These pacemakers provide an alternative for those who don’t respond to other devices.
Takeaways:
- His bundle pacing offers a superior alternative to the potential adverse effects of pacing from the right ventricular apex.
- For patient with heart failure who don’t respond to biventricular pacemakers, His bundle pacing may offer an opportunity to achieve synchrony.
- Basic nursing care for patients receiving a His bundle pacemaker is similar to nursing care for other pacemakers.
For patients with sick sinus syndrome and nonreversible atrioventricular (AV) conduction block, pacemakers provide the only effective treatment by electrically stimulating heart muscle contraction. Over the years, pacemakers have evolved from those that stimulate the right ventricle at a fixed rate to biventricular devices that promote synchronous heart contractions. His bundle pacing, the most recent pacemaker development, avoids some of the adverse effects of chronic right ventricular pacing and offers a treatment alternative for patients who don’t respond to biventricular pacing.
Normal electrical conduction
Normal electrical conduction supports synchronous muscle contraction and optimizes cardiac output. Conduction starts with an impulse in the sinus node that is transmitted through the atria to the AV node. From the AV node, the impulse is conducted through bundle of His, right and left bundle branches, and then to the Purkinje fibers. (See Electrical conduction: Normal path).
Electrical conduction: Normal path
The illustration below demonstrates normal cardiac electrical conduction.
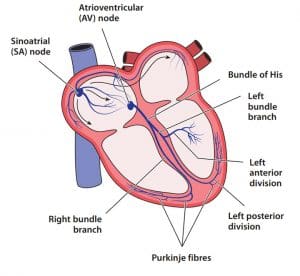
The electrical stimulation of the atria to the ventricles provides for contraction of the atria milliseconds before the ventricles, which allows the atria to empty blood into the ventricles before they contract. If AV synchrony is compromised, the volume of blood emptied into the ventricles decreases, resulting in reduced stroke volume and cardiac output.
Synchrony disruption
Structural changes in the heart—such as cardiomegaly and valvular heart disease—can prevent synchrony and lead to heart failure. Scarring from a myocardial infarction or sarcoidosis may force electrical stimulation to alter its normal course. In addition, abnormal electrical conduction, such as frequent premature ventricular contractions or bundle branch blocks, can change the coordinated stimulation of the heart muscle and prevent synchrony.
Pacemaker evolution
Pacemakers help maintain electrical stimulation of the heart, but they may not maintain the normal electrical conduction that supports synchrony. Technology developments have improved the ability of a pacemaker to support normal conduction. (See Pacemaker history.)
Pacemaker history
Since the 1950s, pacemakers have been evolving to improve outcomes.

1950s – Placement of the first pacemaker. Regardless of the patient’s underlying rhythm, a single lead was placed in the right ventricle with a fixed pacing rate.
1970s – Dual-chamber pacemakers provide a second lead in the right atrium. Manufacturers develop pacemakers that can sense intrinsic conduction, and external programming emerges.
1980s – Rate responsiveness arrives. Pacemakers sense the patient’s activity and adjust the pacing rate as needed.
2000s – Patients with heart failure receive biventricular pacemakers. The addition of a left ventricular lead promotes synchrony.
2018 – The U.S. Food and Drug Administration approves a pacemaker lead to stimulate the His bundle.
Right ventricular pacemakers
Right ventricular pacemakers work by sending electrical impulses from the apex of the right ventricle, rather than from the His bundle through the left and right bundles to the Purkinje fibers. This changes the electrical activation pattern in both the left and right ventricles, which alters the muscle activation pattern. Instead of ventricular synchrony, the resulting less-effective contraction reduces cardiac output. Eventually, frequent pacing from the right ventricular apex remodels and weakens the ventricles, leading to heart failure.
These potential adverse effects have changed pacing recommendations. The 2018 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines on the evaluation and management of patients with bradycardia and cardiac conduction delay recommend that patients who require ventricular pacing at least 40% of the time receive it in a manner that maintains “physiologic ventricular activation” (normal conduction pattern) rather than from the right ventricle apex.
Biventricular pacemakers
Biventricular pacemakers, also known as cardiac resynchronization therapy, were designed to restore synchrony. They avoid asynchronous pacing by adding a lead in the left ventricle, which typically is placed through the coronary sinus. (See Biventricular pacemakers.)
Biventricular pacemakers
This biventricular pacemaker includes three leads: one in the left atrium, one in the right ventricle, and one in the left ventricle via the coronary sinus vein.
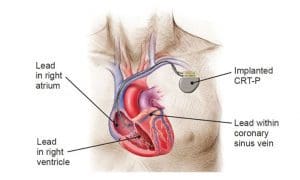
Image provided courtesy of Boston Scientific. ©2020 Boston Scientific Corporation or its affiliates. All rights reserved.
Coordinated electrical stimulation timing facilitates the atria emptying into the ventricles for AV synchrony. Coordinated timing between the right and left ventricles ensures synchronous ventricular contraction. In their review of landmark clinical trials, Chatterjee and Singh reported that for patients with heart failure, cardiac resynchronization therapy has resulted in decreased symptoms, increased functional capacity, reduced hospitalizations, and improved survival.
Biventricular pacemakers offered new hope for patients with heart failure by improving cardiac output. Unfortunately, not all patients achieve the synchrony needed to improve heart failure symptoms and reduce disease progression. In fact, over a third of patients who have received a biventricular pacemaker are non-responders.
Tracy and colleagues describe the characteristics (including lack of a left bundle branch block) of patients likely to be non-responders. A left bundle branch block reflects prolonged activation of the left ventricle, which results in a prolonged QRS duration (>100 msec). The lead in the left ventricle can shorten activation, which promotes synchrony between the left and right ventricles. After implanting a biventricular pacemaker in patients with a left bundle branch block, the QRS should shorten to a duration closer to normal.
For patients with heart failure who don’t have a left bundle branch block, no opportunity exists for the lead in the left ventricle to shorten the activation time and promote synchrony. These patients are less likely to experience improved cardiac output from a biventricular pacemaker. His bundle pacemakers provide them with an alternative approach.
His bundle pacing
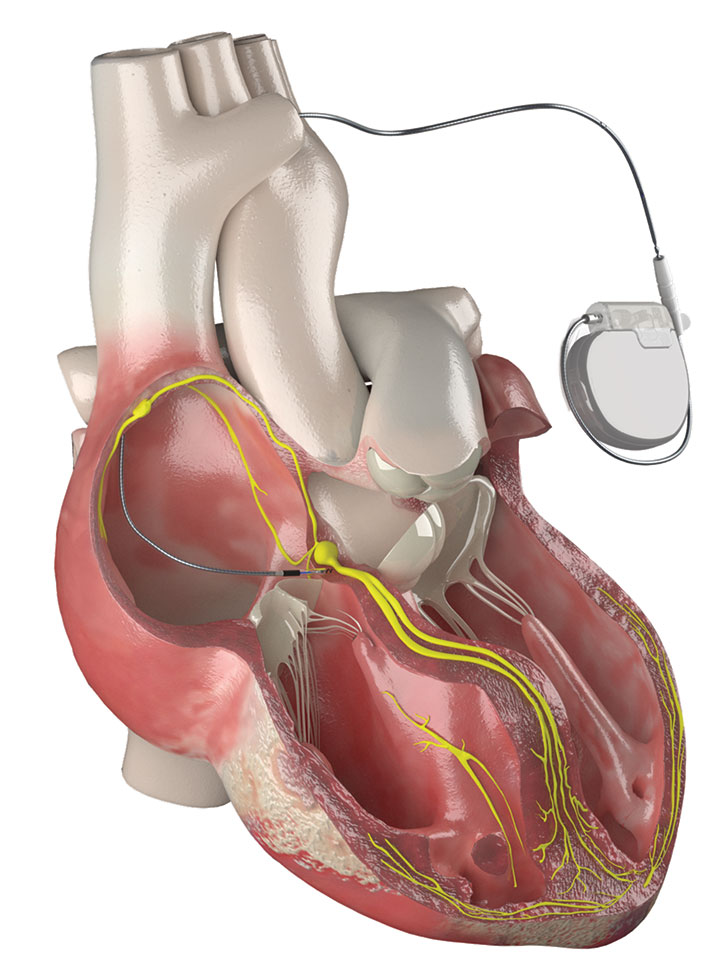
The first His bundle pacemakers were implanted in humans between 1995 and 1997. Patients showed significant improvement in heart size and heart function. Since then, many have viewed His bundle pacemakers as a superior alternative to right ventricular pacing. In a clinical trial of 765 patients, Abdelrahman and colleagues compared outcomes between those who received right ventricular pacemakers and those who received His bundle pacemakers. Patients with His bundle pacemakers had a significant decrease in mortality and heart failure hospitalizations. (See His bundle pacemaker.)
Challenges
Implanting His bundle pacemakers presents several challenges. For example, the His bundle is more difficult to locate than the apex of the right ventricle, which can be identified with fluoroscopy. The ideal His bundle lead placement sites are much smaller (about 2 mm) and require electroanatomic mapping to identify. The cardiologist must view QRS morphologies at multiple sites to determine the best option. (See His bundle placement.)
His bundle placement
The image below shows the pacing lead placed in the penetrating portion of the His bundle (PHB—the region of the His bundle that penetrates the fibers of the heart.). The right bundle branch (RBB) and the left bundle branch (LBB) emerge from the branching portion (BHB). To visualize the placement site, the cardiologist has separated the membranous septum (MS) from the top of the ventricular septum.
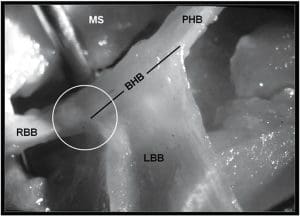
Figure provided by Dr. Marcelo V. Elizari. Used with permission.
These challenges lengthen the time of the implantation procedure. However, as leads and delivery catheters evolve, His bundle lead placement will likely improve.
Selective and nonselective pacing
His bundle pacing can be selective (direct activation of the His bundle) or nonselective (indirect activation). In selective pacing, the lead is placed in the His bundle itself. In nonselective pacing, heart tissue near the septum is stimulated, capturing both the myocardium and the His bundle, which creates a delta wave. No clear consensus exists on which is the most effective modality.
Nursing care
Nursing care for patients who receive a His bundle pacemaker is similar to that for patients who receive other types of pacemakers, including monitoring pacemaker function after placement and providing patient education.
Pacemaker monitoring. For patients on telemetry or an ECG, you can easily determine His bundle pacemaker function by checking for sensing and capture. Sensing is the pacemaker’s ability to detect intrinsic activity and withhold pacing. Capture is the pacemaker’s ability to pace, which results in the planned response in the heart.
Pacing spikes appear as small vertical lines on the ECG when the pacemaker stimulates the conduction system. For a His bundle pacemaker, this spike will occur just before the QRS complex. Capture takes place when a QRS follows the spike. In the nonselective mode, the delta wave extends and widens the QRS complex. (To view ECG images of His bundle pacing, visit ahajournals.org/doi/10.1161/JAHA.118.010972).
Patient education. Focus patient education on identifying signs of infection, incision care, activity restrictions, and follow-up.
Instruct patients to refrain from touching the incision, to monitor themselves for fever, and to check the incision daily for signs of discharge, swelling, and redness. If any of these signs occur or if incisional discomfort resolves and then returns, the patient should contact their provider immediately to determine if the incision is infected. When identified early, an infection can be treated with antibiotics. If not, the device and leads may require removal and then replacement after the infection resolves.
Most pacemaker incisions are closed and covered with nonadhesive wound dressing strips or surgical glue. For incisions covered with surgical glue, instruct patients to avoid showering for 1 to 2 days; for incisions covered with nonadhesive strips, instruct them to avoid showering for 4 to 5 days. The incision shouldn’t be submerged in water, such as during swimming, for several weeks.
Activity restrictions after pacemaker placement have changed with the development of leads that can be screwed into the heart tissue and are less likely to dislodge with activity. Traditionally, patients kept the arm on the pacemaker side in a sling for several days. This shoulder immobilization sometimes resulted in adhesive capsulitis (frozen shoulder). With more stable leads, many providers don’t require slings. However, patients should avoid lifting more than 10 pounds and refrain from participating in activities that involve vigorous arm and shoulder movements, such as golf or tennis, for several weeks.
Help patients schedule follow-up appointments to assess the incision and the pacemaker. Emphasize the importance of keeping these appointments to identify potential infections and other issues with the pacemaker.
A significant difference
In terms of nursing care, His bundle pacemakers aren’t much different from other pacemakers. In terms of function, however, they differ significantly from traditional pacemakers. By providing physiologic pacing, His bundle pacemakers prevent the potential adverse effects of pacing from the right ventricular apex and can help restore synchrony to patients with heart failure who likely wouldn’t improve with biventricular pacing.
Nancy Cash is a clinical instructor at Rutgers University School of Nursing in Blackwood, New Jersey.
References
Abdelrahman M, Subzposh FA, Beer D, et al. Clinical outcomes of His bundle pacing compared to right ventricular pacing. J Am Coll Cardiol. 2018;71(20):2319-30. doi:0.1016/j.jacc.2018.02.048
Burri H, Keene D, Whinnett Z, Zanon F, Vijayaraman P. Device programming for His bundle pacing. Circ Arrhythm Electrophysiol. 2019;12(2):e006816. doi:10.1161/CIRCEP.118.006816
Chatterjee NA, Singh JP. Cardiac resynchronization therapy: Past, present, and future. Heart Fail Clin. 2015;11(2):287-303. doi:10.1016/j.hfc.2014.12.007
Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay. Heart Rhythm. 2019;16(9):e128-226. doi:0.1016/j.hrthm.2018.10.037
Lewis AJM, Foley P, Whinnett Z, Keene D, Chandrasekaran B. His bundle pacing: A new strategy for physiological ventricular activation. J Am Heart Assoc. 2019;8(6):e010972. doi: 10.1161/JAHA.118.010972
Naqvi TZ, Chao C-J. Adverse effects of right ventricular pacing on cardiac function: Prevalence, prevention and treatment with physiologic pacing. Trends Cardiovasc Med. 2021:S1050-1738. doi:10.1016/j.tcm.2021.10.013
Orlov MV, Koulouridis I, Monin AJ, et al. Direct visualization of the His bundle pacing lead placement by 3-dimensional electroanatomic mapping: Technique, anatomy, and practical considerations. Circ Arrythm Electrophysiol. 2019;12(2):e006801.doi:10.1161/CIRCEP.118.006801
Tracy CM, Epstein AE, Darbar D, et al. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. Circulation. 2012;126(14):1784-1800. doi:10.1161/CIR.0b013e3182618569
Upadhyay GA, Tung R. Selective versus non-selective His bundle pacing for cardiac resynchronization therapy. J Electrocardiol. 2017;50(2):191-4. doi:10.1016/j.jelectrocard.2016.10.003
Vijayaraman P, Dandamudi G. How to perform permanent His bundle pacing: Tips and tricks. Pacing Clin Electrophysiol. 2016;39(12):1298-1304. doi:10.1111/pace.12904
Vijayaraman P, Dandamudi G, Lustgarten D, Ellenbogen KA. Permanent His bundle pacing: Electrophysiological and echocardiographic observations from long-term follow-up. Pacing Clin Electrophysiol. 2017;40(7):883-91. doi:10.1111/pace.13130
Zusterzeel R, Selzman KA, Sanders WE, et al. Cardiac resynchronization therapy in women: US Food and Drug Administration meta-analysis of patient-level data. JAMA Intern Med. 2014;174(8):1340-8. doi:10.1001/jamainternmed.2014.2717

















