
Takeaways:
- All healthcare providers should possess primary palliative care are skills; secondary palliative care is used for complex symptoms, difficult discussions, and assistance with hospice transition.
- HEART—History of admissions, Echocardiogram results, Activity intolerance, Refractory symptoms, and Tired caregivers—helps nurses identify patients with heart failure who need palliative care support.
- Palliative and hospice care are distinct disciplines; patients can and should receive palliative care management regardless of enrollment in hospice.
According to the Centers for Disease Control and Prevention, about 6.5 million adults in the United States have heart failure (HF), which is associated with a heavy symptom burden and periods of decompensation that lead to frequent hospitalization, especially with end-stage disease. (See Classifying heart failure.) Consulting palliative care teams to help with this complex syndrome has gained attention recently, with an emphasis on providing an additional layer of support for patients, caregivers (families and friends providing care), and family members. Unfortunately, many patients, caregivers, cardiologists, and primary care providers don’t accept palliative care because they associate it with hospice, not understanding the distinction between the two. (To learn more about the difference between palliative and hospice care, click here.) However, evidence-based guidelines and public opinion call for increased use of palliative care. HF societies in North America and Europe advocate for a paradigm shift from a prognosis-focused to a symptom-focused model of care, promoting palliative care (also called supportive care) consults.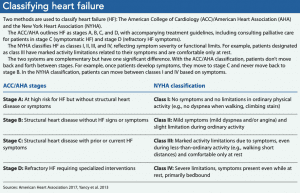
Palliative care teams integrate the medical, psychological, and spiritual aspects of care for patients and support caregivers and family members. These interdisciplinary team members may participate in daily rounding, exploring patients’ understanding of their illness, discussing the prognosis, clarifying care goals, navigating treatment options, and managing symptoms. Palliative care teams also assist with coordinating care and planning end-of-life wishes, including determining the need and timing for hospice care.
As nurses, we’re responsible for advocating for patients and their family members when needs are unmet and quality of life is jeopardized. This article explains the differences between primary and specialty palliative care and when a consult is appropriate. It also discusses using the HEART (History of readmissions, Echocardiogram staging, Activity intolerance, Refractory symptoms, Tired caregiver) acronym as a strategy to trigger awareness of when a palliative care consult is beneficial.
Primary and specialty palliative care
All healthcare providers interacting with patients should possess primary palliative care skills—educating patients about the disease process and prognosis, addressing basic symptom needs, initiating discussions about advance care planning, and reviewing care goals during hospitalization. Specialty palliative care focuses on managing complex symptoms, negotiating difficult discussions about advance care planning, and assisting with transitions to hospice. Currently, no formal guidelines exist for consulting specialty palliative care, but there are several clear indications that nurses can use as a guide. Keep in mind, the inclusion of specialty palliative care doesn’t exclude the nurses’ role in primary palliation.
Current literature suggests that nurses embrace specialty palliative care, but obstacles prevent us from requesting it. Specialty palliative care consults require provider approval, but some providers don’t value this care and deny nurses’ requests. When that happens, nurses may feel they’ve lost credibility with the provider and avoid asking for palliative care in the future. Distinguishing between primary and specialty palliative care needs can be challenging, leading to missed opportunities by healthcare teams to improve care management. In addition, according to the Center to Advance Palliative Care, approximately 60% of U.S. hospitals with 50 or more beds have palliative care teams but struggle to meet care demands. And many rural health systems don’t offer palliative care services, leaving a void in the care management team that results in unwanted procedures and services and poor quality of life.
HEART
Using the HEART acronym can help nurses recognize triggers that may indicate the need for a specialty palliative care consult for patients with HF.
History of readmissions
According to the American Heart Association, HF accounts for 990,000 hospital discharges annually and is ranked as the top discharge diagnosis in older patients. The chronicity of HF, paired with multiple complex comorbidities, predisposes patients to frequent hospitalizations with subsequent readmission. A study by Bergethon and colleagues found that about half of patients with HF are rehospitalized within 6 months of discharge, and 70% of the rehospitalizations are due to worsening HF.
Despite medical advances in HF management, frequent readmissions occur, which are concerning for patients, families, and providers. Patients are readmitted for a variety of reasons, including uncontrolled physical and psychological symptoms, unavoidable illness progression, diligent but imperfect self-care adherence, and care management failures. Many nurses know patients with HF by name because of the repeated admissions. Hospital readmissions are a trigger for palliative care consults, even if the patient is admitted for another diagnosis but also has HF.
Echocardiogram staging
Echocardiograms (echos) are a key HF diagnostic and management tool. They’re used to measure ventricular function, identify structural heart disease and morphologic changes, and guide therapy. Echos provide a wealth of diagnostic information, but the left ventricular ejection fraction (LVEF) is used to stage HF.
The normal LVEF range is between 55% to 70% and reflects the percentage of blood pumped out during systole. For example, an LVEF of 45% indicates that 45% of the total amount of blood in the left ventricle is pumped out. An LVEF of 40% to 54% is slightly below normal; 35% to 39% is moderately below normal; less than 35% is severely below normal and associated with increased risk of life-threatening rhythms.
Nurses can glean information from the echo to help support their request for specialty palliative care. For example, they can look for heart failure and reduced ejection fraction (HFrEF) vs. heart failure and preserved ejection fraction (HFpEF). When the heart muscle is weak, the condition is known as HFrEF; if the heart pumps normally but is stiff and can’t fill properly, the condition is known as HFpEF.
HFrEF is easily identified by echo: When the LVEF is less than 40%, patients typically have accompanying symptoms of dyspnea, decreased exercise tolerance, and edema. Unfortunately, HFpEF is a greater challenge to recognize by echo because the LVEF is reported at 50% or greater even though these patients typically present with symptoms similar to HFrEF, making them candidates for palliative care.
When nurses use the LVEF value and reports of uncontrolled HF symptoms, they can feel confident in their request for a specialty palliative care consult, especially for patients with HFrEF.
Activity intolerance
Activity (including exercise and activities of daily living) intolerance is a complicated phenomenon reported by many patients with HF. It’s directly related to reduced oxygen supply from the cardiovascular system and is a major HF symptom. It’s also an independent predictor of prognosis and decreased quality of life. Reduced LVEF with HFrEF or ventricular stiffness with HFpEF leads to low-grade systemic inflammation and insulin resistance. These factors contribute to loss of muscle mass, further compromising the patient’s ability to participate in activities.
The 2013 American College of Cardiology Foundation/American Heart Association (ACCF/AHA) Guideline for the Management of Heart Failure recommends including cardiac rehabilitation (rehab), but many patients with end-stage HF can’t tolerate these activities. For example, a patient with HF who has a 4-lb (1.8 kg) weight gain within 3 days won’t benefit from or be able to participate in cardiac rehab because weight gain within a short time while receiving medication therapy might be the result of a cycle of chronic HF exacerbation. Other factors that make rehab inappropriate include concurrent, continuous, or intermittent dobutamine therapy; a drop in systolic blood pressure with activity; supine resting heart rate at or above 100 beats per minute; ventricular arrhythmias at rest or with activities; and concurrent comorbidities that limit activity, such as pulmonary disease. Any one of these factors is a strong indicator for a specialty palliative care consultation.
Many patients and caregivers don’t understand how HF affects activities of daily living, resulting in depression, anxiety, and frustration as patients become more reliant on caregivers. The palliative care team can facilitate conversations between the patients and caregivers, help set activity goals to reduce caregiver strain, and promote a level of independence for the patient.
Refractory symptoms
Refractory symptoms—such as dyspnea, fatigue, and pain—are those that can’t be adequately controlled with regularly prescribed medications.
Dyspnea. Many patients with HF report dyspnea as a dominant symptom, occurring at rest or with minimal activities even with maximum pharmacologic therapy. Dyspnea impairs functional capacity and quality of life independent of disease severity. Dyspnea in patients with HF is thought to be associated with pulmonary congestion resulting in reduced LVEF. Providers will prescribe diuretics to reduce pulmonary congestion, but the sensation of dyspnea is multifactorial and may be related to chronically elevated systemic inflammation and psychologic distress.
Fatigue. Fatigue—physical and psychological—is primarily caused by decreased cardiac output, but it also can be associated with deconditioning, poor sleep cycles, and depression or anxiety.
Pain. According to Alemzadeh-Ansari and colleagues, pain prevalence in patients with HF varies from 23% to 85%. The most common pain site is in the legs below the knees, which is theorized to be the result of cytokines and inflammatory markers that contribute to the presence of pain and how the body perceives it. Patients also report back, major joint, and chest pain, and many patients have pain in more than one area.
Other refractory symptoms include nausea, anorexia, depression, and anxiety. Patients with end-stage HF also may demonstrate protein malnutrition and cachexia.
Palliative consultation and assistance with refractory symptom management extends beyond routinely prescribed angiotensin-converting enzyme inhibitors, beta blockers, and diuretics. It also may include opiates (short-acting and extended-release morphine), antianxiety medications (such as clonazepam), and other integrative therapies. For example, the benefits of massage therapy recently have been explored and supported for reducing the physiologic and psychologic symptoms associated with HF. This therapy can be initiated by the caregiver, engaging them in an initial intervention to help reduce the patient’s symptoms. Another option is using guided imagery to reduce dyspnea. This mind-body intervention uses imagination to promote relaxation and improve overall well-being.
Tired caregiver
Many studies show that caregivers are vital for patients with HF. These caregivers assist patients with emotional, cognitive, and physical function and play a key advocacy role. Although they typically don’t receive any formal education on how to provide appropriate care, they’re expected to perform consistent surveillance to prevent patient decompensation.
According to the National Alliance for Caregiving and the AARP Public Policy Institute, most caregivers have their own health and well-being problems, either pre-existing or arising from their caregiving role. They’re frequently overwhelmed by varying emotions as the final months of the patient’s life approach.
Evidence of a tired caregiver include physical decline, signs of depression or anxiety, social isolation, and diminished self-care. Frequently, nurses are witnesses to the emotional and physical toll on caregivers. With no break, caregivers ultimately experience a loss of resilience, and unmet needs ignored by the healthcare team further intensify the caregiver’s strain and burden.
The palliative care team can provide education to help caregivers manage refractory symptoms, support them during decision-making, and assist with care transition. Psychological support for caregivers of patients with HF is the responsibility of the patient’s healthcare team, including the direct patient care nurse. In addition to active listening and serving as a constant presence for the patient and family, nurses can offer periods of respite for tired caregivers with chaplain visits, meals off of the unit, and companionship in the family member’s absence.
Be the voice
Nurses, who are vital to primary palliative care for patients with HF and their caregivers, usually are the first healthcare team members to recognize unmet needs that can be addressed by specialty palliative care. Nurses can be the voice for patients and caregivers by requesting inclusion of these services.
The authors work at the College of Behavioral, Social, & Health Science School of Nursing in Clemson, South Carolina. Tracy Fasolino is an associate professor. Megan E. Mayfield is a lecturer.
References
Alemzadeh-Ansari MJ, Ansari-Ramandi MM, Naderi N. Chronic pain in chronic heart failure: A review article. J Tehran Heart Cent. 2017;12(2):49-56.
American Heart Association. Classes of heart failure. May 31, 2017. heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure
Ashley J, Fasolino T. Palliative and hospice care: Educational needs of inpatient registered nurses. Creative Nursing. 2016;22(2):1-7.
Bergethon KE, Ju C, DeVore AD, et al. Trends in 30-day readmission rates for patients hospitalized with heart failure: Findings from the Get With the Guidelines—Heart Failure Registry. Circ Heart Fail. 2016;9(6):e002594.
Brunjes DL, Kennel PJ, Schulze PC. Exercise capacity, physical activity, and morbidity. Heart Fail Rev. 2017;22(2):133-9.
Center to Advance Palliative Care. America’s care of serious illness. 2019 state-by-state report card on access to palliative care in our nation’s hospitals. September 2019. reportcard.capc.org
Centers for Disease Control and Prevention. Heart disease: Heart failure. December 9, 2019. cdc.gov/heartdisease/heart_failure.htm
Fasolino T. Using guided imagery to address dyspnea and spiritual peace for end-stage heart failure patients: An interdisciplinary approach. J Pain Symptom Manage. 2020;59(2):468-9.
Given BA, Reinhard SC. Caregiving at the end of life: The challenges for family caregivers. Generations. 2017;41(1):50-7.
Haykowsky MJ, Daniel KM, Bhella PS, Sarma S, Kitzman DW. Heart failure: Exercise-based cardiac rehabilitation: Who, when, and how intense? Can J Cardiol. 2016;32(10 suppl 2):S382-7.
Marwick TH. The role of echocardiography in heart failure. J Nucl Med. 2015;56(Suppl 4):31S-8S.
McKelvie RS, Moe GW, Cheung A, et al. The 2011 Canadian Cardiovascular Society heart failure management guidelines update: Focus on sleep apnea, renal dysfunction, mechanical circulatory support, and palliative care. Can J Cardiol. 2011;27(3):319-38.
Modin D, Andersen DM, Biering-Sørensen T. Echo and heart failure: When do people need an echo, and when do they need natriuretic peptides? Echo Res Pract. 2018;5(2):R65-79.
Montero D, Diaz-Cañestro C. Determinants of exercise intolerance in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Int J Cardiol. 2018;254:224-9.
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation. 2016;133(4):e38-360.
National Alliance for Caregiving, AARP Public Policy Institute. Caregiving in the U.S. 2020. Washington, DC: AARP Public Policy Institute; 2020. caregiving.org/caregiving-in-the-us-2020
Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation. 2020;141(9):e139-596.
Whellan DJ, Goodlin SJ, Dickinson MG, et al. End-of-life care in patients with heart failure. J Card Fail. 2014;20(2):121-34.
Yancy CW, Jessup M, Casey DE, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: Executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.2013;128(16):1810-52.


















1 Comment.
Ottimo articolo… !
Il paziente ha diritto di vivere l’ultimo periodo della propria vita con dignità. Dobbiamo dunque condividere il progetto di qualità della cura e applicare nella pratica quotidiana le cose che abbiamo studiato…