Understand your role in patient-centered care.
- The 2022 heart failure management update includes patient-centric recommendations focused on stages, primary prevention, left ventricular ejection fraction classification, pharmacologic management, and comorbidity management.
- The new guidelines place heavy emphasis on primary prevention strategies for patients to Stage A and Stage B heart failure.
- The guidelines highlight the role of nurses in heart failure management.
Learning Objectives
- Explain causes of and risk factors for heart failure.
- Describe how to prevent more severe heart failure in patients with Stages A and B.
- Discuss pharmacologic and comorbidity management of patients with heart failure.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity.
Expiration: 5/1/26
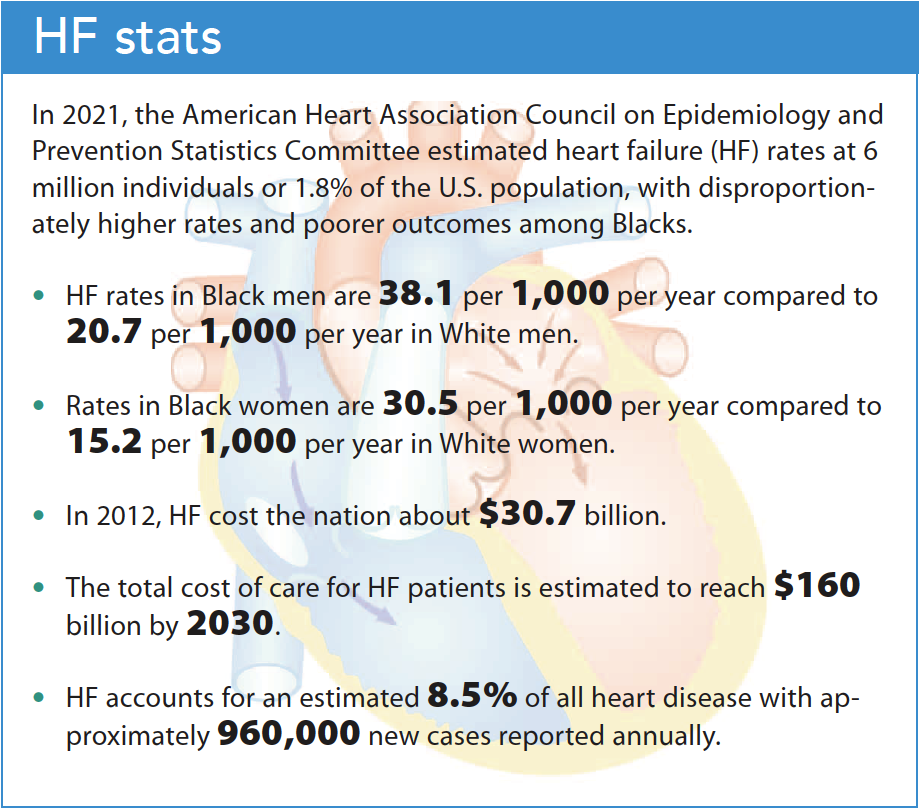
Heart failure (HF) is a clinical syndrome that results from changes in the cardiac structure and leads to impaired ventricular filling or reduced blood ejected with each heartbeat. Primary prevention and management require that nurses have a clear understanding of the causes, risk factors, and pathology of HF as well as their role in patient-centered management based on the 2022 American Heart Association (AHA), the American College of Cardiologists (ACC), and the Heart Failure Society of America (HFSA) guideline for the management of heart failure. (See HF stats.)
Causes and risk factors
According to the 2022 guidelines, HF may be caused by abnormalities in systolic function (failure to pump), diastolic function (elevated filling pressures), or both. Providers use physical assessment findings and typical clinical symptoms to diagnose HF. Clinical findings may include signs of congestion or volume overload, which include increase in body weight, jugular vein distension, shortness of breath on exertion, fatigue, presence of pulmonary congestion found with rales in lung fields on auscultation, and the possible presence of pleural effusion on chest x-ray. Additional physical findings may include peripheral edema, abdominal distention (ascites), and hepatomegaly.
HF risk factors include hypertension, diabetes, age, atrial fibrillation (AF), and obesity. Underlying systemic illnesses or connective tissue disease such as sarcoidosis, lupus, rheumatoid arthritis, scleroderma, and hypothyroidism also can contribute to HF. In addition, cardiotoxic chemotherapy can increase the risk for HF, as does substance misuse with cocaine, alcohol, and methamphetamine.
Pathology
Pathological changes that occur with the reduction of systolic function or cardiac output in HF lead to activation of several compensatory responses to maintain adequate cardiac output. These responses include the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system (SNS). RAAS activation results in vasoconstriction as well as sodium and fluid retention, which initially helps to maintain oxygen perfusion throughout the body, but ultimately results in worsening of HF through exacerbation of cardiac dysfunction and negative remodeling. SNS activation results in increased heart rate and myocardial contractility, which leads to increased stroke volume. Over time, this compensatory mechanism causes increased afterload (pressure that the heart must work against), which worsens HF through negative remodeling and deteriorating left ventricular function.
Patient-centric management
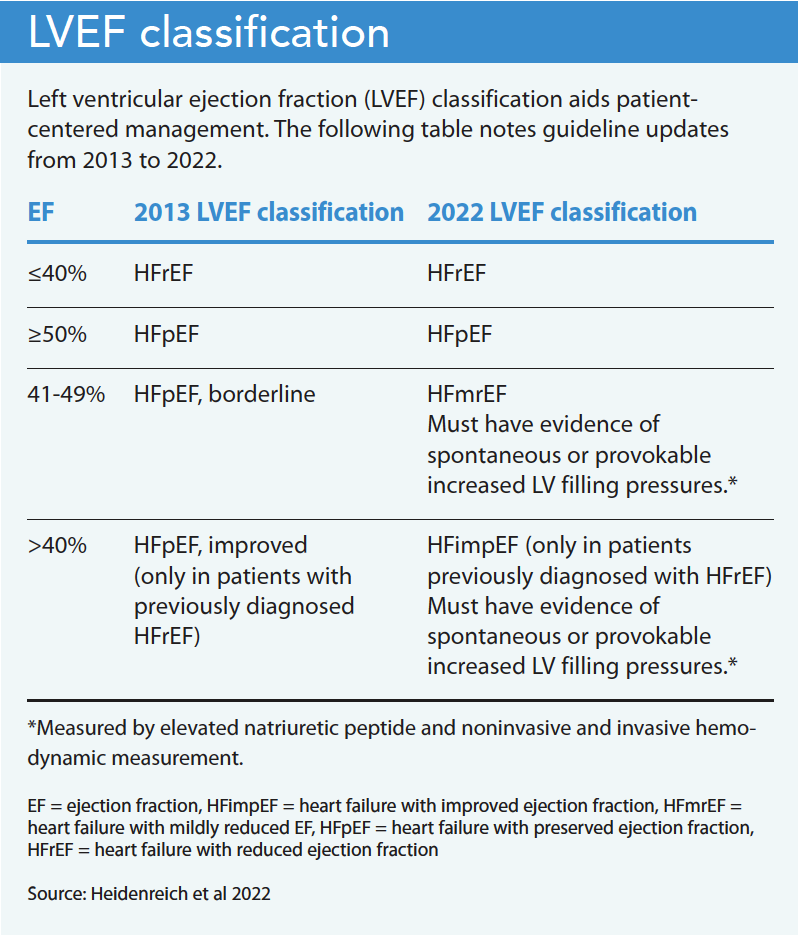
The 2022 HF management update consolidated the 2013 American College of Cardiology Foundation/AHA Guideline for the Management of Heart Failure and the 2017 ACC/AHA/HFSA Focused Update and included patient-centric recommendations. These recommendations focus on HF stages, primary prevention, classification of left ventricular ejection fraction (LVEF), pharmacologic management, and comorbidity management. (See LVEF classification.)
Revised HF stages
Patient-centric recommendations for HF stages focus on using straightforward terminology. Stage A is now called “At risk for HF” as opposed to the 2013 version “At risk for HF but without structural heart disease or symptoms of HF.” Stage B is now referred to as “Pre-HF” rather than “Structural heart disease but without signs or symptoms of heart failure.” Stage C is now called “Symptomatic HF,” and Stage D is “Advanced HF.”
Primary prevention
The new guidelines place heavy emphasis on primary prevention strategies for patients diagnosed with Stage A and Stage B HF.
Stage A. Individuals with Stage A have risk factors for HF, but no symptoms, no structural heart disease, and no evidence of cardiac injury based on cardiac biomarkers. They include those with comorbidities such as hypertension, atherosclerotic cardiovascular disease (CVD), diabetes, metabolic syndrome, and obesity. Others at risk include those with exposure to cardiotoxic agents, a genetic variant for cardiomyopathy, or a positive family history of cardiomyopathy. Primary prevention for these patients focuses on lifestyle habits, including a healthy diet, maintaining regular physical activity, weight management, and smoking cessation. Those with hypertension should strive for a goal blood pressure of <130/80 mm Hg. The guidelines recommend that anyone with type 2 diabetes who has or is at high risk for CVD should use a sodium/glucose cotransporter-2 inhibitor (SGLT2i). Other recommendations include screening at-risk individuals with a natriuretic peptide biomarker (BNP) and calculating risk scores.
Stage B. Patients with Stage B have no HF symptoms, but do have documented structural heart disease, evidence of increased filling pressures, increased BNP levels, or persistently elevated cardiac troponin with no other cause. In addition to implementing all Stage A primary prevention strategies for these patients, the updated guidelines recommend prescribing pharmacologic agents based on the LVEF. If the LVEF is ≤40%, the guidelines recommend an angiotensin-converting enzyme inhibitor (ACEi) and beta blocker. An angiotensin receptor blocker (ARB) may be used in place of an ACEi if the patient is intolerant. If the LVEF is <30% and the patient has more than a 1-year survival rate, the guidelines recommend placing an implantable cardiac defibrillator. Genetic counseling is recommended for anyone with nonischemic cardiomyopathy.
Pharmacologic management
In addition to the pharmacologic management recommendations for Stages A and B HF, the guideline-directed medical therapy for patients with Stages C and D who have HF with reduced ejection fraction (HFrEF) now includes five medication classes: renin-angiotensin system inhibition with angiotensin receptor-neprilysin inhibitors (ARNi), ACEi, or ARB; beta blockers; mineralocorticoid receptor antagonists (MRAs); and SGLT2i. In patients with Stages C and D, ARNi, ACEi, and ARB reduce morbidity and mortality; beta blockers, bisoprolol, carvedilol, and metoprolol succinate reduce mortality and hospitalizations. MRAs (spironolactone and eplerenone) also reduce morbidity and mortality in this population; however, potassium and renal function should be closely monitored due to risk of hyperkalemia and renal insufficiency. SGLT2i, regardless of diagnosis of type 2 diabetes, reduces HF-related hospitalizations and cardiovascular mortality and is recommended for anyone with Stages C and D HF.
Comorbidities
Many patients with HF have comorbidities, including anemia, hypertension, sleep disorders, cardiac amyloidosis, AF, a family history of cardiomyopathy, and cancer being treated with chemotherapy.
Anemia. Anemia can exacerbate HF severity and increase the risk of mortality. Providers diagnose iron deficiency anemia, which is associated with reduced exercise capacity, when ferritin levels reach <100 micrograms per liter. Treating iron deficiency anemia improves patient quality of life and decreases the risk of cardiovascular death and hospitalizations. Several clinical trials have indicated that I.V. repletion of iron provides better outcomes than oral repletion, which has poor absorption. Erythropoietin-stimulating agents are associated with worse long-term outcomes and aren’t recommended for patients with HF who have anemia.
Hypertension. Although the updated guidelines recommend a blood pressure goal of <130/80 mmHg in patients with hypertension, the risk of incident HF significantly decreases with a systolic blood pressure target of <120. Providers should up-titrate antihypertensive medications prescribed for patients with HF to help them reach goal blood pressures.
Sleep disorders. In patients with HF who experience daytime sleepiness, providers should determine whether they have central sleep apnea (CSA) or obstructive sleep apnea (OSA) to inform clinical decision making. CSA is related to a reduction in the respiratory drive from the central nervous system, while OSA is related to a collapse in the pharyngeal airway.
Typical CSA treatment involves adaptive sero-ventilation (ASV); however, this treatment is associated with increased mortality rates in those with HFrEF, so isn’t recommended. Continuous positive airway pressure can be used to treat OSA and CSA and is associated with improved sleep quality and nocturnal oxygenation, making it a preferred option over ASV.
Cardiac amyloidosis. Cardiac amyloidosis in patients with HF can be detected with thorough screening, which includes a detailed history, ECG, echocardiogram, and cardiac magnetic resonance imaging. AHA offers an algorithm for amyloidosis diagnosis and treatment. The presence of monoclonal light chains, which is the most frequent cause of amyloidosis from plasma cell dyscrasias, should prompt providers to refer the patient to hematology and oncology specialists for further treatment and management. In the absence of a monoclonal light chain and the presence of an abnormal technetium-99 m pyrophosphate imaging study (used as a diagnostic tool for cardiac amyloidosis), gene sequencing is recommended, as those with cardiac transthyretin amyloidosis variant disease have an underlying mutation of the TTR gene and may benefit from a referral for genetic counseling and screening for family members.
Providers should individualize treatment for patients with cardiac amyloidosis based on whether the patient has HFrEF. The updated guidelines recommend tafamidis for treating patients with New York Heart Association (NYHA) I–III symptoms (Class I symptoms, no physical activity limitations; Class II, slight limitation; Class III marked limitation). A randomized clinical trial revealed tafamidis had lower all-cause mortality (29.5% vs. 42.9%) and lower cardiovascular-related hospitalizations (0.48 vs. 0.70 per year) compared to other treatment options.
Atrial fibrillation. A complex relationship exists between AF and HF, so anticoagulation should be considered after an individual risk score has been calculated using the CHA2DS2-VASc risk assessment. This score is calculated based on the patient’s age and gender as well as the presence of specific comorbidities, including HF, hypertension, diabetes, history of stroke or transient ischemic attack, and vascular disease. To decrease risk of stroke, oral anticoagulation begins in men with a score of one point or more and in women with a score of two points or more. HF in the presence of AF independently contributes to an increased mortality risk as a result of hypercoagulability.
Cardiomyopathy. The updated guidelines recommend an in-depth family history that includes at least three generations to uncover members with a weak, enlarged, or thick heart. Family members with a history of HF, muscular dystrophy, pacemaker or defibrillator use, or sudden death constitute a positive finding for increased cardiomyopathy risk. Inquiry also should include identifying family members currently on a transplant list or those who’ve had a heart transplant.
Malignancies. Several chemotherapy agents are associated with developing cardiomyopathy and HF. An interprofessional team should evaluate the risk-benefit ratio to determine whether chemotherapy should be continued or temporarily or permanently discontinued. Before initiating chemotherapy, patients at risk for CVD or with known CVD should have their cardiac function evaluated and then monitored at regular intervals throughout treatment. Use of an ACEi, ARB, or beta blocker has shown benefit in preventing drug-induced cardiomyopathy. These medications also help prevent the progression of HF and improve cardiac function in patients with cancer-related cardiomyopathy whose EF is <50%.
Palliative care
The updated guidelines recommend palliative care and management to optimize patient outcomes and end-of-life quality. For patients with advanced HF, particularly Stage D, palliative care aids communication to address prognosis, life-extending therapies vs. treatment discontinuation, symptom management, and hospice. To ensure supportive care as HF advances, the team should present reasonable, individualized treatment options (including advanced directives and goals of care) early.
Self-care
In addition to preventive strategies for Stages A and B HF, the updated guidelines highlight self-care, with extensive discussion related to patients with Stage C. The guidelines recommend using an interprofessional team to screen for and address social determinants of health (socioeconomic status, food insecurity, homelessness or housing insecurity, abuse, limited English proficiency, low health literacy, social isolation, and limited transportation) that may affect self-care. They also recommend evaluating patients for medical barriers, such as cognitive impairment, depression, substance misuse, and frailty that might affect their ability to perform appropriate self-care. Other initiatives include vaccination against respiratory illnesses, including COVID-19 and influenza. Vaccination helps to decrease all-cause and cardiovascular mortality as well as all-cause, cardiovascular, and respiratory illness in this population.
Nursing implications
The updated HF management guidelines reference nurses nine times. For example, the guidelines note the role of the nurse in patient education about medication adherence and healthy lifestyle behaviors, which, when combined with other interventions, can help reduce asymptomatic LV dysfunction. Nurse-led support for patients with HF who experience depression can improve self-care, which leads to improved clinical outcomes. In addition, nurses have successfully coached patients in restricting their daily dietary sodium intake to 2 to 3 g per day, resulting in improved function and decreased leg edema. Nurses also play a significant role in evaluating patients for LV assistive devices when HFrEF becomes too advanced for less invasive interventions.
When nurses organize or take part in care coordination, case management, and early post-discharge follow-up, all-cause mortality and re-hospitalization rates decrease. Nurses are invaluable members of the interprofessional team caring for patients with HF at any stage.
The authors work at the University of Louisiana at Lafayette College of Nursing and Health Sciences. Deedra Harrington is interim department head and full professor/graduate faculty. Christy McDonald Lenahan is graduate coordinator. Robin Beacom is senior coordinator.
American Nurse Journal. 2023; 18(5). Doi: 10.51256/ANJ052306
References
Akbarian S, Ghahjaverestan NM, Yadollahi A, Taati B. Distinguishing obstructive versus central apneas in infrared video of sleep using deep learning: Validation study. J Med Internet Res. 2020;22(5):e17252. doi:10.2196/17252
Cunha JP. What does CHADS score mean? emedicinehealth.com/what_does_chads_score_mean/article_em.htm
Heart Failure Society of America. Heart failure facts & information. hfsa.org/patient-hub/heart-failure-facts-information
Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):10-1161. doi:10.1161/CIR.0000000000001063
Heidenreich PA, Fonarow GC, Opsha Y, Sandhu AT, Sweitzer NK, Warraich HJ. Economic issues of heart failure in the United States. J Card Fail. 2022;28(3):453-6. doi:10.1016/j.cardfail.2021.12.017
Jarvis S, Saman S. Heart failure 1: pathogenesis, presentation and diagnosis. Nursing Times. 2017;113(9):49-53.
Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics—2021 update. Circulation. 2021;143(8): e254-743. doi:10.1161/CIR.0000000000000950
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A Report of the American College of Cardiology
Foundation/American Heart Association task force on practice guidelines. Circulation. 2013;128(16):1810-52. doi:10.1161/CIR.0b013e31829e8807
Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017; 70(6):776-803. doi:10.1016/j.jacc.2017.04.025
Key words: heart failure, guidelines, heart failure management, patient-centered care

















5 Comments. Leave new
I thoroughly enjoyed reading the article. Thanks so much.
There have been so many advances in the identification of heart disease and heart failure over the last fifty years. Knowing more about this evolving clinical area can improve quality of life for patients and family members.
I would like to add that there is a specialty organization which focuses on “the professional development and the advancement of nurses as leaders in cardiovascular disease prevention and management.” It is the Preventive Cardiovascular Nurses Association (PCNA).
Very good
this article is very informative
I can definitely benefit from the information provided in this article. Thank you.
This article was very information with a lot of updated information.