Your knowledge can help eradicate the disease.
- The World Health Organization, the Centers for Disease Control and Prevention, and the European Association of the Study of Liver endorsed simplified treatment pathways to reach the goal of eradicating hepatitis C by 2030.
- The United States Preventative Services Task Force recommends that all adults between the ages of 18 and 79 be tested once, using an anti-HCV blood test, regardless of risk. Other populations may require more frequent screening.
- The development of protease inhibitors as part of an antiviral regimen revolutionized treatment and rendered HCV not only treatable, but curable with direct-acting antivirals.
In October 2021, the Infectious Diseases Society of America (IDSA) and the American Association for the Study of Liver Diseases (AASLD) updated their hepatitis C virus (HCV) guidelines with simplified pathways to extend treatment options and help providers remove barriers and accelerate virus eradication. In June 2022, the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and the European Association of the Study of Liver endorsed these simplified treatment pathways to reach the goal of eradicating HCV by 2030. Your knowledge of HCV and the new guidelines can help ensure treatment adherence and aid HCV eradication.
HCV transmission
HCV, one of several strains of the hepatitis virus that infect the liver, spreads via contact with infected blood. Currently, individuals who share needles are the highest risk group for transmission. Other risk groups include men who have sex with men and infants born to infected mothers. Less commonly, sexual activity with an infected person or contact with their personal effects (for example, razors) can transmit HCV. Other links to the spread of HCV include contaminated instrumentation in healthcare (including dialysis) and community (including tattooing tools) settings.
Acute to chronic infection
When an individual becomes infected with HCV, they enter the acute stage and the body’s immune response begins fighting the virus. This typically occurs during the first 6 months of infection. Estimates indicate that fewer than half of infected individuals will clear the virus on their own and that it will progress into a chronic infection.
HCV prevalence
The incidence of HCV has increased fourfold over the past decade. In the United States, between 2.4 million and 4.7 million individuals have been infected; over half are unaware of their infection. Those in their 20s and 30s make up the fastest-growing group, secondary to I.V. drug use. Before the influx of HCV infection among those who use I.V. drugs, Baby Boomers (those in their late 50s to 70s) experienced the highest incidence of HCV infection. These groups, at about 36% each, account for 72% of HCV cases. Adults in their late 30s to early 50s have the lowest incidence of HCV infection (about 23%), and the remaining 5% comprise individuals under age 18 and over age 80. Children make up a small percentage of those infected with HCV.
Signs and symptoms
Many adults infected with HCV experience no symptoms. Those who develop symptoms typically do so between weeks 2 and 12, and symptoms may last up to 26 weeks. They include abdominal pain, nausea, vomiting, clay or light-colored stools, fever, fatigue, loss of appetite, jaundice, dark-colored urine, and joint pain. Most infected children are asymptomatic or have nonspecific symptoms, such as mild abdominal pain, which makes diagnosing the virus difficult. Many children with HCV have chronic disease.
Complications
Untreated HCV can lead to serious complications, including significant scarring of the liver tissue and cirrhosis. Scarred or cirrhotic liver tissue disrupts blood flow and function, which may result in liver cancer or liver failure. Although early HCV treatment decreases the risk, the infection increases an individual’s overall lifetime risk of developing liver cancer.
Other rare co-morbidities associated with HCV include diabetes, glomerulonephritis, and non-Hodgkin lymphoma. HCV infection can increase the risk for diabetes by altering normal glycogen production and storage in the liver, which leads to enlargement and increased insulin resistance. Cryoglobulinemia, an abnormal blood protein caused by viruses and seen primarily with HCV infections, causes blood thickening and vascular damage, which has been linked to nephropathies, with the most common being glomerulonephritis. Cryoglobulinemia also has been linked to non-Hodgkin lymphoma, a rare complication of HCV in which the virus causes an autoimmune response within the B cells, prompting a lymphoproliferative response that leads to B cell–mediated non-Hodgkin lymphoma.
Screening recommendations
 The United States Preventive Services Task Force recommends that all adults between the ages of 18 and 79 be tested once, using an anti-HCV blood test, regardless of previously defined risk. For those at increased risk, recommendations include more frequent screening. However, no specific guidelines have been established to address frequency. The CDC suggests that anyone who asks for testing should be given the opportunity, even in the absence of risk factors.
The United States Preventive Services Task Force recommends that all adults between the ages of 18 and 79 be tested once, using an anti-HCV blood test, regardless of previously defined risk. For those at increased risk, recommendations include more frequent screening. However, no specific guidelines have been established to address frequency. The CDC suggests that anyone who asks for testing should be given the opportunity, even in the absence of risk factors.
The CDC recommends increased screening for several groups, including pregnant women, who may not report drug use out of fear of being judged or losing custody of their unborn child. However, those who are infected may transmit HCV perinatally. Any child born to a woman who tests positive for HCV also should be tested. Since the transmission rate is approximately 5% for pregnant women infected with HCV and higher in those with a confirmed diagnosis of HIV, the CDC now recommends that all pregnant women receive testing during each pregnancy.
The CDC also advises testing for anyone with a history of injecting drugs, regardless of age; those who continue to inject drugs should be tested regularly. Other groups that should be tested include individuals diagnosed with HIV or those at increased risk for acquiring HIV; those who received blood from a known HCV positive donor; those who received blood, blood products, or an organ transplant before July 1992; and anyone who has received or is now undergoing dialysis. Healthcare workers who’ve been exposed to blood from an infected patient also should be tested. (See HCV screening.)
Treatment
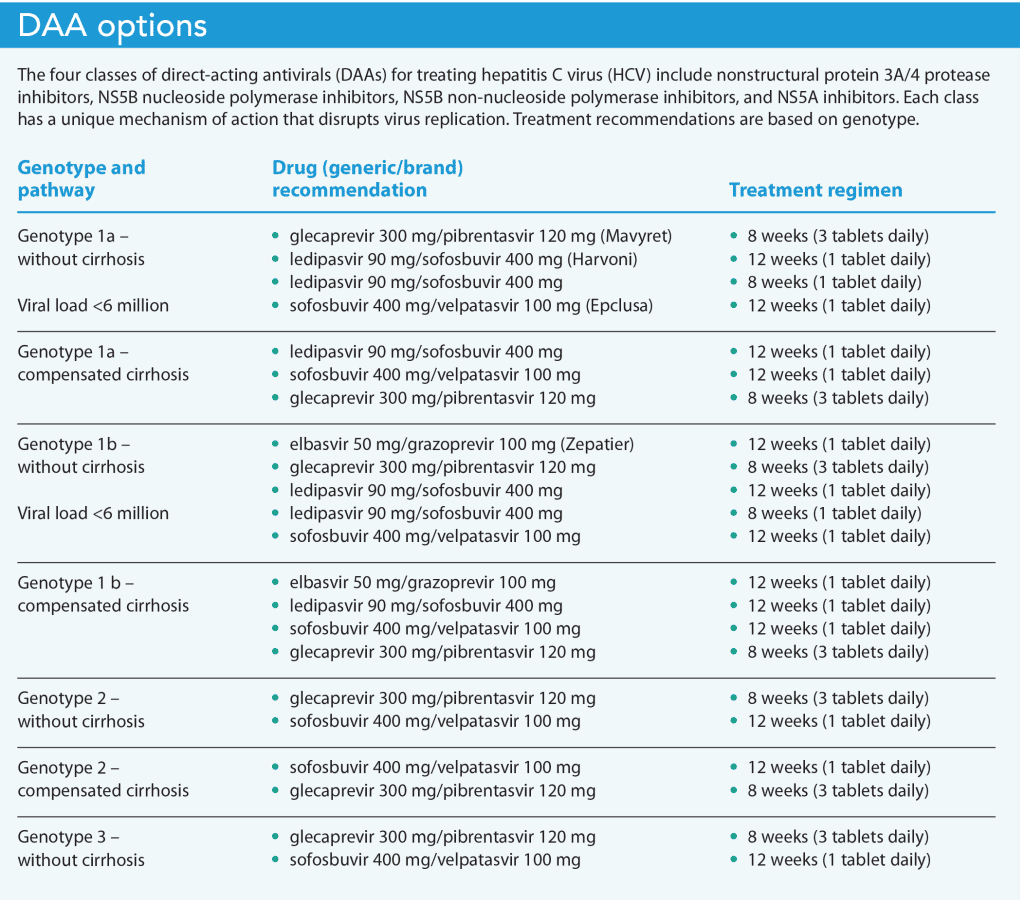
Historically, patients have received treatment from an infectious disease specialist in coordination with a gastroenterology specialist using injected interferon-alpha and daily oral ribavirin. The 24- to 48-week treatment time and undesirable side effects resulted in low adherence. In 2011, the development of protease inhibitors as part of the antiviral regimen revolutionized treatment and rendered HCV not only treatable, but curable with direct-acting antivirals (DAA). These oral medications have simple dosing, provide greater tolerance, result in fewer side effects, and require less than 12 weeks of treatment. About 10 years after DAA treatment development, the updated guidelines and simplified pathways were introduced by IDSA and AASLD. (See DAA options.)
Patient eligibility
Studies indicate that antiviral regimens can help reduce all-cause mortality in individuals infected with HCV, making it beneficial for most to receive treatment. However, the new pathways aren’t recommended for those who have a history of HIV or hepatitis B virus (HBV) coinfection, liver transplant, or cirrhosis. They’re also not recommended in patients with known or suspected hepatocellular carcinoma or those who are pregnant. These individuals should seek treatment with a gastroenterology or infectious disease specialist to ensure close monitoring. The only exclusion for HCV treatment is a life expectancy of less than 12 months related to a comorbidity other than HCV-related liver damage.
Before beginning treatment
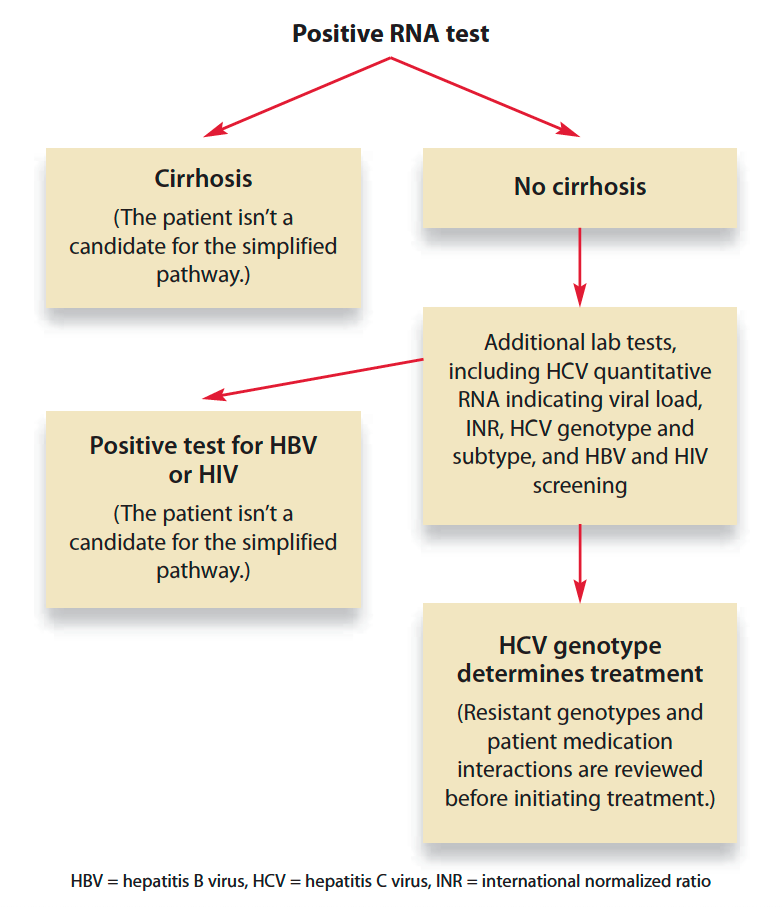
After a positive RNA test for acute or chronic HCV infection, the provider must determine if the patient has cirrhosis. The gold standard is a liver biopsy, but the provider also can use a liver ultrasound or FIB-4 test. The FIB-4, a noninvasive calculation, requires a hepatic panel and complete blood count to determine the ratio of a person’s age, alanine transaminase, aspartate aminotransferase, and platelets. A FIB-4 result of >3.25 indicates severe fibrosis related to cirrhosis and excludes the patient from the simplified pathways.
For patients who meet the criteria for treatment inclusion, a battery of lab tests (HCV quantitative RNA indicating viral load, international normalized ratio [INR], HCV genotype and subtype, and HBV and HIV screening) help determine the best treatment option. If pangenotypic DAA is used, HCV genotype and subtype testing may not be necessary. An assay for resistant viral strains can help determine appropriate treatment for patients with genotype 1a, 1b, and 3.
Other requirements before beginning treatment include a history of decompensated cirrhosis or severe liver disease and medication reconciliation to identify any drug–drug interactions with the chosen DAA. If necessary, medications may be discontinued or changed before beginning DAA therapy. (See Treatment preparation.)
Treatment preparation
Before participation in the simplified treatment pathway, patients must be screened to determine if they meet the criteria for inclusion.
Treatment monitoring
Although no specific recommended monitoring related to the use of DAAs during treatment exists, providers should individualize follow-up based on a patient’s unique biological, psychological, and social needs. In addition to individualized follow-up, a few disease processes require consideration during treatment. For example, patients with diabetes may experience hypoglycemic events, so provide thorough patient education, including information about possible changes in diabetes drug regimens during DAA therapy. Those prescribed coumadin for clotting disorders require close monitoring of their INR and dosage adjustments as needed. When 12 weeks have passed after completing therapy, the provider should order a quantitative HCV RNA test to determine sustained virologic response, which if not detectable, indicates an HCV cure. These individuals should resume screening as appropriate for normal risk of HCV.
Treatment challenges
Reduced duration for DAA therapy has eliminated one of the biggest challenges related to HCV treatment, but obstacles still exist. For example, many patients who use I.V. drugs may be unhoused, which makes continuing therapy difficult. Treating other at-risk populations, including incarcerated individuals and men who have sex with men, also presents challenges. The IDSA and AASLD recommend providing treatment programs within communities, in collaboration with mental health professionals, and in correctional facilities to connect with individuals where they live, which can help ensure treatment adherence.
Play your part
Your role in the care of patients with HCV includes screening and risk assessment; communication of test results; treatment monitoring; and patient education regarding the virus, its potential complications, treatment options, and outcomes. Develop a strong foundational knowledge of HCV, and play your part in eradicating the virus.
Christi Callahan, Carey Cole, and Wendy Downey serve as faculty at Radford University in Radford, Virginia.
American Nurse Journal. 2023; 18(10). Doi: 10.51256/ANJ102312
References
American Association for the Study of Liver Diseases and Infectious Disease Society of America. HCV guidance: Recommendations for testing, managing, and treating hepatitis C. hcvguidelines.org
Centers for Disease Control and Prevention. Know more hepatitis. August 15, 2022. cdc.gov/knowmorehepatitis/hcp/
Centers for Disease Control and Prevention. Testing recommendations for hepatitis C virus infection. July 13, 2023. cdc.gov/hepatitis/hcv/guidelinesc.htm
Chopra S. Clinical manifestations and natural history of chronic hepatitis C virus infection. February 15, 2023.
Pockros PJ. Direct-acting antivirals for the treatment of hepatitis C virus infection. UpToDate. April 2, 2021. uptodate.com/contents/direct-acting-antivirals-for-the-treatment-of-hepatitis-c-virus-infection
Stone R. Pregnant women and substance use: Fear, stigma, and barriers to care. Health Justice. 2015;3(2). doi:10.1186/s40352-015-0015-5
U.S. Preventive Services Task Force. Hepatitis C virus infection in adolescents and adults: screening. March 2, 2020. uspreventiveservicestaskforce.org/uspstf/document/RecommendationStatementFinal/hepatitis-c-screening
U.S. Preventive Services Task Force. Screening for hepatitis C virus infection in adolescents and adults: US Preventive Services Task Force recommendation statement. JAMA. 2020;323(10):970-5. doi:10.1001/jama.2020.1123
World Health Organization. WHO publishes updated guidance on hepatitis C infection – with new recommendations on treatment of adolescents and children, simplified service delivery and diagnostics. June 24, 2022. who.int/news/item/24-06-2022-WHO-publishes-updated-guidance-on-hepatitis-C-infection
Key words: hepatitis C, HCV, HCV transmission, HCV screening, direct-acting antivirals


















