressive symptoms and anxiety in osteoarthritis: A systematic review and meta-analysis. Age Ageing. 2016;45(2): 228-35.
Treatment of Osteoarthritis of the Knee: Evidence-based Guideline. American Academy of Orthopaedic Surgeons. 2nd ed. May 18, 2013. aaos.org/research/guidelines/TreatmentofOsteoarthritisoftheKneeGuideline.pdf
Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26(3):355-69.
ant5-CE Osteo-417

















4 Comments.
It’s evident that the medical community will notice an increase in osteoarthritis in our aging population. Ongoing reviews allows nursing practices to stay on top of evidence based medicine and the trending diseases we see daily in these aging populations. My area is outpatient/clinic practice, and as first line nursing it’s very important to have tools to educate, dispell myths and provide support in the management of diseases.
Can osteoarthritis develop at a young age?
Thank you for the very useful information!
I received this journal and read this CEU-earning article, but when I try to register and take the test, the computer does not allow me to purchase at checkout. The little circle just goes around endlessly. I would appreciate if someone could contact me (through my email below) to see what the problem is.
Thanks,
Susan