
Teach patients with diabetes this essential tool for self-care.
Takeaways:
- Carbohydrate counting can be a challenging skill for both nurses and patients.
- Nurses have an important role to play providing education and supporting patients with diabetes.
- Many diet, carbohydrate, and diabetes management tools and resources are available to aid nurses and patients.
Mr. Tucker,* a 20-year-old man with type 1 diabetes, is admitted to the hospital for a severe hypoglycemic event. For about a month, he’s experienced these events about twice a week at various times throughout the day. His endocrinologist wants him to go home on a new insulin-to-carbohydrate ratio (ICR) regimen. Before Mr. Tucker is discharged, he’ll need to understand how to count carbohydrates and how to administer insulin based on an ICR. As his bedside nurse, are you prepared to provide this education?
In the United States, over 34 million Americans have diabetes. To avoid the many consequences of poor diabetes management, patients must know how to care for themselves at home. However, many nurses may be uncomfortable teaching about carbohydrate counting and ICRs. Knowledge of carbohydrates, their importance in diabetes management, and counting methods may ease some of this discomfort so you can properly educate patients.
Carbohydrates explained
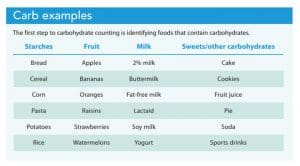
All foods are a combination of three micronutrients—carbohydrates (carbs), proteins, and fats—that our bodies use for energy. Three types of carbs—starches, dietary fiber, and sugars—can be found in grains, fruits, starchy vegetables, milk, and sweets.
Ultimately, all carbs breakdown into glucose for energy, raising blood glucose levels. In healthy bodies, insulin stimulates glucose absorption by muscle and adipose tissue to lower these levels. For individuals with diabetes, their bodies can’t create insulin, can’t use it, or both.
All patients have unique nutritional needs related to lifestyle and clinical status. The American Diabetes Association (ADA) recommends seeking guidance from a registered dietitian nutritionist (RDN) for the best nutrition management. Work with the RDN to support and reinforce your diet education with patients, and share information about the patient’s behaviors and eating patterns to help the RDN individualize the patient’s dietary plan.
Providers may order a consistent carbohydrate diet to help manage diabetes. This plan requires the patient to eat about the same amount of carbs at each meal to maintain stable blood glucose levels. According to the ADA, carbohydrate reduction has the most evidence for improving glucose levels over time.
When you talk with Mr. Tucker about what he eats at home, he says that he typically avoids regular soda and candy and that he knows certain foods—such as pasta and bread—can increase his blood sugar. He hasn’t been keeping a food diary or log of his meals. While in the hospital, he’s noticed that he’s receiving smaller amounts of food than he usually eats at home. You explain that a consistent carbohydrate diet will help maintain stable blood glucose throughout the day.
Managing carbohydrates
You can describe carbohydrate amounts as servings (an estimate) or grams (a specific measurement). For example, one slice of bread, which contains 12 grams of carbohydrate, is one carbohydrate serving. To determine the specific carbohydrate grams in a food, patients should read food labels. However, reading food labels can be confusing, so teach patients what to look for. (See Reading food labels.)
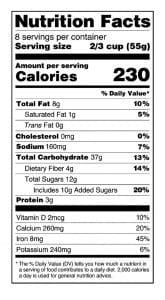
Reading food labels
When counting carbohydrates, patients should learn to read food labels so they can identify the serving size, amount of servings per container, and grams of total carbohydrate. Emphasize that patients should note the grams of carbohydrate not the total daily percentage.
Patients can manage carbohydrate intake using the plate method or by basic or advanced carb counting.
Plate method
The plate method focuses on portion sizes and helps to limit the amount of high-carbohydrate foods on the plate. Instruct the patient to take a 9-inch plate and divide it into three sections. Half of the plate is for non-starchy vegetables (broccoli, carrots, cucumber, lettuce, onion, spinach, tomatoes), one quarter is for a protein, and the other quarter is for a grain or starchy vegetable (acorn squash, corn, green peas, potatoes, yams). For example, half of a plate includes a salad with lettuce, tomato, carrots, and onion; one quarter is baked chicken breast; and the last quarter is white rice. As a visual tool, the plate method can aid portion control, basic carbohydrate counting, and meal planning. If you determine the plate method is best for the patient, notify the provider so they can adjust the medication plan as needed. (See What’s on your plate?)
What’s on your plate?
Managing carbohydrate consumption with the plate method involves dividing a 9-inch plate into three sections, as shown in the illustration below.

Carbohydrate counting
Basic carbohydrate counting requires patients to identify foods with carbohydrates and count the number of carbohydrate servings. Most consistent carbohydrate diets comprise three to five carbohydrate servings in a meal (about 40 to 75 grams) and one to two servings for a snack (about 15 to 30 grams). The patient should be able to identify and plan a meal with the specified number of carbohydrate servings. A patient who receives a fixed meal dose of insulin (for example, 6 units of lispro) should consume a consistent amount of carbohydrate servings per meal to decrease the likelihood of hyper- or hypoglycemia after eating.
Advanced carb counting requires the patient to identify foods with carbohydrates, calculate the amount of carbohydrate (by grams), and use ICR (determined by the provider) to determine the amount of insulin needed to cover the food intake. The provider may need to adjust the ratio over time to match the patient’s clinical needs. ICR (one unit of insulin administered for every “X” amount of carbohydrates in a meal) gives the patient more flexibility with meal timing and the amount of food consumed. For example, if a patient has an ICR of 1:30, they administer 1 unit of insulin for every 30 grams of carbohydrate. So, if the patient eats a meal with 60 grams of carbohydrate, they’ll administer 2 units of insulin. Because the number of grams of carbohydrate varies, the calculation of the ICR may not always result in a whole number. Typically, if the decimal result is less than 0.5, patients round down to the nearest whole number. If the decimal result is greater than or equal to 0.5, they round up to the nearest whole number. If the patient has poor math skills, advise the provider that this may not be a safe option.
When you review Mr. Tucker’s electronic health record, you note that his ICR is 1:15 at breakfast, 1:12 at lunch, and 1:12 at dinner. You determine that he’ll need to learn advanced carbohydrate counting. To assess Mr. Tucker’s ability to use advanced carbohydrate counting, you educate him on the topic and evaluate his math skills using teach back with real-life examples.
Patient education and evaluation
Similar to the nursing process, patient education involves five steps: assessment, goal setting, planning, implementation, and evaluation or monitoring.
Assessment
Start by assessing the patient’s readiness to learn and their baseline knowledge. Does the patient know what a carbohydrate is or what foods contain carbohydrates? Has the patient already been practicing some of the techniques for managing carbohydrate intake, such as avoiding sugary beverages or reading food labels? The answers to these questions will help you and the patient identify personalized learning goals.
Also assess the patient’s food security. The International Food Policy Research Institute defines food security as having the “physical, social, and economic access to sufficient, safe, and nutritious food.” You can teach the correct information, but if a patient can’t apply it to their everyday life, they may feel defeated or give up. Answers to the following questions will help you identify whether the patient needs additional community resources: Does the patient have access to a grocery store with fresh fruits and vegetables? Does the patient receive food primarily from food banks? Is the patient able to buy and prepare their own meals?
After speaking with Mr. Tucker, you learn that he can identify some foods that contain carbohydrates and that he’s been avoiding sodas and sweets. He read food labels for a high school health class but hasn’t been when shopping. He shops for most foods in the grocery store but also eats out with his friends about three times a week.
Goal setting
Next, collaborate with the patient to set goals and help keep them actively engaged throughout the education process.
Working with Mr. Tucker, you determine that he has three goals: successfully reading food labels, determining the total amount of carbohydrate on his hospital tray for each meal, and accurately calculating the amount of insulin with an ICR.
Planning
After setting education goals, plan what content and strategies you want to use and determine what teaching strategies best meet the patient’s learning preferences and health literacy needs. Fleming and Mills identified four main learning styles: visual (pictures, diagrams, handouts), aural (discussion, video), read or write (handouts, pen and paper), and kinesthetic (physical or hands-on activities, return demonstration). Many people learn best using a mixture of methods, but speak with the patient to determine which they prefer.
The U.S. Department of Health and Human Services describes health literacy as the ability to obtain, process, and understand health information to make appropriate decisions. Poor health literacy isn’t solely an inability to read. It also includes difficulty processing numbers and understanding health information. To aid patient comprehension, communicate using simple sentences with common language; avoid medical terminology. You may need to repeat information or include repetitive educational activities to increase retention.
After talking with Mr. Tucker, you establish that he’s primarily a visual learner. He also likes to write notes for himself. You print out patient education handouts about carbohydrate counting for him to read on his own. You also provide him with a pen and blank paper to take notes.
Implementation
Time constraints may be a challenge when providing patient education in the hospital, but every meal provides an opening to actively teach food planning and carbohydrate counting. Start by having the patient discuss which foods on their plate are mainly carbohydrates and which foods are not. This also is an opportunity to look at food portions and how the patient can apply this to their meals at home.
If the patient is learning the plate method, use the food tray to practice dividing the plate into the three sections. Then, ask the patient to categorize the food items as carbohydrate (grain or starchy vegetable), protein, or non-starchy vegetable. If the tray includes a beverage or food item with a food label, point out the amount of carbohydrate per serving and serving size. Then show the patient how to use this information to determine the total grams of carbohydrate in the container. If the patient is learning advanced carbohydrate counting with an ICR, use each meal as an opportunity to practice calculating the amount of insulin they should receive for the meal.
After discussing learning goals with Mr. Tucker in the morning, you begin teaching at lunch. The first goal is reading nutrition labels. You show him the food label on the juice and identify the serving size and total carbohydrate per serving. You also show him how to calculate the total carbohydrates for the container. Mr. Tucker’s second goal is determining the total amount of carbohydrate on his meal tray. Each meal tray arrives with a meal ticket that includes the amount of carbohydrate for each food item. You instruct Mr. Tucker to add up the items he’ll eat. Together, you determine that he’ll have 60 grams of carbohydrate for lunch. Mr. Tucker’s third goal is calculating the amount of insulin he needs using an ICR. You provide him with his lunch ICR (1:12) and then write out and explain the following equation: 60 grams (total grams of carbohydrate) ÷ 12 (carbohydrate ratio) = 5 units of insulin.
Evaluation
After implementing the education plan, the last step is determining if the patient has met the goals and if you need to provide further education. The teach-back method reinforces education and lets you evaluate patient understanding by allowing them to describe in their own words what was taught or demonstrate a skill. Use mealtimes to evaluate if your teaching was successful or if a specific topic needs reinforcement.
At dinner, you evaluate what information Mr. Tucker retained from the education at lunch and what topics need further reinforcement. He looks at his meal ticket and determines that he’s going to be eating 64 grams of carbohydrate. You provide him with the dinner ICR (1:12). He calculates that he’ll need 5.3 units of insulin. He asks, “How do I give myself 0.3 units of insulin?” You first check his meal ticket and determine that he correctly calculated the total amount of carbohydrate on his tray. When you check the ICR against the amount of insulin he calculated, you verify that he’s correct. You then explain that if the decimal is less than 0.5 you round down to the whole unit, and if it’s greater than or equal to 0.5 you round up to the whole unit. For this dinner, he’ll need 5 units of insulin.
After evaluating the patient’s knowledge, reinforce the education throughout the hospital stay and ask if the patient has any additional questions or concerns. In addition, find out whether they need any diabetes supplies or support at discharge. Ask the patient if they have a working glucose meter, testing supplies, and insulin at home, and if they can afford and are able to obtain any needed supplies or medications. Find out if they have a diabetes care provider and if they need a follow-up appointment, an outpatient diabetes education referral, or a home health referral. After this discussion with the patient, notify the provider or the care manager about any needs to ensure a successful discharge.
Positive impact
Carbohydrate counting can aid glycemic control and provide more flexibility for patients with diabetes, but it may be challenging for both nurses and patients. When you gain the knowledge needed to provide patients with comprehensive diabetes education, you can positively impact their self-management skills.
*Name is fictitious.
Arley Henry is a diabetes programmatic nurse specialist at the University of Pittsburgh Medical Center Presbyterian Hospital in Pittsburgh, Pennsylvania.
Patient and nurse resources
Various tools and resources can help patients and nurses with carbohydrate counting. In the in patient setting, nurses can collaborate with registered dietitian nutritionists and certified diabetes care and education specialists for support in teaching and learning about carbohydrate counting, and hospital pharmacists can assist with medication education.
Many websites and mobile apps offer carbohydrate counting materials, guides, and meal-planning tips. In addition, portion control products (such as divided plates and measuring tools) can assist patients with dietary goals.
Websites:
• American Diabetes Association (diabetes.org): Access information about diabetes, risk factors, and resources.
• Association of Diabetes Care and Education Specialists (diabeteseducator.org): This organization is focused on improving prediabetes, diabetes, and cardiometabolic care via innovative education, management, and support.
• U.S. Department of Agriculture (nutrition.gov and choosemyplate.gov): These sites are dedicated to providing credible information to help users make healthy eating choices.
Apps:
• CalorieKing (calorieking.com): Use this large food database to search by brands, fast food chains, or barcode scanning.
• Glucose Buddy (glucosebuddy.com): Track blood glucose readings, insulin, food, and activity throughout the day.
• MyFitnessPal (myfitnesspal.com): Use this app to track food. It can be synched with other fitness apps or devices.
• MySugr (mysugr.com): Access the food database and track blood glucose, meals, and medications
References
American Diabetes Association. The Complete Guide to Carb Counting: Practical Tools for Better Diabetes Meal Planning. 4th ed. Arlington, VA: American Diabetes Association; 2019.
American Diabetes Association. 5. Facilitating behavior change and well-being to improve health outcomes: Standards of medical care in diabetes—2020. Diabetes Care. 2020;43(suppl 1):S48-65. doi:10.2337/dc20-S005
Association of Diabetes Care and Education Specialists. Resources for people living with diabetes.
Blevins S. The art of patient education. MEDSURG Nurs. 2018;27(6):401-2.
Bowen ME, Cavanaugh KL, Wolff K, et al. The diabetes nutrition education study randomized controlled trial: A comparative effectiveness study of approaches to nutrition in diabetes self-management education. Patient Educ Couns. 2016;99(8):1368-76. doi:10.1016/j.pec.2016.03.017
Centers for Disease Control and Prevention. Diabetes meal planning. March 11, 2021.
Centers for Disease Control and Prevention. National diabetes statistics report, 2020. February 11, 2020.
Cornell S, Halstenson C, Miller DK, eds. The Art and Science of Diabetes Self-Management Education. 5th ed. Chicago, IL: American Association of Diabetes Care & Education Specialists; 2020.
Ha Dinh TT, Bonner A, Clark R, Ramsbotham J, Hines S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: A systematic review. JBI Database System Rev Implement Rep. 2016;14(1):210-47. doi:10.11124/jbisrir-2016-2296
Health Resources & Services Administration. Health literacy. August 2019.
International Food Policy Research Institute. Food security.
Krall JS, Donihi AC, Hatam M, Koshinsky J, Siminerio L. The Nurse Education and Transition (NEAT) model: Educating the hospitalized patient with diabetes. Clin Diabetes Endocrinol. 2016;2:1. doi:10.1186/s40842-016-0020-1
University of Wisconsin Hospitals and Clinics Authority. Insulin to carbohydrate ratios (ICRs) (Adult inpatients).
U.S. Food & Drug Administration. Changes to the nutrition facts label. February 10, 2021.

















